

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Giant cell hepatitis (GCH) with autoimmune hemolytic anemia (AHA) is a rare disease of infancy, characterized by the presence of both Coombs-positive hemolytic anemia and progressive liver disease with giant cell transformation of hepatocytes [1]. Even though its exact pathophysiology is unclear, it may involve B-cell-mediated autoimmunity [2]. Steroids and azathioprine, which are known to be effective in treating ‘classical’ autoimmune hepatitis, have failed to show long-term efficacy in the treatment of GCH-AHA. However, there are several reports of successful treatment with the anti-CD20 monoclonal antibody, rituximab. We report a case of GCH-AHA associated with jaundice, pallor, and red urine, where remission was achieved following treatment with rituximab.
CASE REPORT
A seven-month-old male infant was referred to the Seoul National University Children's Hospital due to severe anemia. Over a period of one month, he had intermittent red urine. However, this worsened four days prior to the initial visit. He also had jaundice, which was noticed one week prior to visiting the hospital. He had no family history of autoimmune disease or liver disease, except for a gallstone in his father which was treated by cholecystectomy. However, it was unknown whether the patient's father had a pigmented gallstone. Physical examination revealed jaundice, pallor, and splenomegaly.
The results after laboratory examination are as follows: white cell blood count, 11,700/mm3; hemoglobin, 3.5 g/dL; platelet count, 295,000/mm3; and reticulocytes, 32.7%. Severe normocytic hypochromic anemia was observed and several spherocytes and teardrop cells were observed in the peripheral blood smear. Both direct and indirect Coombs test results were positive, and Coombs anti-IgG and anti-C3d were positive. Low plasma haptoglobin and increased plasma hemoglobin were detected. The liver function test revealed the following: aspartate aminotransferase (AST), 180 IU/L; alanine aminotransferase (ALT), 169 IU/L; serum total bilirubin, 4.8 mg/dL; and serum conjugated bilirubin, 2.03 mg/dL. The prothrombin time internatonal normalized ratio was 0.95 and plasma ammonia level was 56 μmoL/L.
To evaluate the etiology of the cholestatic hepatitis, autoimmune, infectious, and metabolic causes were investigated. Serological test results for hepatitis A, B, and C; Epstein-Barr virus; herpes simplex virus; rubella virus; and toxoplasma were all negative. The cytomegalovirus (CMV) IgM test result was positive and the alpha-fetoprotein level was 30.3 ng/mL. The immunoglobulin G, A, and M levels were 622 mg/dL, 28 mg/dL, and 211 mg/dL, respectively. Test results for the anti-neutrophil cytoplasmic antibody, anti-liver-kidney-microsomal antibody 1, and anti-smooth muscle antibody were negative. The test result for the anti-nuclear antibody was weakly positive (1:40). Plasma amino acid analysis showed increased levels of methionine, lysine, and threonine, which was interpreted as a nonspecific result of liver injury. Urine organic acid analysis was nonspecific. Liver ultrasonography revealed no significant abnormalities.
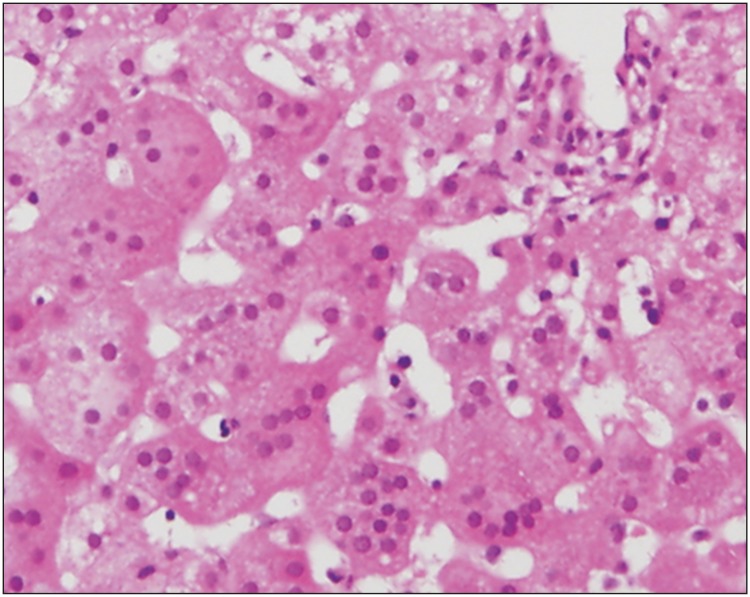
The laboratory findings suggested warm-type autoimmune hemolytic anemia with infantile cholestasis of unknown cause. The patient was admitted and was administered intravenous (IV) methylprednisolone. On day 4, the IV methylprednisolone was switched to an equivalent dose of oral prednisolone (2 mg/kg daily). Red blood cell transfusion was performed four times. Following treatment with ursodeoxycholic acid (UDCA) and steroids, the liver function test results improved and the hemolytic anemia was stabilized. Thus, the steroid dose was tapered to 1.5 mg/kg daily. One month later, the patient developed jaundice and was producing pinkish urine again. The liver function test results were as follows: AST, 309 IU/L; ALT, 903 IU/L; total bilirubin, 4.4 mg/dL; and conjugated bilirubin, 2.33 mg/dL. Abdominal ultrasonography revealed slightly heterogeneous hepatic parenchymal echogenicity with mild splenomegaly. Liver biopsy revealed multinucleated hepatocytes, hepatocyte rosette formation, moderate lobular inflammation with neutrophilic infiltration, and frequent spotty necrosis. Portal inflammation was minimal with no bile duct abnormalities and fibrosis (Fig. 1). There was no evidence of CMV infection.
The association of hepatitis and warm-type autoimmune hemolytic anemia in a young infant, the absence of autoantibodies, the infectious and metabolic causes, and the histological evidence of giant cell transformation of hepatocytes led to the diagnosis of GCH-AHA. During the follow-up period, the patient had progressive anemia and worsening hepatitis. The peak values were measured on day 7 of admission and were as follows: AST, 1,781 IU/L; ALT, 4,136 IU/L; total bilirubin, 15.6 mg/dL; and conjugated bilirubin, 9.52 mg/dL. On day 4, he received a high dose (2 g/kg daily) of intravenous immunoglobulin (IVIG). On day 6, the prednisolone dose was increased to 2 mg/kg daily, and he received rituximab infusion at a dose of 375 mg/m2. The serum AST, ALT, and bilirubin levels began to decline on day 8. He received a total of four weekly doses of rituximab. One month after the diagnosis, the liver function was normal. Six weeks after the diagnosis, hemolytic anemia, however, relapsed with a hemoglobin level of 4.9 g/dL. He received a high dose (2 g/kg daily) of IVIG and one additional dose of rituximab. His anemia improved after two weeks of treatment. Three months after diagnosis, he was admitted to the intensive care unit for respiratory failure. Combined pneumocystis and CMV pneumonia were diagnosed and he received IV trimethoprim-sulfamethoxazole, pentamidine, and ganciclovir. Nine months after the diagnosis, the relapse of hemolytic anemia and hepatitis was observed. However, it was controlled by administering one additional dose of rituximab. The patient has been in clinical remission for 10 months after the last relapse and continues to receive oral prednisolone (0.5 mg/kg daily) along with UDCA (Fig. 2).
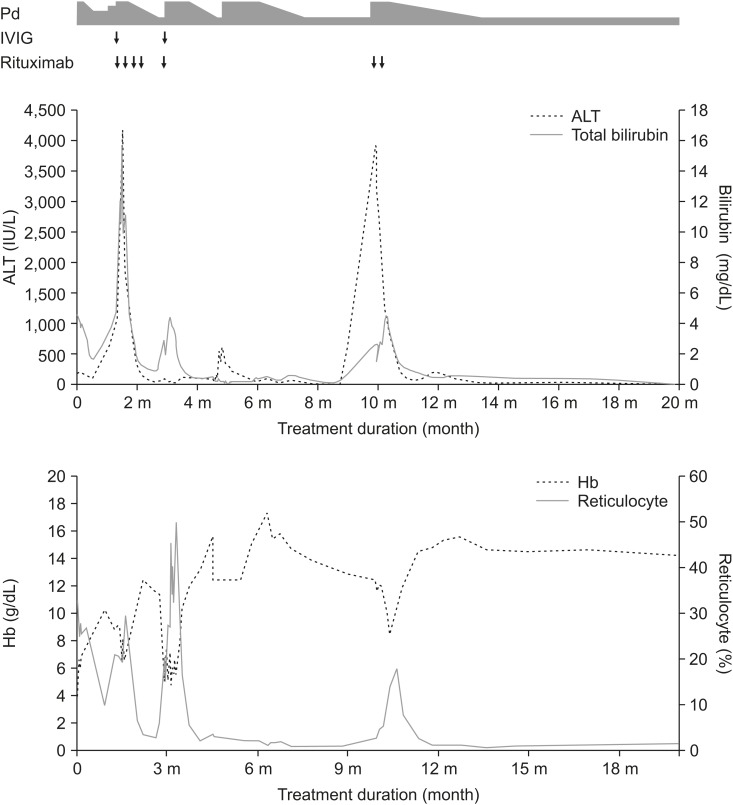
Fig. 2
Treatment course and response to therapy. ALT, total bilirubin, Hb, and reticulocyte percentage are shown over time. Dose of steroid is represented by the thickness of gray bar; the highest point being 2 mg/kg/day. IVIG and rituximab administration is marked by arrows.
ALT: alanine aminotransferase, Hb: hemoglobin, IVIG: intravenous immunoglobulin, Pd: prednisolone.
DISCUSSION
GCH-AHA is a descriptive term for a condition in which both Coombs-positive anemia and severe hepatitis characterized by giant cell transformation of the hepatocytes are present [13]. It is a very rare disease and less than 100 cases have been reported in the English literature since its first recognition. Infants and young children are predominantly affected. The median age at onset is eight months [4]. Majority of the cases have been described in Caucasian populations. However, very few cases from East Asia have also been reported [5].
Most patients initially present with signs of hemolytic anemia, such as pallor, jaundice, and hepatosplenomegaly [3]. Hepatitis usually occurs within one week to 15 months (usually one to two months) following the diagnosis of AHA [6]. Although the onset of hepatitis is usually insidious, it can rapidly progress to liver failure [17]. Prognosis is often poor, and the mortality rate can reach as high as 30% [3]. The causes of death range from disease progression to liver failure and severe infection due to prolonged immunosuppression [13].
The pathogenesis of the disease is unclear; however, several studies have suggested the involvement of an autoimmune mechanism based on the clinical response to immunosuppressive therapies [18]. The absence of the conventional autoantibodies associated with autoimmune hepatitis and the different histopathological patterns suggest that the mechanism that underlies the pathogenesis of GCH-AHA differs from that of ‘classical’ autoimmune hepatitis [1]. This finding is consistent with the frequently reported resistance to steroids and azathioprine in GCH-AHA patients [3].
Whittington et al. [2] proposed B-cell-mediated autoimmunity as a major mechanism involved in the development of this disease. In GCH-AHA patients, giant cell transformation of hepatocytes, marked alterations in the lobular structure, and minimal portal inflammation are observed. A similar pattern is also observed in gestational alloimmune liver disease (GALD), which is caused by IgG-driven complement-mediated hepatocyte injury. C5b-9 staining revealed that the pattern of C5b-9 deposition in the hepatocytes of GCH-AHA patients is similar to that observed during GALD, suggesting that a complement-mediated injury is also involved in GCH-AHA. Based on their observations, the authors concluded that B-cell-mediated autoimmunity may play a role in GCH-AHA. Their finding is further supported by several studies that reported successful treatment with rituximab, which specifically targets B cells [91011].
For treatment, several immunosuppressants have been tested since the first description of the disease (Table 1) [12345678910111213141516171819202122232425]. There are several reports of clinical response following treatment with high doses of corticosteroids. However, after tapering the doses, a high rate of recurrence was reported [1312]. Even though successful maintenance with azathioprine has been reported by several authors, there are also frequent reports of refractory diseases [3812]. Trials involving IVIG, cyclosporine, cyclophosphamide, vincristine, plasmapheresis, and alemtuzumab have been reported, with anecdotal success [713141516]. Liver transplantation was performed in a small number of patients. However, virtually all cases were complicated by early relapse or graft rejection, and therefore, liver transplantation is no longer recommended presently [1718].
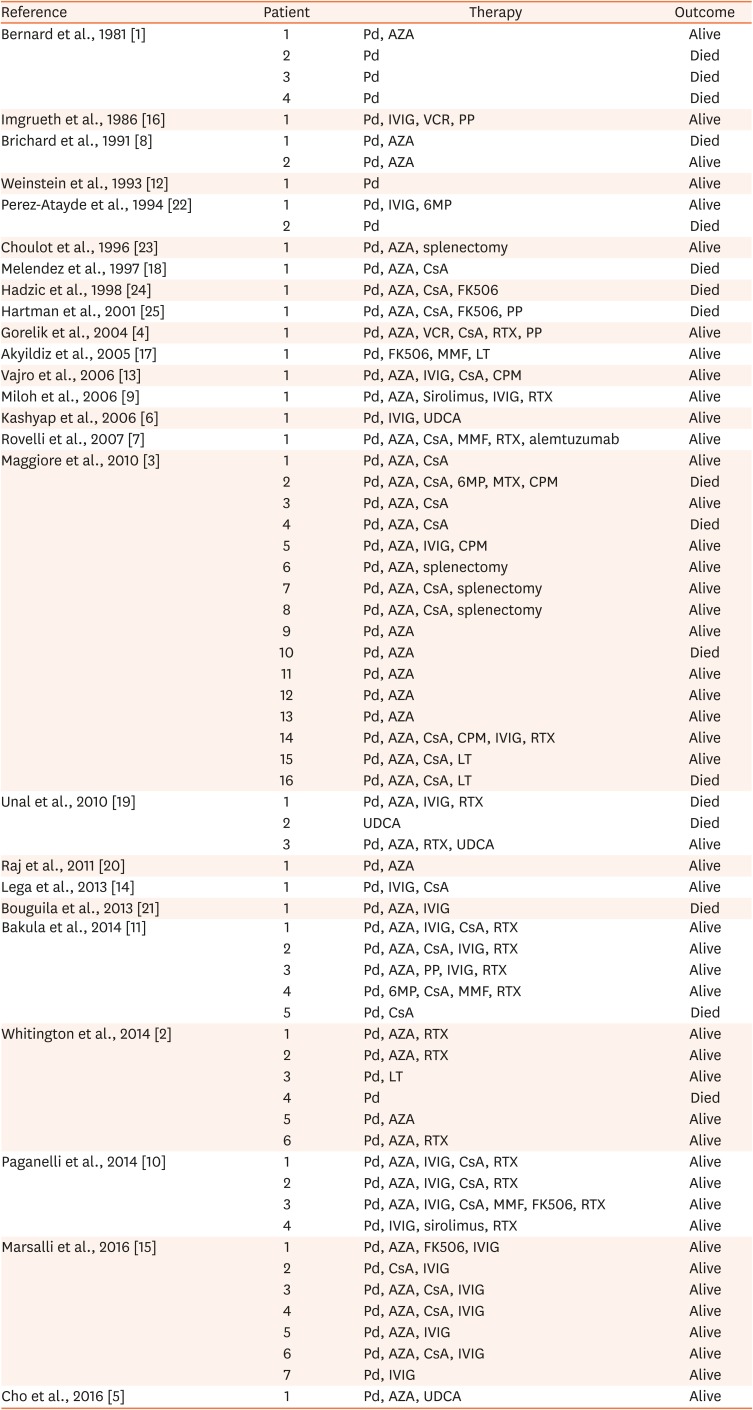
Table 1
Therapeutic interventions in previously reported cases of GCH with AHA
| Reference | Patient | Therapy | Outcome |
|---|---|---|---|
| Bernard et al., 1981 [1] | 1 | Pd, AZA | Alive |
| 2 | Pd | Died | |
| 3 | Pd | Died | |
| 4 | Pd | Died | |
| Imgrueth et al., 1986 [16] | 1 | Pd, IVIG, VCR, PP | Alive |
| Brichard et al., 1991 [8] | 1 | Pd, AZA | Died |
| 2 | Pd, AZA | Alive | |
| Weinstein et al., 1993 [12] | 1 | Pd | Alive |
| Perez-Atayde et al., 1994 [22] | 1 | Pd, IVIG, 6MP | Alive |
| 2 | Pd | Died | |
| Choulot et al., 1996 [23] | 1 | Pd, AZA, splenectomy | Alive |
| Melendez et al., 1997 [18] | 1 | Pd, AZA, CsA | Died |
| Hadzic et al., 1998 [24] | 1 | Pd, AZA, CsA, FK506 | Died |
| Hartman et al., 2001 [25] | 1 | Pd, AZA, CsA, FK506, PP | Died |
| Gorelik et al., 2004 [4] | 1 | Pd, AZA, VCR, CsA, RTX, PP | Alive |
| Akyildiz et al., 2005 [17] | 1 | Pd, FK506, MMF, LT | Alive |
| Vajro et al., 2006 [13] | 1 | Pd, AZA, IVIG, CsA, CPM | Alive |
| Miloh et al., 2006 [9] | 1 | Pd, AZA, Sirolimus, IVIG, RTX | Alive |
| Kashyap et al., 2006 [6] | 1 | Pd, IVIG, UDCA | Alive |
| Rovelli et al., 2007 [7] | 1 | Pd, AZA, CsA, MMF, RTX, alemtuzumab | Alive |
| Maggiore et al., 2010 [3] | 1 | Pd, AZA, CsA | Alive |
| 2 | Pd, AZA, CsA, 6MP, MTX, CPM | Died | |
| 3 | Pd, AZA, CsA | Alive | |
| 4 | Pd, AZA, CsA | Died | |
| 5 | Pd, AZA, IVIG, CPM | Alive | |
| 6 | Pd, AZA, splenectomy | Alive | |
| 7 | Pd, AZA, CsA, splenectomy | Alive | |
| 8 | Pd, AZA, CsA, splenectomy | Alive | |
| 9 | Pd, AZA | Alive | |
| 10 | Pd, AZA | Died | |
| 11 | Pd, AZA | Alive | |
| 12 | Pd, AZA | Alive | |
| 13 | Pd, AZA | Alive | |
| 14 | Pd, AZA, CsA, CPM, IVIG, RTX | Alive | |
| 15 | Pd, AZA, CsA, LT | Alive | |
| 16 | Pd, AZA, CsA, LT | Died | |
| Unal et al., 2010 [19] | 1 | Pd, AZA, IVIG, RTX | Died |
| 2 | UDCA | Died | |
| 3 | Pd, AZA, RTX, UDCA | Alive | |
| Raj et al., 2011 [20] | 1 | Pd, AZA | Alive |
| Lega et al., 2013 [14] | 1 | Pd, IVIG, CsA | Alive |
| Bouguila et al., 2013 [21] | 1 | Pd, AZA, IVIG | Died |
| Bakula et al., 2014 [11] | 1 | Pd, AZA, IVIG, CsA, RTX | Alive |
| 2 | Pd, AZA, CsA, IVIG, RTX | Alive | |
| 3 | Pd, AZA, PP, IVIG, RTX | Alive | |
| 4 | Pd, 6MP, CsA, MMF, RTX | Alive | |
| 5 | Pd, CsA | Died | |
| Whitington et al., 2014 [2] | 1 | Pd, AZA, RTX | Alive |
| 2 | Pd, AZA, RTX | Alive | |
| 3 | Pd, LT | Alive | |
| 4 | Pd | Died | |
| 5 | Pd, AZA | Alive | |
| 6 | Pd, AZA, RTX | Alive | |
| Paganelli et al., 2014 [10] | 1 | Pd, AZA, IVIG, CsA, RTX | Alive |
| 2 | Pd, AZA, IVIG, CsA, RTX | Alive | |
| 3 | Pd, AZA, IVIG, CsA, MMF, FK506, RTX | Alive | |
| 4 | Pd, IVIG, sirolimus, RTX | Alive | |
| Marsalli et al., 2016 [15] | 1 | Pd, AZA, FK506, IVIG | Alive |
| 2 | Pd, CsA, IVIG | Alive | |
| 3 | Pd, AZA, CsA, IVIG | Alive | |
| 4 | Pd, AZA, CsA, IVIG | Alive | |
| 5 | Pd, AZA, IVIG | Alive | |
| 6 | Pd, AZA, CsA, IVIG | Alive | |
| 7 | Pd, IVIG | Alive | |
| Cho et al., 2016 [5] | 1 | Pd, AZA, UDCA | Alive |
GCH: Giant cell hepatitis, AHA: autoimmune hemolytic anemia, Pd: prednisolone, AZA: azathioprine, IVIG: intravenous immune globulin, VCR: vincristine, PP: plasmapheresis, 6MP: 6-mercaptopurine, CsA: cyclosporine A, FK506, tacrolimus, RTX: rituximab, MMF: mycophenolate mofetil, LT: liver transplantation, CPM: cyclophosphamide, UDCA: ursodeoxycholic acid.
Gorelik et al. [4] reported the first successful treatment of steroid-resistant anemia in GCH-AHA with an anti-CD20 monoclonal antibody, rituximab. Their rationale was based on the observation that rituximab is safe and effective in treating refractory autoimmune hemolytic anemia. Miloh et al. [9] reported the first successful control of refractory hepatitis in GCH-AHA with rituximab. Since then, an increasing number of patients have been successfully treated with rituximab [231011]. Although relapse after rituximab therapy is frequently reported, all but one patient achieved clinical remission after additional doses of rituximab were administered. Only one case involving rituximab-refractory GCH-AHA has been reported so far, and in that case, the GCH-AHA was controlled using an anti-CD52 monoclonal antibody, alemtuzumab [7]. However, in the aforementioned study, three doses of rituximab were administered, whereas in most of the studies, four doses were administered. This difference might have prevented the achievement of clinical remission in their case. Therefore, it is recommended to administer at least four doses of rituximab for initial treatment. Additional doses should be considered if there is incomplete remission or relapse [11].
In our patient, autoimmune hemolytic anemia was the first manifestation of the disease at the age of seven months. IV methylprednisolone and a subsequent high dose of prednisone initially induced remission of anemia; however, a relapse of anemia and aggravation of hepatitis was observed after the dose was tapered. The condition was not controlled until initiation of treatment with rituximab, which led to a marked clinical response. Although there were two episodes of relapse after initial clinical remission, they were effectively controlled by administering additional doses of rituximab. We believe that this is the first reported case involving the successful treatment of GCH-AHA with rituximab without the use azathioprine or maintenance immunosuppressants other than steroids (Table 1) [12345678910111213141516171819202122232425]. The clinical course was complicated due to the coexistence of pneumocystis and CMV pneumonia. Since impairment in T cell immunity is implied in these opportunistic infections, the most likely culprit seems to be the long-term use of high doses of steroids rather than rituximab, which selectively kills B cells.
Steroids and azathioprine are still considered as the first line treatments for GCH-AHA; however, the frequent relapses and serious complications may even result in death [3]. In contrast, there is increasing reports of rituximab leading to the achievement of clinical remission in GCH-AHA. No serious adverse effects have been reported to date, although potential adverse effects include infusion reaction, allergic reaction, increased susceptibility to infection, and hypogammaglobulinemia. Additionally, rituximab has a steroid-sparing effect, which could potentially prevent serious complications as a result of the long-term administration of high doses of steroids [10]. Considering the involvement of B-cell-mediated autoimmunity in the pathogenesis of the disease, early administration of rituximab is recommended. Further studies on the efficacy and safety of rituximab as a first-line treatment are required. Additionally, guidelines for salvage therapy after relapse following the administration of four doses of the drug are also needed.
 XML Download
XML Download