

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Uterine leiomyoma is the most common benign tumor of the female genital tract, affecting approximately 20–50% of all women. Although hysterectomy is an option for the surgical management of uterine leiomyomas, myomectomy is an attractive alternative for women who desire to preserve fertility [12].
Laparoscopic myomectomy (LM) was described in 1979 by Semm [3]; LM has distinct advantages over abdominal myomectomy, including shorter hospital stay, faster recovery, less adhesion, cosmetic advantages, and reduced blood loss [456]. On account of these merits, LM has become a recent trend for the surgical treatment of uterine leiomyoma. With the use of more advanced instruments, such as articulating forceps or barbed suture devices, and increase in the surgeons' experience, surgeons are attempting to minimize the number of abdominal incisions and visible scars; single-port LM (SP-LM) has been introduced and is a rapidly evolving field with this tendency [7891011].
However, technical difficulties are associated with SP-LM when suturing uterine defects because of the collision of instruments, limited number of operating arms, and absence of an assistant arm for maintaining tension. Therefore, barbed suture devices are frequently used during SP-LM procedures because they are easy to use and shorten the operative time [10]. Despite these advantages, the use of residual barbed suture materials has been implicated to cause bowel complications after laparoscopic gynecologic surgery [1213]. Given that bowel complications adversely affect the patients' quality of life, efforts are needed to find alternative suturing methods to repair the uterine defects during SP-LM.
To compensate the limitations of the barbed suture devices, we adopted several modified suture techniques, which included Hem-o-lok clip anchoring, continuous horizontal mattress suturing of the myometrium, and baseball suturing of the uterine serosa in SP-LM (Choi's LM) since 2011 [14]. This retrospective study reported that Choi's LM performed using the modified suture technique was associated with a shorter operative time and less blood loss.
Several studies reported immediate surgical outcomes and provided technical descriptions of the novel suturing technique for SP-LM; in contrast, only a limited number of studies reported the long-term recurrence and pregnancy outcomes of patients who underwent SP-LM.
LM had higher recurrence rate than open myomectomy [15], and a 5-year cumulative recurrence rate of up to 52.9% had been reported after LM [16].
After myomectomy, uterine rupture and dehiscence are among the life-threatening complications that can possibly occur during pregnancy [17]. In this study, we aimed to investigate the long-term outcomes, including pregnancy outcome and recurrence rate, of patients who underwent Choi's LM as treatment for symptomatic uterine leiomyoma and compare these outcomes with those of patients who underwent conventional multi-port LM (4-port LM).
Go to : 
Materials and methods
1. Study population
In October 2011, with 55 patients who underwent 2-port LM, Choi's LM was introduced in SP-LM using a new modified suture technique. This Choi's LM procedure was performed by a single surgeon (CH Choi) who performed over 100 LM procedures per year at Samsung Medical Center.
Patients with <3 symptomatic leiomyoma measuring 10 cm or less on ultrasonography and were eligible for Choi's LM. Patients who fulfilled the inclusion criteria were selected consecutively to undergo this procedure, and data were collected prospectively. The decision to perform this procedure was not influenced by the patient's history of abdominal surgery or type of leiomyoma. Before surgery, the risks were explained to the patient, including the potential need for an additional port during surgery and the risk of uterine rupture in future pregnancies. As a control, all patients who underwent conventional multi-port LM (4-port LM) from January 2008 through November 2010 were included. The inclusion criteria were the same as above.
2. Data collection
The following patient characteristics were obtained: age, body mass index (BMI), parity, symptoms resulting from myomas, location and type of largest myomas, and number and diameter of dominant myomas.
During the long-term follow-up, patients were evaluated via ultrasonography every 6 months for the first year and annually thereafter. Leiomyoma recurrence was confirmed when a new leiomyoma measuring 3 cm or more was detected on ultrasonography. Patients were also asked if they attempted to become pregnant, and all of the obstetric data were collected during the follow-up.
3. Surgical procedure
The Choi's LM procedure was described in our previous study [14]. Briefly, using the open Hasson technique, a 2-cm vertical incision was made within the umbilicus, and an extra-small wound retractor (Alexis; Applied Medical, Rancho Santa Margarita, CA, USA) was inserted into the wound opening. Once it fixed in the opening site, the retractor laterally retracted the sides of the wound opening. A surgical glove with sheaths inserted into 3 fingers was attached to the outer ring of the retractor to maintain pneumoperitoneum.
After enucleation of the leiomyoma, the uterine parenchymal defect was closed laparoscopically in a double layer. A 1-0 Vicryl suture (Polyglactin; Ethicon, Somerville, NJ, USA) on a large curved needle was then used to make a deep and wide bite. Before suturing, the Vicryl suture was tied with a Hem-o-lok clip, which acts as anchor on the tail of the continuous suture and was the starting point of the suture site (Fig. 1A). Basically, all sutures were completed with one continuous suture using a double layer technique. First, a horizontal mattress suture with a deep and wide bite was performed at the bottom of the defect to attach the myometrium closely and for hemostasis (Fig. 1B and C). In the case of large myometrial defects, additional horizontal mattress sutures were performed in a continuous manner. Following the horizontal mattress suture, a baseball suture was performed in the opposite direction to close the myometrium and serosa tightly (Fig. 1D and E). In the baseball suture, the edges of the uterine defect were approximated with introflexion stitches (myometrium/serosa–serosa/myometrium direction) at 1.5-cm increments from the side of the incision and held tightly with articulating grasper to secure tension. After completing the baseball suture, 2 Hem-o-lok clips were applied and pushed with maximal tension to secure the suture (Fig. 1F). The knot was tightly fixed immediately, decreasing the risk of knot loosening during interrupted knot typing. Up to 3 Hem-o-lok clips were used during this procedure.
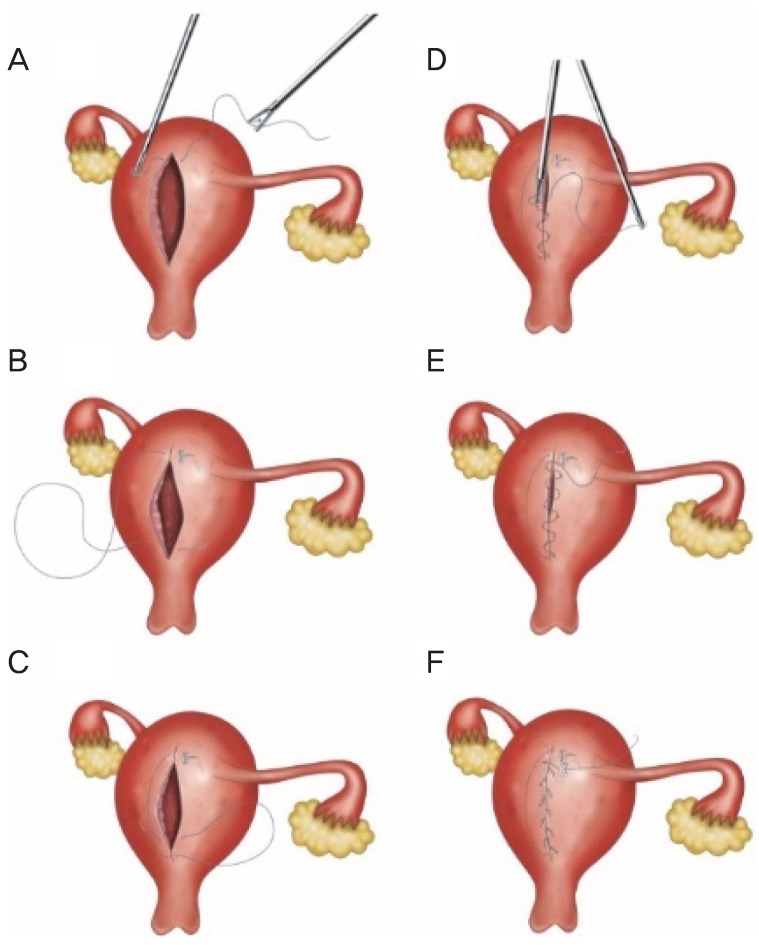 | Fig. 1Single-port laparoscopic myomectomy (LM) with a modified suture technique with a Hem-o-lok clip (Choi's LM). (A) The 1-0 Vicryl suture was tied with a Hem-o-lok clip, which acts as an anchor on the tail of the continuous suture that is the starting point of the suture site. (B, C) A horizontal mattress suture with a deep and wide bite was performed at the bottom of the defect to attach the myometrium closely. (D) A baseball suture was performed in the opposite direction to approximate the myometrium and serosa tightly, while the grasper was used and pushed with maximal tension to cinch down on the last suture site to secure the suture. (E) The same procedures were continuously repeated. (F) The Hem-o-lok clip was used to cinch down on the suture site and secure the knot tightly.
|
If the surgery was difficult to perform on a single-port platform or when prolonged operation was anticipated, the surgeon decided whether to create an additional 5-mm port in the suprapubic area at any time during the surgery. To perform a 2-port LM, a 5-mm ancillary trocar was inserted 2 fingerbreadths above the symphysis pubis. Lastly, the resected leiomyoma was wrapped with an endopouch and removed via the umbilical wound by cutting it into smaller pieces using a knife.
4. Statistical analyses
Descriptive statistics were used to analyze categorical and continuous variables. Continuous variables were compared using the Mann-Whitney U-test or Student's t-test. Fisher's exact test, χ2 test, or logistic regression test was used to analyze categorical variables. Recurrence rates were compared using Kaplan-Meier curve. Statistical analyses were performed using SPSS version 25.0 (SPSS, Chicago, IL, USA). A P-value of ≤0.05 was considered significant, and all P-values were 2 sided.
Go to :
Results
Of 184 patients who underwent Choi's LM and 4-port LM, 27 were excluded because of the size (>10 cm) or number (≥3) of myomas. Of 157 patients who fulfilled the inclusion criteria, 55 underwent Choi's LM and 102 underwent 4-port LM.
The detailed patient demographic data and characteristics of myomas are shown in Table 1. Patients' age, BMI, parity, and symptoms related to myomas were similar in the 2 groups. The mean age of Choi's group was 39.4±6.2 years (range, 27–52 years), while that of the 4-port LM group was 38.6±5.7 years (range, 26–55 years) (P=0.41, respectively). Nineteen patients (34.5%) in the Choi's LM group and 31 (30.4%) in the 4-port LM (P=0.56) were nulliparous. The initial preoperative indications were menorrhagia (40% vs. 45.1%), compression symptoms (38.2% vs. 28.4%), and pelvic pain (20.0% vs. 26.5%).
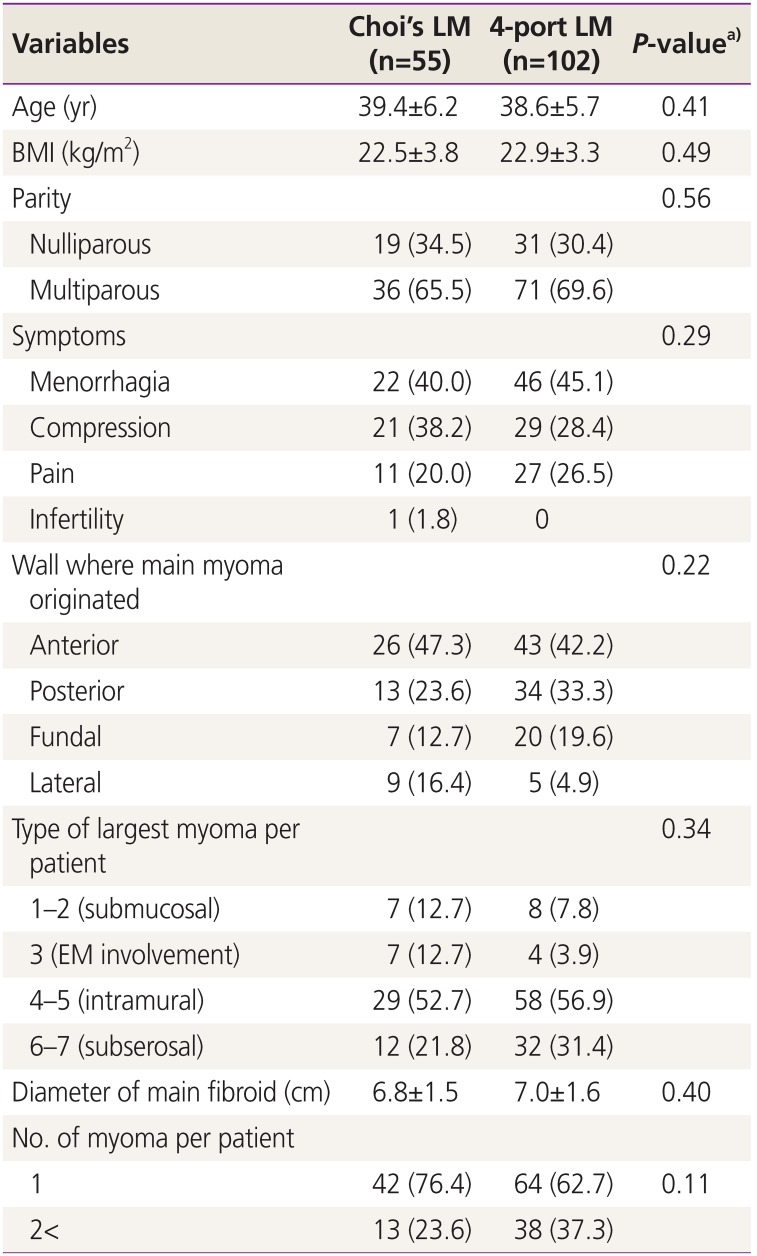
Table 1
Demographic data of the patients in the Choi's laparoscopic myomectomy (LM) and 4-port LM group
Data are shown as mean±standard deviation or number (%).
BMI, body mass index; EM, endometrium.
a)The P-value was determined using χ2 test, Fisher's exact test, or Student's t-test.
![]()
There was no significant difference in the characteristics of the myomas between the 2 groups. Forty-two women (76.4%) in the Choi's LM group and 64 women (62.7%) in the 4-port LM group had a single leiomyoma (P=0.11). The most common type of leiomyoma was intramural type (3–5; 36 [65.4%] vs. 62 [60.8%]), followed by subserosal type (6–7; 12 [21.8%] vs. 32 [31.4%]) and submucosal type (1–2; 7 [12.7%] vs. 8 [7.8%]; P=0.34). For both groups, anterior wall (26 [47.3%] vs. 43 [42.2%]) was the most common location of myomas. Mean diameter of the largest leiomyoma was also similar between 2 groups (6.8±1.5 cm [range, 5.0–9.9 cm] vs. 7.0±1.6 cm [range, 5.0–9.9 cm]), as measured on ultrasonography (P=0.11).
In Choi's LM group, 16 (29.1%) patients required an additional port to achieve meticulous repair of the uterine defect. We compared the clinical factors associated with the need for an additional port. In multivariate analysis (Table 2), clinical factors associated with additional port insertion were diameter of the main fibroid and parity (P=0.04 and 0.023, respectively). Multiparous women did not require an additional port. Type and location of leiomyoma were not associated with the need for an additional port. However, there is a possibility that the cases of patients requiring an additional port were more complicated, which can lead to longer operating time, larger blood loss, and/or longer hospital stay.
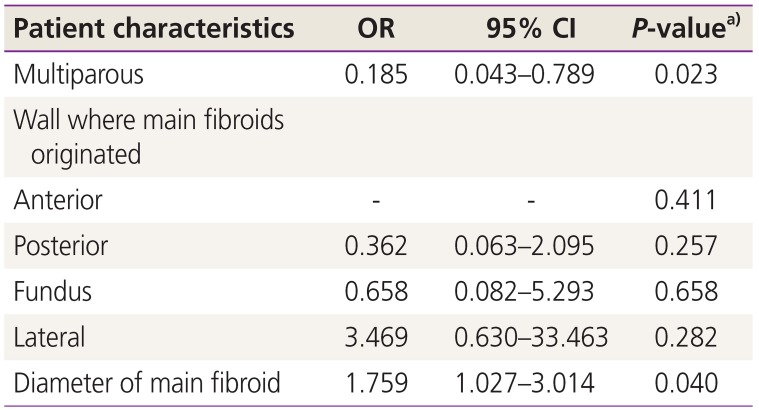
Table 2
Logistic regression results for predicting additional port insertion in Choi's laparoscopic myomectomy
CI, confidence interval; OR, odds ratio.
a)The P-value was determined using Logistic regression test.
![]()
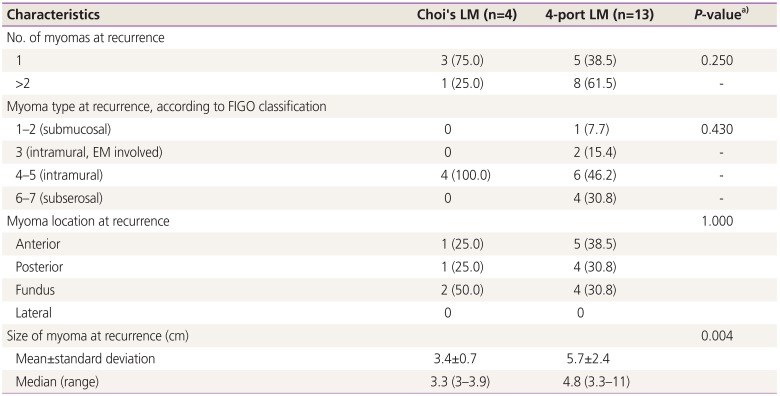
Within a median follow-up of 69 months, 17 patients (4 [7.1%] vs. 13 [14.6%]) had myoma recurrence (P=0.292) (Table 3). In Choi's LM group, most of the patients had solitary-type (4 [75%]) and intramural-type myomas (4 [100%]). In contrast, the 4-port LM group had multiple (8 [61.5%]) and more various types of myomas (P=0.25). The size of dominant myomas at recurrence was significantly smaller in Choi's LM group (3.4±0.7 cm [range, 3.0–3.9 cm] vs. 5.7±2.4 cm [range, 3.3–11.0 cm]; P=0.004). The Kaplan-Meier curve (Fig. 2) showed similar 5-year cumulative recurrence rate in both groups.
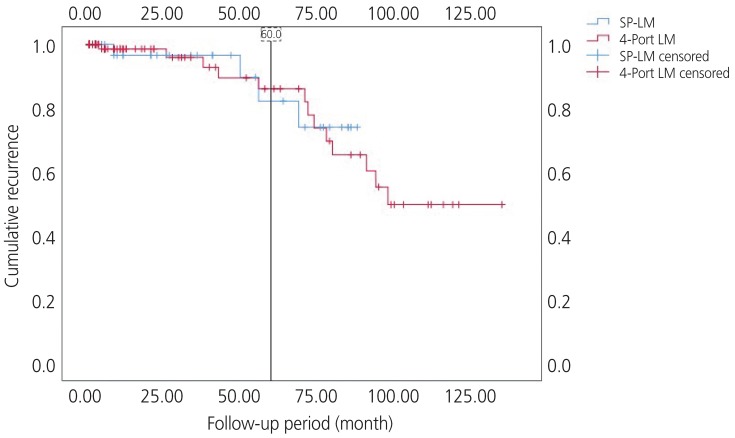 | Fig. 2Kaplan-Meier curve showing similar cumulative recurrence rate (P=0.835). Probability of 5-year recurrence-free survival of patients: Choi's LM (82.2%) vs. 4-port LM (86.0%).SP, single-port; LM, laparoscopic myomectomy.
|
Table 3
Characteristics of recurrence after myomectomy
EM, endometrium; FIGO, Federation of Gynecology and Obstetrics; LM, laparoscopic myomectomy.
a)The P-value are represented as myoma recurrence (P=0.292).
![]()
The pregnancy outcomes of the 2 groups are summarized in Table 4. Four patients in the Choi's LM group and 9 in the 4-port LM group successfully conceived, and all of had full-term delivery. Three patients had 2 pregnancies during the follow-up period. Two patients in the Choi's LM group and 1 in the 4-port LM group had a successful vaginal delivery with no serious complications. They developed the same type of myoma (pedunculated subserosal type 7) before surgery. No major complications (such as uterine rupture or dehiscence) related to LM occurred during pregnancy. No abnormal findings, other than mild adhesion, were reported during cesarean section in both groups.
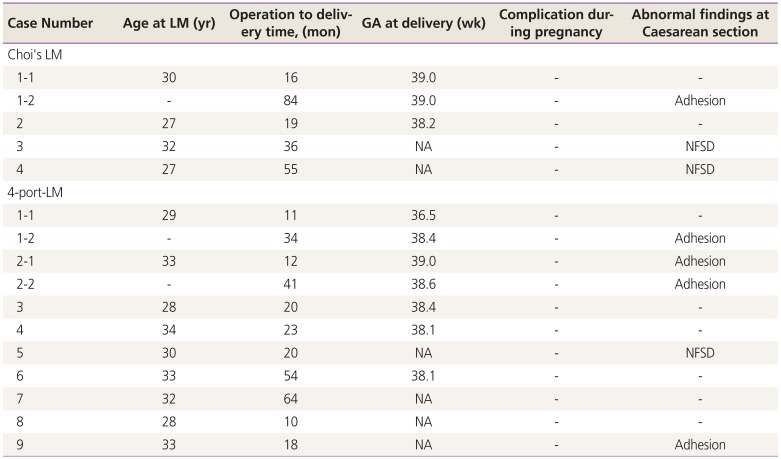
Table 4
Pregnancy outcomes of patients after myomectomy
LM, laparoscopic myomectomy; GA, gestational age; NFSD, normal full-term vaginal delivery; NA, not available (the exact GA was not available if delivered outside).
![]()
Go to :
Discussion
This study suggests that SP-LM using a modified suture technique (Choi's LM) was a possible alternative in selected patients with a symptomatic leiomyoma measuring 10 cm or less and fewer than 3 leiomyomas considering the long-term outcome. Although 16 patients (29.1%) needed an additional port, the perioperative outcomes of this study were comparable to those of previous studies using barbed suture devices for SP-LM [181920].
Patients who were nulliparous and/or had a large leiomyoma were more likely to require an additional port. This result can be explained by the meticulous suturing of the myometrium for nulliparous women. Although cosmetic outcomes and surgical outcomes were important, meticulous suture was more important for nulliparous women who are planning to become pregnant in the future. Myomectomy is a fertility-preserving surgery for nulliparous women but may lead to uterine rupture during pregnancy. Single-layered closure of uterine wall defect and frequent use of electrocautery are risk factors of uterine rupture [17]. Surgeons who perform single-port myomectomy should pay special attention on suturing the myometrium in nulliparous women. Although Choi's LM had no adverse pregnancy outcomes related with the insertion of Hem-o-lok clips in situ, the data used in this study were too insufficient.
Long-term follow-up data of our study showed that the recurrence rate was acceptable compared with that of previous studies [1621]. Two groups had similar patient and myoma characteristics identified as risk factors: age, size of myoma, and number of myoma [16]. Peri- and postmenopausal patients with single myoma had the lowest recurrence rate after undergoing laparoscopy and can be considered as the best candidate for SP-LM [22].
Several studies have reported the benefits of SP-LM. SP-LM provides better cosmetic results because of the relatively hidden umbilical scar [23]. Although 29.1% of patients in this study required an additional port, the port was located at 2 finger widths above the symphysis pubis, alleviating cosmetic concerns. Another possible benefits of SP-LM using the glove technique are as follows: less common subcutaneous emphysema, port-site wound infection, and hemorrhage because of the tamponade effect of the wound retractor [24]. In this study, no wound-related complications, such as hematoma, herniation, or wound dehiscence, were reported. Furthermore, the glove-wound retractor system provided a higher degree of freedom for operative maneuvers, making laparoscopic suturing easier to perform. Additionally, leiomyoma was wrapped in an endopouch and extracted through a trans-umbilical knife morcellation, which lessened the risk of leiomyoma seeding by mechanical morcellation [25].
Despite these advantages, laparoscopic repair of uterine defects through a single port remains arduous and requires greater surgical skill because of the limited of instrument movement. Besides, the quality of uterine defect suture is important in myomectomy considering the perioperative outcomes and future pregnancy. Therefore, in order to reduce tissue ischemia and necrosis, it is crucial to ensure that the tensile strength is evenly distributed over the entire length of the uterine defect. When suturing is insufficient, oozing from the uterine defect, formation of dead space, and subsequent hematoma formation at the incision site increase the risk of postoperative wound infection and adhesion [2627]. Recently, barbed suture devices have been widely used in minimally invasive surgery because they allow continuous wound closure with even distribution of tensile strength and are easy to use as there is no need to tie knots [2728]. However, in some cases, the exposed barbed suture material caused entanglement and/or erosion of bowel or mesentery, resulting in bowel complications, including bowel obstruction, strangulation, or volvulus, and thus requiring surgical intervention [1213]. To eliminate these complications, previous case reports recommended cutting the barbed suture devices flushed with the myometrium or using the conventional suture material for repair of the seromuscular layer of the myometrium [13]. Besides, barbed sutures cannot be reversed, and fine-tuning of tension can be difficult. Moreover, this type of suture device is unavailable in some countries, and the cost can be a problem. However, in Choi's LM, we repaired the uterine defect with Vicryl sutures, which are commonly used in laparotomy or laparoscopic surgery. Unlike the barbed suture devices, tension can be modified repeatedly with Choi's LM if needed, and once the suture is passed, additional Hem-o-lok clips could be applied on the suture site repeatedly to maintain tension, if required. This procedure is very simple compared with the conventional interrupted suturing method and is effective for hemostasis.
There were several limitations in our study. First, the number of cases was small and many patients required an additional port. However, surgeons who perform SP-LM should keep in mind that the purpose of the operation is not to use a single-port approach, but to successfully perform a myomectomy. Therefore, surgeons should not hesitate to convert from a single-port system to a 2-port system if necessary to achieve complete myomectomy. Moreover, we expect that the conversion rate to a 2-port system will decrease with technical improvements and increase in surgeon's experience. Second, a greater limitation is the lack of control group. Hence, futures studies should provide a comparison between the new suture technique and the conventional suture method. Lastly, although the nonabsorbable Hem-o-lok polymer ligation clip has been widely used in laparoscopic surgery [29303132333435], the Hem-o-lok clips present on the uterine surface may lead to foreign body reaction since the Hem-o-lok clips have adhesive potential.
In conclusion, recent trends in the surgical treatment of uterine leiomyoma include minimally invasive options, such as single-port surgery. However, repairing the uterine defect using a single-port system is one of the most challenging and time-consuming steps. This study showed that SP-LM using a modified suture technique with a Hem-o-lok clip (Choi's LM) is a feasible and safe alternative in select patients. However, a large prospective study is required to conclusions.
Go to :
 XML Download
XML Download