

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cow's milk allergy (CMA) is a common diagnosis in infants and children. It manifests in a variety of ways, including skin manifestations, respiratory symptoms, and gastrointestinal tract symptoms. However, the symptoms of CMA are nonspecific. Moreover, other diseases, including functional gastrointestinal disorders such as infantile colic and gastroesophageal reflux disease, may have overlapping symptoms. Additionally, at times, many healthcare professionals and parents alike confuse, CMA with lactose malabsorption. As a consequence, CMA is clearly overdiagnosed in many cases, but it is also underdiagnosed in many others [1].
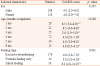
Recently, the Cow's Milk-related Symptom Score (CoMiSS™) was developed as an awareness tool for evaluating cow's milk-related symptoms [2]. The CoMiSS™ considers crying, regurgitation, stools, skin and respiratory symptoms (Table 1). Its score ranges from 0 to 33. Each symptom has a maximum score of 6, except respiratory symptoms where the maximum score is 3. An arbitrary cut-off CoMiSS™ value of ≥12 was proposed as being likely cow's milk-related and suggestive of CMA [3].
Table 1
The Cow's Milk-related Symptom Score

*Crying was only considered if the child was crying for 1 week or more, assessed by the parents, without any other obvious causes.
Although many infants with Cow's Milk-related Symptoms have no impaired growth or weight gain, faltering of these parameters suggests organic disease, of which Cow's milk allergy is a possible cause.
![]()
As CoMiSS™ values in presumed healthy infants remain limited, the collection of age-related CoMiSS™ data is needed. In 2017, a multicenter, cross-sectional study was conducted in four European countries with the aim of determining an age-related CoMiSS™ in presumed healthy infants [4]. The availability of such data is important to establishing a cut-off value for this tool to identify infants requiring further evaluation. The present study aimed to further determine the age-related CoMiSS™ values in presumed healthy infants in Poland.
MATERIALS AND METHODS
The method used in this study was similar to that used in the 2018 study by Vandenplas et al. [4]. In brief, this was a cross-sectional study involving a convenience series of participants attending well-child clinics in two locations in Poland (Warsaw, Trzebnica). The CoMiSS™ scores were determined in presumed healthy infants ≤6 months of age undergoing regular checkups involving routine vaccinations and growth and development monitoring. As cow's milk-related symptoms are also observed, in (a lower percentage) of breastfed infants, both formula- and breast-fed infants were eligible for inclusion. The exclusion criteria were as follows: any known history of acute or chronic diseases, preterm delivery (delivery <37 weeks of gestation), treatment with therapeutic formula (e.g., extensively hydrolyzed formula), and the administration of any food supplements (except vitamins) or medications. The baseline demographic characteristics (sex, age, gestational age at birth, type of feeding) and information about any history of acute or chronic diseases were collected to assess each infant's eligibility. The CoMiSS™ questionnaire was subsequently explained to the parents by the members of the research team, and the CoMiSS™ was determined. The study obtained ethical clearance from the ethics committee of the Medical University of Warsaw. Informed consent was obtained from each patient's parent or legal guardian.
Statistical analysis
The analysis was performed using the statistical software R (version 3.5.1; http://cran.r-project.org). Data were assessed for normality using the Kolmogorov-Smirnov test as well as by visual assessment of histograms. Nominal variables are presented as n (%), while continuous variables are presented as the median (Q1–Q3) due to the lack of a normal distribution and/or use of an ordinal measurement scale. The CoMiSS™ total score was compared between groups based on sex, age, and feeding type using the Mann-Whitney U-test or Kruskal-Wallis test, as appropriate. The Mann-Whitney U-test or Kruskal-Wallis test was also used to compare scores for individual components of the CoMiSS™ between groups. The post-hoc Dunn test with Bonferroni correction was used for the analysis of subgroups based on age and feeding type. Two-sided p-values <0.05 were considered as significant.
RESULTS
Study population
The study was conducted between January and August 2018. The infants' baseline demographic and clinical characteristics are shown in Table 2. Overall, data for 226 presumed healthy infants (118 female and 108 male) were available. The median (Q1–Q3) age was 4 months (3.0–4.0), with no difference between female and male. The majority of infants (192/226, 85.0%) were breastfed (exclusively or partially).
Table 2
Baseline characteristics

![]()
Overall results of the CoMiSS™
Table 3 presents the descriptive statistics, while the distribution of CoMiSS™ total values is shown in Fig. 1. The median (Q1–Q3) overall CoMiSS™ value was 4 (2–7), and the mean (standard deviation) was 4.7 (3.5). The 95th percentile (pc) for the total CoMiSS™ was 11. Eleven of the 226 (4.9%) infants had a total CoMiSS™ ≥12 (i.e., the value currently considered as suggestive of CMA).
Table 3
Descriptive statistics of the Cow's Milk-related Symptom Score

![]()

Analysis of the total CoMiSS™ by sex, age, and type of feeding
Table 4 presents the analysis of the total CoMiSS™ by sex, age, and type of feeding. There were no differences in the total CoMiSS™ values based on sex (p=0.345). However, the total CoMiSS™ values differed between age groups (p<0.001). The highest scores were recorded at month 1 and month 2 [median (Q1–Q3) 6.5 (5.0–9.0) and 6.5 (4.0–8.8), respectively]. Total CoMiSS™ values also differed between groups with different types of feeding (exclusive breastfeeding vs. formula feeding vs. mixed feeding) (p<0.001). The highest score was recorded in infants in the mixed feeding group [median (Q1–Q3) 6.0 (4.8–10.0)]; however, this score was based on the data from 9 only 16 infants.
Table 4
Analysis of the total CoMiSS™ by selected characteristics (sex, age, and type of feeding)
CoMiSS™: Cow's Milk-related Symptom Score.
Data presented as median (Q1–Q3); comparison of groups with Mann-Whitney U-test or Kruskal-Wallis test.
a-fp-values from Dunn post-hoc test.
ap<0.001, bp=0.007, cp=0.048, dp=0.010, ep=0.007, fp=0.027, gp=0.001.
![]()
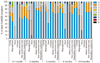
Distribution of CoMiSS™ individual component scores by sex, age, and type of feeding Table 5 and Figs. 2, 3, 4 present the distribution of scores for the CoMiSS™ individual components (crying, regurgitation, stools, skin symptoms, and respiratory symptoms) by sex, age, and type of feeding.
Table 5
Analysis of CoMiSS™ individual component scores by sex, age, and type of feeding

CoMiSS™: Cow's Milk-related Symptom Score.
Data presented as p-values; comparison of groups with Mann-Whitney U-test or Kruskal-Wallis test.
![]()

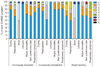 | Fig. 4Distribution of Cow's Milk-related Symptom Score (CoMiSS™) individual scores by the type of feeding.
|
Sex had no impact on scores for any of the CoMiSS™ individual components (Fig. 2). Age had an impact on crying (p=0.001) and stools (p<0.001) (Fig. 3). Type of feeding had an impact on stools (p<0.001) and total skin symptom score (urticaria, atopic dermatitis) (p=0.029) (Fig. 4). Neither sex, nor age, nor type of feeding had an impact on regurgitation or respiratory symptoms.
DISCUSSION
Principal findings
CoMiSS™ data from presumed healthy infants in various populations remain limited, and its availability is important for establishing a cutoff value for this tool to identify infants requiring further evaluation. This cross-sectional study adds to earlier age-related CoMiSS™ data by providing additional CoMiSS™ values in presumed healthy infants in Poland.
Comparison with other studies
This study was based on the same methodology used in the 2018 study by Vandenplas et al. [4]. In the latter study, the overall median CoMiSS™ value was similar between countries, but the 95th pc value was greater in the Polish infants (n=79; median 4, 95th pc 12) than in infants from Belgium (n=279; median 3, 95th pc 8), Italy (n=75; median 3, 95th pc 8), and Spain (n=130; median 4, 95th pc 9). Compared with earlier results, in the current larger Polish cohort, the 95th pc CoMiSS™ value (11) was similar as previously reported, suggesting regional differences. As the CoMiSS™ was assessed in a presumed healthy population, it has been previously hypothesized that differences in the perception of various symptoms may be responsible for such differences. For example, it is known that the perception of infant crying differs between populations [5]. In both studies, the CoMiSS™ data from formula- and breastfed infants were obtained. Compared with the study by Vandenplas et al. [4], in the present study, we found differences in CoMiSS™ values between exclusively breastfed, exclusively formula-fed, and mixed-fed infants. However, the number of participants in the exclusively formula-fed and mixed-fed infants were small.
Other studies have assessed whether the CoMiSS™ can be used as a potential diagnostic tool in infants with suspected CMA. One of these studies was conducted in Indian children aged between 0 and 24 months. The positive and negative predictive values for the CoMiSS™ were 93% and 33%, respectively [6]. A second study was conducted in 38 Chinese children with suspected CMA. The authors of this study concluded that the CoMiSS™ may be useful in the diagnosis of CMA. However, they suggested that a CoMiSS™ cutoff score of ≥12 as the criterion for the early identification of CMA may be significantly high and suggested a cut-off of ≥6, at least in Chinese infants [7]. A single-blinded, prospective, multicenter trial involving infants that is validating the sensitivity and specificity of the CoMiSS™ against open oral food challenge is ongoing [8].
Limitations
Only two, well-child, primary pediatric care centers were involved in this study. While we recognize the value of random sampling, which involves random selection of the centers/participants, for pragmatic reasons, we used convenience sampling (i.e., the participants were selected based on their ease of recruitment). As with any cross-sectional study, our study is also subject to non-response bias, i.e., the participants/infants whose parents agreed to contribute may differ from those who were not approached, thus, the representativeness of the healthy infant population may be questioned. Only a small percentage of the infants were exclusively formula-fed; however, thelatter reflects a real-world situation in infants below 6 months of age in Poland.
Conclusions
This cross-sectional study adds to earlier age-related CoMiSS™ data by providing CoMiSS™ values in presumed healthy infants in Poland. Further studies in other populations are needed to establish normal CoMiSS™ values in various populations. Similarly, studies that assess the usefulness of the CoMiSS™ as a diagnostic and/or monitoring tool in children with CMA are needed.
 XML Download
XML Download