

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Preterm delivery takes place before the 37th week of pregnancy [1]. This type of delivery is one of the most important causes of mortality and morbidity in infants around the world [23]. Even, in the most developed countries, the preterm delivery rate has increased. For example, in the United States, it has risen from 9.5% in 1981 to 12.7% in 2005 [4]. In Europe and other developed countries, the estimated preterm delivery rate is about 5–9% [56]. Preterm delivery is also responsible for 17–34% of deaths in infants in the first year of life in the United States [7]. However, almost 90% of the preterm deliveries occur in the developing countries of which 85% take place in Asia and Africa [8]. In Iran, as a developing country, the preterm delivery rate was estimated between 5.6% and 13.4% based on the geographical regions under study [9]. Preterm birth causes 75% of perinatal deaths and over 50% of the preterm babies have long-term morbidities. Many preterm infants are at increased risk of death, different diseases, and disabilities, such as developmental disorders of the nervous and respiratory system, defect in sense, learning disability, digestive complications, and many other health problems [1011].
Given the worrying trend of preterm delivery throughout the world and its related outcomes, it seems that studying the causes and risks of these factors is very important [812]. Factors causing preterm birth have not been fully identified yet, however, various studies have considered different factors in the etiology of this outcome [13]. Some studies in this regard have mentioned the following factors as possible causes of preterm birth: genetic factors, rupture of membranes, hypertension, diabetes, multiparity, multiple births, techniques of infertility treatment, elective Caesarean section during previous pregnancies, smoking and alcohol consumption during pregnancy, mental disorders, and environmental exposures [8]. However, identifying the precise cause of preterm delivery still requires further studies, especially in developing countries where few studies have been conducted in this area [14].
Hence, given the importance of preterm delivery and its consequences as a major global health problem and the few studies conducted so far in Iran, the present study was designed to determine the maternal risk factors of preterm delivery in Iran. Identifying the risk factors can be an effective step in preventing and controlling the consequences and complications of preterm delivery.
Materials and methods
1. Study design and subjects
This study was a population-based case-control study. Cases included all pregnant mothers referred to the maternity wards of the Selseleh County hospitals (Lorestan province, Iran) who had preterm delivery between March 21, 2007 and March 21, 2012. The preterm delivery was defined as delivery before 37 weeks of gestation. Preterm delivery cases were identified by daily monitoring of all the new deliveries in all the maternity wards of the County hospitals. On the other hands, the preterm delivery cases were considered as incident cases. Then, for each case, two controls were selected. The controls were a selected by random sampling from all the pregnant mothers referred to the same maternity wards of the County hospitals who had term delivery (≥37 weeks of gestation) during the same period (±2 weeks). In this study, mothers with premature infants due to congenital or chromosomal anomalies were excluded.
2. Data collection
The data collection tool was a standard questionnaire. However, some information was obtained through interviews with the pregnant mothers and some were gathered from the medical records. The questionnaire included information, such as demographic characteristics of the mother (age, occupation, body mass index, education, etc.), past obstetric history (gestational age at delivery, history of caesarian delivery, unwanted pregnancy, gravidity, multiparity, childbirth, etc.), complications of pregnancy and delivery (such as history of gestational diabetes, hypertension, abortion, eclampsia, placenta previa, uterine prolapse, stillbirth and etc.). The data were collected by a trained research doctor.
3. Statistical analysis
For analysis, the relevant data were entered into Stata 14. Descriptive analyses, such as mean and standard deviation were used for the continuous variables; and number and relative frequency were used for the categorical variables. For determination of the most important risk factors of preterm delivery, univariate and multivariable logistic regression analyses were performed. Then, the crude and adjusted odds ratio (OR) with 95% confidence interval (CI) were calculated. A large number of risk factors were evaluated, and hence, inadequate data for the combination of the maternal risk factors and preterm delivery (2×2 contingency table) are expected. It is argued that when there are inadequate data for the combination of the risk factors and outcomes, the estimates, such as OR and its CI, could be biased [15]. As a result, the OR tends to be inflated and its CI tends to be inappropriately wide. Such bias is known as sparse data bias and it can exaggerate the results of the multivariable analysis [15]. Penalization via data augmentation and firth bias adjustment was performed to offset the impact of sparse data bias on the results. Firth bias adjustment is a common traditional technique for reducing sparse data bias in which ½ is added to each cell of a contingency table. In penalization by data augmentation method, a very weakly informative prior [log-F(2, 2)] was considered for the effect of the maternal risk factors (βi in logistic regression model or ORs) on the preterm delivery. It is argued that very weakly informative prior provides a plausible range for the relative estimates with 95% certainty and the OR of the effect of maternal risk factors on preterm delivery falls between 1/40 and 40 [16]. The area under the receiver operating characteristic (ROC) curve was used for assessing the discriminative ability of the multivariable logistic regression analysis. A P-value of <0.05 was considered as statistically significant.
Results
The maternal characteristics of the cases and controls, as well as the results of the univariate logistic regression analysis, are shown in Table 1. A total of 48 cases with preterm delivery and 100 controls were enrolled in the study. The mean (standard deviation) age of the cases was 32.25 (6.81) years and that of the controls was 29.33 (6.56) years (P=0.02). A majority of the cases and controls had a school or lower level of education (65% vs. 70%, respectively). A majority of the cases and controls had a gravida of ≤3, history of ≤2 childbirths, and no history of abortion.
Table 1
Association between preterm delivery and maternal characteristics using univariate logistic regression analysis
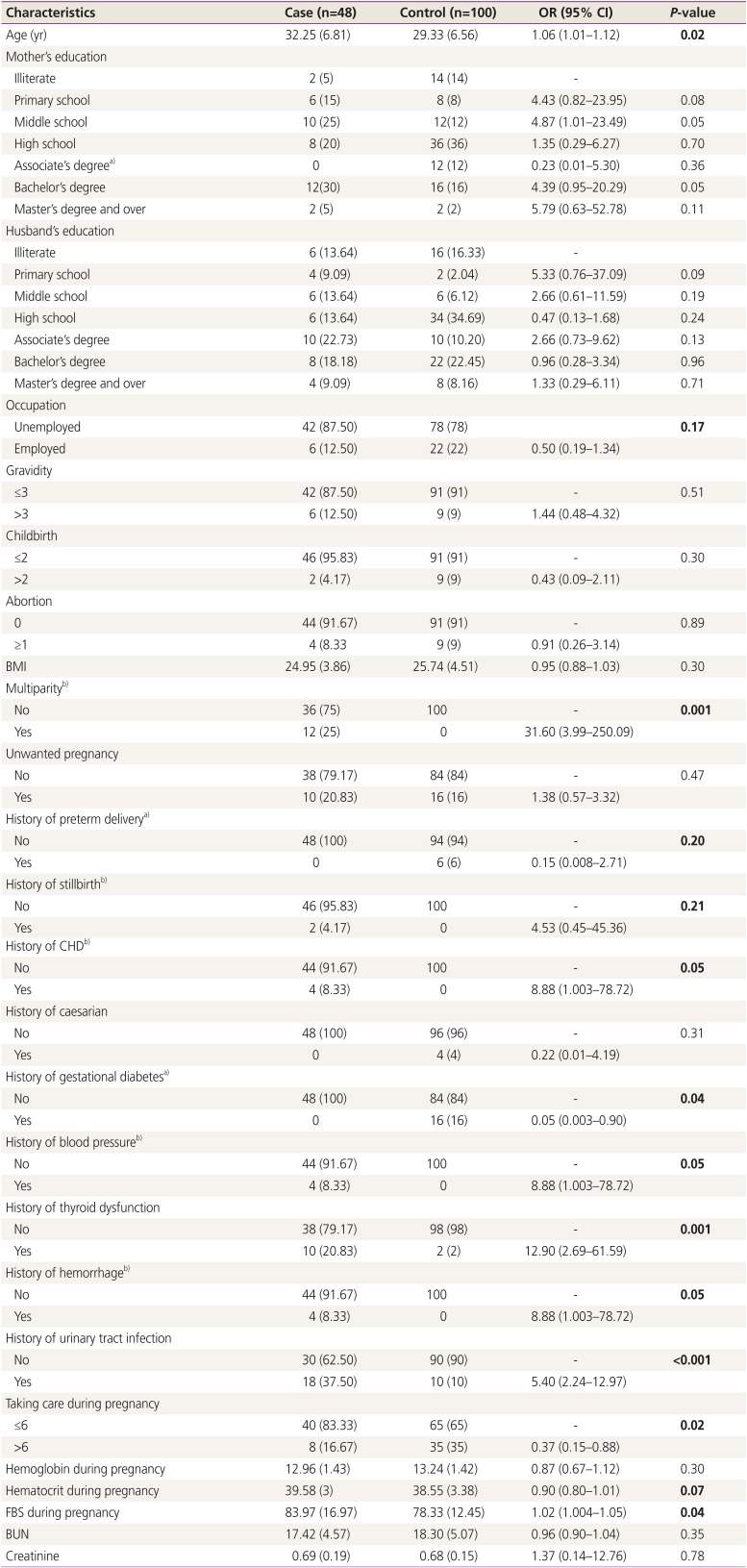
A significant difference was found between the cases and the controls regarding the multiparty, history of coronary heart disease (CHD), gestational diabetes, blood pressure, thyroid dysfunction, hemorrhage, urinary tract infection, taking care during pregnancy, and FBS level (all P≤0.05). The highest significant crude OR was found for multiparity (OR, 31.60; 95% CI, 3.99–250.09). The odds of preterm delivery was 5.40 times higher in those having a history of urinary tract infection than those without (95% CI, 2.24–12.97). Similarly, the odds of the outcome was 2.73 times lower in the women who received ≥6 care during pregnancy from rural or urban health centers than those who received <6 care during pregnancy (OR, 0.37; 95% CI, 0.15–0.88).
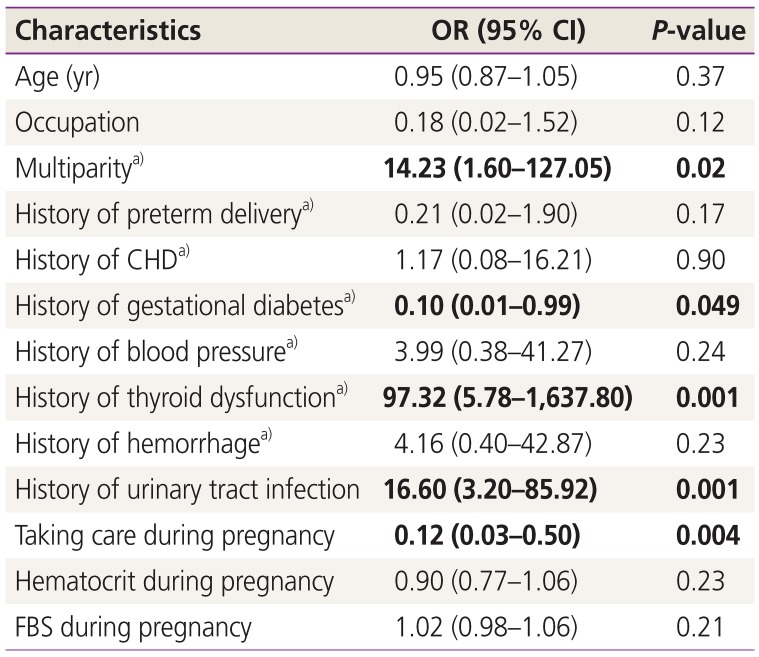
The results of the multivariable logistic regression analysis are presented in Table 2. After selecting the variables with a P-value of ≤0.20 in the univariate analysis for the multivariable analysis, only multiparity, history of gestational diabetes, thyroid dysfunction, urinary tract infection, and taking care during pregnancy were statistically significant (P≤0.05). The highest adjusted OR was determined for a history of thyroid dysfunction (OR, 97.32; 95% CI, 5.78–1,637.80).
Table 2
Association between preterm delivery and maternal risk factor using multivariable logistic regression analysis
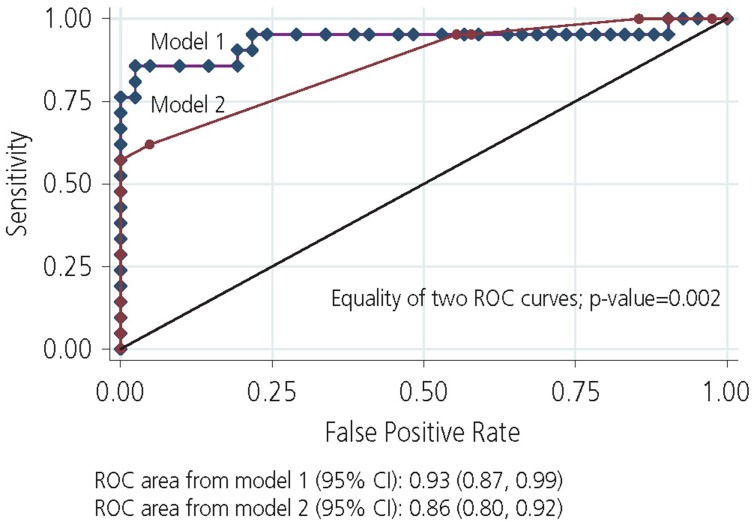
The ROC curves for model 1 with all 13 maternal characteristics included in the multivariable logistic regression analysis and for model 2 with only the significant maternal characteristics included in the multivariable logistic regression analysis are shown in Fig. 1. In analyses that compared the ability of the models to discriminate preterm labor, the ROC for model 1 was significantly greater than that of model 2 (0.93 vs. 0.86, P=0.002).
Discussion
The present study aimed to determine the maternal risk factors for preterm delivery in Iran, which was achieved by a population-based case-control study. The results of the multivariable logistic regression analysis showed that variables, such as multiparity, history of gestational diabetes, thyroid dysfunction, urinary tract infection, and taking care during pregnancy had significant statistical associations with preterm delivery (P<0.05). Besides, the area under the ROC curve for the significant maternal variables in the multivariable logistic regression analysis was 0.86 (95% CI, 0.80–0.92)
In the present study, mothers who received prenatal care for ≥6 times during pregnancy had a lower risk of preterm delivery as compared to those who received care for <6 times (OR, 0.12; 95% CI, 0.03–0.50). This finding has been supported by various other studies in this regard [1314171819]. For example, the study by Jiang et al. [13] showed that lack of prenatal care is related to an increased risk of preterm birth, so that the mothers without prenatal care during pregnancy had 5.19 times increased risk of preterm birth (OR, 5.19; 95% CI, 3.77, −7.14); and mothers with irregular prenatal care had 2.87 times of increased risk of preterm birth (OR, 2.87; 95% CI, 2.16–3.80). Another study performed in Iran showed that mothers of premature infants received less perinatal care; while with more care, the risk of premature delivery was reduced [18]. Perhaps more attention to risk symptoms is paid during prenatal care along with appropriate health and treatment advice by the health care personnel. Hence, improving prenatal care and increasing the number of care can be effective in reducing the risk of premature birth. However, this interpretation about the number of prenatal care in the present study should be done with caution, because the low number of perinatal care in the mothers with premature infants might be due to premature birth and consequently shorter gestational age.
In agreement with other previous studies, the results of this study showed that there was a significant statistical association between multiparity and preterm delivery after adjusting the confounding variables (OR, 14.23; 95% CI, 1.60–127.05) [1320212223]. The study by Shoja et al. [23] indicated that the odds of preterm delivery in mothers with multiparity pregnancy was more than those without multiparity pregnancy (OR, 3.09; 95% CI, 1.01–9.6). This problem may be because multiparity limits the uterine space for the fetus and also causes secretion of hormones inducing delivery, and therefore, preterm labor was more in this group.
In this study, we found a significant negative association between preterm delivery and maternal medical disorders, such as gestational diabetes (OR, 0.10; 95% CI, 0.01–1.01) after adjustment of the confounding variables. This finding was inconsistent with studies conducted in this field [3141824252627]. The study by Namakin et al. [18] in Iran showed that mothers with a history of gestational diabetes and hypertension had a higher risk of preterm delivery (OR, 2.99; 95% CI, 1.6–5.5). Zhang et al. [14] in China reported that women with a history of gestational diabetes have 3.44-fold increased risk of preterm birth (OR, 3.44; 95% CI, 1.69–6.99). On the other hand, several studies have shown that there no association between preterm delivery and gestational diabetes [132829]. For example, a case-control study in China showed no relationship between gestational diabetes and preterm delivery [13]. Perhaps one of the reasons for the negative relationship in this study was the low sample size involved. However, it can be said that gestational diabetes can affect the growth and development of the fetus during pregnancy. Particularly, during the second and third trimesters of pregnancy, maternal diabetes can lead to a high level of nutrition and fetal growth. Subsequently, a large fetus with increased bodyweight may also increase the risk of preterm delivery. Therefore, regular monitoring of blood glucose during pregnancy should be given special attention.
In the present study, there was a significant statistical association between thyroid dysfunction (OR, 97.32; 95% CI, 5.78–1,637.80) and preterm delivery in the multivariable logistic regression analysis, and this is in agreement with other previous studies [33031323334]. A review by Nazarpour et al. [32] showed that thyroid dysfunction has adverse effects on pregnancy outcomes especially on the preterm delivery. Another review by Stagnaro-Green [30] also suggested that hypothyroidism and autoimmune thyroid disease are associated with preterm delivery in women. Given the high prevalence of thyroid disorders in women on one hand and the hormonal changes and multiple metabolic needs occurring during pregnancy affecting the mother's thyroid function on the other, it is recommended that all pregnant women check their thyroid gland function before trying for pregnancy to prevent adverse consequences of thyroid disorders.
Finally, in agreement with other previous studies [2335363738], the results of our study indicated that there is a significant statistical association between the history of urinary tract infection and preterm delivery after adjusting the confounding variables (OR, 16.60; 95% CI, 3.20–85.92). A study by Shoja et al. [23] demonstrated that there was a significant statistical relationship between pregnancy infection and preterm delivery (OR, 2.78; 95% CI, 1.07–7.20). Another study in this field showed that mothers with a history of urinary tract infection had a 1.59-fold increased risk of preterm delivery (OR, 1.59; 95% CI, 1.14–2.21) [38]. Different studies indicate that microorganisms in the membranes are associated with increased prostaglandin production, which is one of the important factors associated with the prevalence of preterm labor. Prostaglandin is produced by the invasion of microorganisms, coagulase protease, and elastase and the endotoxin directly induces preterm delivery. One of the most common microorganisms is β-hemolytic streptococcus, which may be present in the natural vaginal flora in 50% of women and causes 20% of preterm labor [3839]. Therefore, treatment of infections in pregnancy is one of the factors that reduce the prevalence of preterm labor and its recurrence.
One of the limitations of this study that can be noted is the retrospective nature and low sample size. Therefore, it is recommended that cohort studies be carried out in larger geographic units and with a larger sample size to determine the precise causes of preterm delivery. Additionally, some information was extracted from the mother's medical records which may not be accurately recorded and associated with information bias. Also, the last limitation of this study, which should be mentioned, is selection bias. For some of the variables, such as multiparity, unwanted pregnancy, stillbirth, CHD, etc., there were no women in the control group, therefore, these risk factors might be have been affected by selection bias rather than by the actual risks.
In summary, the results of this study suggest that multiparity, history of gestational diabetes, thyroid dysfunction, urinary tract infection, and taking care during pregnancy have a significant statistical association with preterm delivery. The area under the ROC curve for these variables was 0.86. Therefore, performing perinatal care and identifying pregnant mothers with the above risk factors can reduce the preterm delivery rate, and subsequently reduce the consequences of preterm delivery in the infants and the mothers.
 XML Download
XML Download