

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Constipation is among the most common conditions encountered by pediatric gastroenterologists. The vast majority of children who meet the criteria for functional constipation (FC) can be managed solely with medical therapies and do not require extensive workup [1]. When constipation becomes refractory to typical measures, further workup is recommended [2]. Two major components of this workup are the Oral-anal Transit Test (OTT) which measures the transit time of radio-opaque markers through the alimentary tract and colonic manometry (CM) which evaluates the neuromuscular integrity of the colon. The OTT is inexpensive, safe, and widely available, whereas CM is more invasive and expensive, and although a growing number of motility centers exist, there are still relatively few [34]. Other methods of transit measurement including wireless motility capsule and colonic scintigraphy suffer from a lack of data or standardization in children [5]. Given its simplicity, maximizing the information gained from the OTT is of interest to the practicing gastroenterologist. Recent guidelines do not support the routine use of the OTT in the evaluation of FC and its role in the evaluation of refractory pediatric constipation has not been directly addressed, but the adult literature advocates for the use of OTT in guiding therapy for constipation [25]. CM is clearly recommended in the evaluation of intractable constipation in children [2] and is advocated as a guide for surgical therapies for intractable constipation [467].
Limited data exists regarding the correlation of the OTT to CM or its ability to help pediatric gastroenterologists determine which patients would benefit from early referral to a motility center. A recent study by Tipnis et al. [8] addresses this issue. They studied the ability of the OTT to predict CM results. They found that all patients with normal transit had normal CM. This could lead to the conclusion that patients with normal OTT do not need CM. However, in this study the definition of a normal CM only required that High Amplitude Propagating Contractions (HAPC) propagate over 30 cm of colon. In children, this may represent an HAPC propagating only through the transverse or descending colon. While up to 95% of naturally occurring HAPCs do not reach the rectum, a normal CM is defined by the American Neurogastroenterology and Motility Society/North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition consensus statement as the presence of at least one HAPC propagating through the sigmoid colon [49]. Therefore, it is possible that some patients with a normal OTT might actually have an abnormal CM. Furthermore, we know that some patients with outlet dysfunction also have slow transit [5] and no data exists on which patients with an abnormal distal collection of markers might have colonic dysmotility on CM.
The primary aim of this study is to evaluate the ability of the OTT to predict results of CM using the definition of a normal HAPC as one propagating through the sigmoid colon.
Go to : 
MATERIALS AND METHODS
Patients
This retrospective study was approved by the Institutional Review Board of Atrium Health Levine Children's Hospital (IRB No. 05-16-34E). We identified all patients who underwent CM between August 2009 and December 2018 for any indication. Their records were retrospectively reviewed to identify which of those patients also had an OTT study done. Patients were excluded if the OTT was not done within 6 months of the CM.
Oral-anal Transit Test
Patients were administered a Sitzmarks capsule (Konsyl Pharmaceticals, Easton, MD, USA) containing 24 radio-opaque rubber rings. If not able to swallow the capsule whole, the capsule was opened and the rings sprinkled on applesauce. Patients with palpable impaction received a large volume cleanout and/or enema therapy prior to capsule ingestion, and the capsule was not administered until after impaction clearance was demonstrated radiographically. Patients were encouraged to stop all laxatives, but allowed to continue osmotic laxatives. Stimulant laxatives were held. A single view abdominal radiograph was obtained 5 days (120 hours) after capsule ingestion occurred. Consistent with published protocols, OTT was defined as abnormal if six or more markers remained [58]. The number and most proximal extent of any remaining markers were recorded based on plain radiographic location as ascending (including hepatic flexure), transverse, descending (including splenic flexure), or rectosigmoid colon.
Colonic manometry protocol
Patients were admitted for bowel preparation between 24 and 72 hours prior to the procedure, depending on severity of constipation. All cleanouts consisted of Polyethylene Glycol 3350 with electrolytes via nasogastric tube and oral laxatives. If tube placement was not tolerated, Polyethylene Glycol 3350 was administered orally.
On the morning of the CM, patients underwent colonoscopy under general anesthesia. Propofol and/or inhaled anesthetics were utilized but narcotics, benzodiazepines, antiemetics, and muscle relaxants were prohibited. Once the cecum was reached, a guidewire was advanced through the colonoscope, and the colonoscope was removed under fluoroscopic guidance. Then a single-use water perfused CM catheter consisting of 8 sensors spaced 5, 10, or 15 cm apart was advanced over the guidewire until the tip of the catheter was as far proximal as possible. Then the guidewire was removed and the catheter secured in place.
Once the patient was awake and alert, they were transferred to their hospital room and the catheter was connected to the recording system (Laborie, Mississauga, ON, Canada). The catheter was perfused with sterile water at 0.15 mL/second/sensor. The study was conducted for 6 hours as per published guidelines [4]. There were at least 60 minutes from the conclusion of the catheter placement until the start of recording. Fasting and postprandial motility were monitored for at least 90 minutes. An abdominal radiograph was obtained prior to Bisacodyl administration to document catheter position. At least 5 hours into the recording, the patient received 2 doses of Bisacodyl via the central lumen of the motility catheter (0.2 mg/kg of a 2 mg/mL compounded solution, max dose 10 mg) spaced 30 minutes apart.
An HAPC was defined as a contraction attaining at least 60 mmHg, lasting at least 10 seconds, traversing at least 30 cm in length [910]. The most distal segment of colon through which the HAPC propagated was recorded after viewing sensor location on a plain radiograph obtained during the CM study. A CM was considered normal if there was at least one HAPC progressing through all sigmoid sensors during the study, and if an HAPC did not progress through all sigmoid sensors, even if greater than 30 cm in length, it was considered incomplete, and thus abnormal [4]. We hypothesize that using this more widely accepted definition of a normal HAPC will identify colonic dysmotility in those CM which may have been previously read as normal [8]. Although there is no definitive definition of colonic inertia on CM in existing literature, we defined colonic inertia as a lack of HAPC propagating past the ascending colon. Patient demographics and clinical history were recorded. Descriptive statistics were utilized.
Go to :
RESULTS
Thirty-four patients underwent both OTT and CM for intractable constipation +/− fecal incontinence (44% male, age 4–18 years, mean 11.5 years). All except one patient (Hirschprung's Disease) had a diagnosis of FC+/− fecal incontinence. No patients had spinal dysraphism, imperforate anus, or any known underlying neuromuscular disease. All patients were seen and formally evaluated by the lead author prior to undergoing CM and were deemed to be refractory to medical management. All patients were treated with combinations of osmotic and stimulant laxatives, and all had either an enema or suppository as part of their management at some point. None had been on a formal trans-anal irrigation program or had been treated with anal sphincter botulinum toxin. Twenty-seven patients had abnormal OTT (79.4%) and 23 patients had abnormal CM (67.6%). Of the 11 patients with a normal CM study, 6 had a normal OTT (54.5%). Of the 23 patients with an abnormal CM study, only one had a normal OTT (4.3%). The most common abnormal CM finding was isolated sigmoid dysfunction (arrest of HAPC in the distalmost descending colon sensor or the proximal most sigmoid colon sensor). The site of manometric dysfunction stratified by OTT result is shown in Table 1.
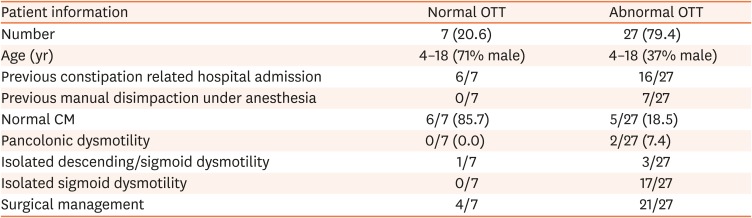
Table 1
Demographics and CM results stratified by OTT results
Values are presented as number (%), range (mean), or number only.
CM: colonic manometry, OTT: Oral-anal Transit Test.
![]()
Normal Oral-anal Transit Test patients
Seven patients had a normal OTT. Of patients with a normal OTT, 4/7 had no markers remaining at day 5, with the other 3 patients having between 1 and 4 markers remaining in the rectum. Of normal OTT patients, 6/7 (85.7%) had a normal CM. The normal OTT patient with an abnormal CM had arrest of HAPC in the proximal descending colon.
Abnormal Oral-anal Transit Test patients
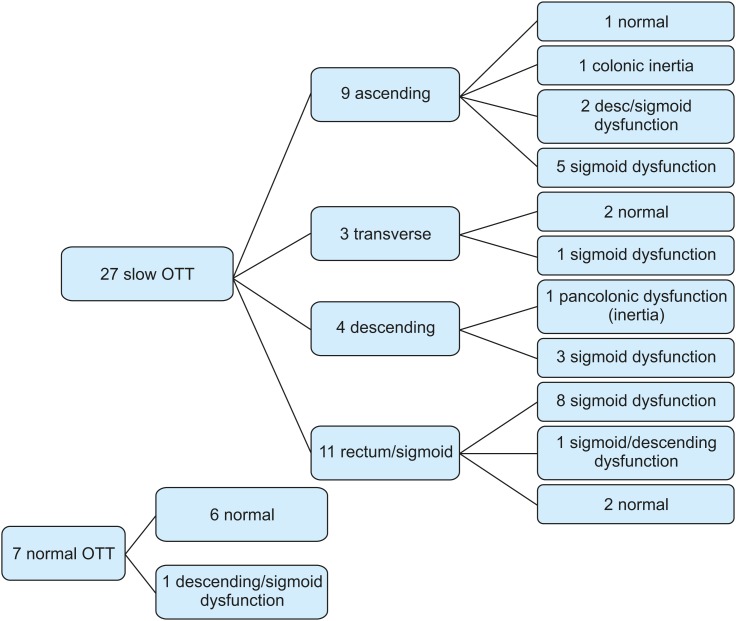
Twenty-seven patients had slow transit on OTT, most commonly between 19–24 markers remaining. Of the 27 abnormal OTT patients, 19% had normal CM. As the number of markers remaining increased, the likelihood of an abnormal CM increased (Table 2). Of the 27 abnormal OTT patients, the most proximal extent of any remaining marker was most commonly recto-sigmoid colon (41%) followed by ascending (33%), descending (15%) and transverse colon (11%).

Fig. 1 depicts manometry results stratified by most proximal extent of remaining radio-opaque markers. When all markers progressed to at least the sigmoid colon, this was 100% predictive against colonic inertia on CM. The combination of greater than 6 markers remaining with the most proximal extent in the ascending colon was 100% predictive of an abnormal CM. All patients with colonic inertia had a least 23 markers remaining. The proximal extent of remaining markers alone was not a good predictor of CM. Further analysis of the subgroup of patients with isolated sigmoid dysfunction on CM shows that of the 17 patients with isolated sigmoid dysfunction, only 8 (47.1%) had all remaining markers confined to the sigmoid or rectum, with the other 53% having markers as proximal as the ascending [5], transverse [1] or descending colon [3].
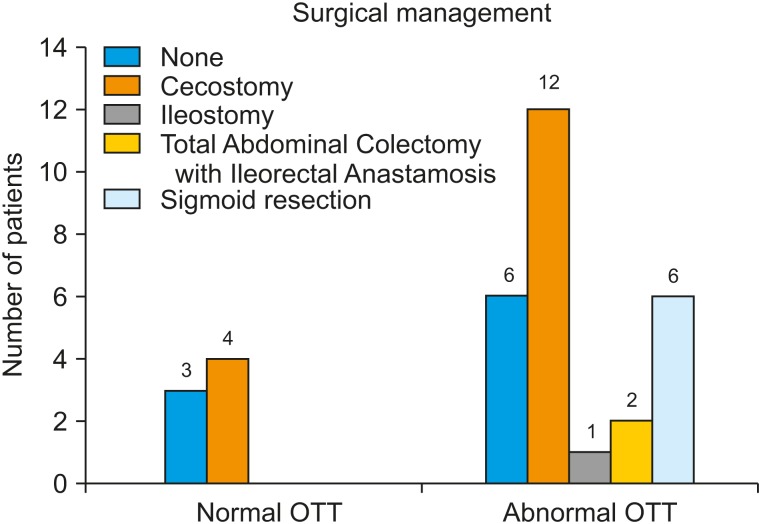
Surgical management
Seventy-four percent of the study population were surgically managed. 4/7 patients (57.1%) with normal OTT and 21/27 patients (77.8%) with abnormal OTT had surgical management. Of abnormal OTT patients, 80.0% (4/5) with normal CM and 77.3% (17/22) with abnormal CM had surgery. No patients with normal OTT had bowel resection. See Fig. 2 for description of surgical management of abnormal OTT patients. Of note, of the 6 patients who had a sigmoid resection, 5 had markers remaining proximal to the sigmoid colon, but all 6 patients had isolated sigmoid colonic dysfunction on CM.
Go to :
DISCUSSION
When constipation becomes intractable, there is significant variability in workup and management including the use of OTT and CM [111213]. Due to the limited availability, cost, and invasiveness of CM, maximizing the yield of noninvasive tests like OTT to guide therapy for refractory constipation would be of great interest to practicing gastroenterologists. OTT and CM give us different information. OTT gives us ‘real world’ information about transit as opposed to CM that studies an empty decompressed colon not subject to a typical stool burden or gaseous distension. Therefore, one might conclude that OTT is a more useful marker of colonic function. However, CM is used to guide surgical management [7].
A normal OTT has been thought to represent normal colonic transit. A distal collection of radio-opaque markers in the rectum or rectosigmoid most likely represents outlet dysfunction or dys-synergic defecation as the primary pathology, and markers scattered through the colon represents slow transit constipation (STC) or colonic inertia [5141516]. However, some studies have shown that over 50% of patients with dys-synergic defecation also have slow transit, therefore results of OTT are still nonspecific and suffer from lack of standardization in interpretation [5]. Our study shows that a distal collection of markers on an abnormal OTT is often associated with impaired neuromuscular integrity of the colon. Whether or not this neuromuscular dysfunction is a primary problem or whether secondary to colonic distension and tension from longstanding stool with-holding remains unknown.
The ability of OTT to predict CM has been infrequently studied. King et al. [17] described decreased presence of HAPCs in children with slow transit but STC was diagnosed with scintigraphy that is rarely used in clinical practice, and all patients already had a functioning cecostomy, so their results cannot be directly compared to our study. Giorgio et al. [16] found that in STC patients, there were fewer HAPC's propagated past the descending colon and a higher incidence of simultaneous contractions as compared to controls. However, no specific information was available about the distribution of markers and their ability to predict these findings. Tipnis et al. [8] found that no patients with normal OTT had abnormal CM, and 53% of patients with abnormal OTT had normal CM. We found a higher rate of abnormal CM in patients with abnormal OTT, likely because we required HPAC propagation through the sigmoid colon for normal CM. The previous study might underestimate the prevalence of clinically significant distal colonic dysmotility.
We found that all markers progressing to at least the sigmoid colon essentially ruled out colonic inertia but the most proximal extent did not predict segmental abnormality. Greater than 6 remaining markers with the most proximal extent being the ascending colon ruled out the possibility of normal CM. No patients with less than 23 markers remaining had colonic inertia; however, colonic inertia does not preclude markers progressing as far as the left colon. Overall the location of markers cannot be used to predict segmental dysmotility with enough accuracy to obviate the need for CM. The higher the number of markers remaining, the more likely there will be an abnormal CM. However, the most proximal extent of remaining markers does not predict the extent of the manometric abnormality. In addition, a distal collection of markers more often than not represented an actual dysmotility, not just outlet dysfunction. Eight-two percent of patients with and abnormal manometry study with markers remaining only in the rectosigmoid had an abnormal CM study (Fig. 1).
Intriguing but beyond the scope of this article is why patients with a normal OTT and/or a normal CM have clinically intractable constipation. It shows the multifactorial nature of refractory constipation; that there are likely environmental, behavioral, and yet unknown pathophysiological mechanisms behind refractory constipation that these studies cannot discern.
This study has several drawbacks including its retrospective nature, the relatively small number of patients, and the fact that only 25% of our CM population had an OTT. Part of the reason for the low percentage may be that we did not start to use OTT more widely until several years into the study period. However, despite the small number of patients, it is still the largest study to directly compare OTT and CM results. Furthermore, we performed CM the same day as catheter placement under anesthesia. There are conflicting reports on this, but at least one study supports this practice [18]. For OTT, we chose the day five X-ray to assess colonic transit, but this method is not validated as the gold standard. Other methods exist, including the Metcalf method, but we chose the day five X-ray due to its simplicity, tolerability, lack of repeated radiation exposure, and because this method most closely approximates the method used by Tipnis et al. [8] which is the study most closely resembling this study [5]. We encouraged the discontinuation of all laxatives during the OTT, but we did allow osmotic laxatives while undergoing OTT if parents insisted, which could underestimate abnormal results. One major drawback of our study was the lack of performance of unsedated anorectal manometry to formally assess defecation dynamics, therefore we cannot comment on the effect that dys-synergic defecation might have had on the OTT or colonic motility.
In conclusion, OTT and CM are both valuable tests but they are assessing two different aspects of colonic function. OTT can be used as a screening test to rule out colonic inertia. However, the location of remaining markers can not be used to clearly predict the location of any potential manometric abnormality, therefore, before any type of surgical resection is intertained, CM is necessary to identify the extent of the manometrically abnormal colonic segment. Due to the small numbers of patients in this study further research is warranted to confirm our results.
Go to :
 XML Download
XML Download