

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Celiac disease (CD) is caused by an abnormal immune response to gluten ingestion in genetically susceptible individuals. It affects approximately 1% of the general population and has a myriad of presentations ranging from asymptomatic patients to those with diarrhea, malabsorption, and failure to thrive [123].
Hepatitis B virus (HBV) is one of the common causes of chronic infectious liver injury worldwide. Universal immunization has played an important role in decreasing the burden of chronic HBV infection. A hepatitis B surface antibody (HBsAb) concentration below 10 mIU/mL is considered low and may be inadequate to protect the individual against HBV infection [45].
When comparing patients previously immunized with the standard HBV vaccine schedule, CD patients were found to have significantly higher rates of low HBsAb concentrations as compared to controls [678]. Our aim was to assess whether HBsAb concentrations measured in pediatric CD patients currently in serological remission on gluten-free diets (GFDs) differed from those in patients not yet on GFDs.
MATERIALS AND METHODS
We retrospectively reviewed the electronic medical records of pediatric CD patients from two tertiary medical centers in Israel, Schneider Children's Medical Center (Petah-Tikva, Israel) and Shaare Zedek Medical Center (Jerusalem, Israel). All CD patients were diagnosed according to guidelines published by the European Society for Pediatric Gastroenterology Hepatology and Nutrition [9]. Adherence to GFD and serologic remission status were assessed by reviewing physician notes in the medical records and of bi-annual celiac serology measurements.
All participants had been immunized as infants with a standard 3-dose regimen (0, 1, 6 months old) using a recombinant DNA vaccine (Engerix-B Peds; GlaxoSmithKline, Rixensart, Belgium). None had received a booster dose between the initial immunization and testing for HBsAb concentration. We examined hepatitis B surface antigen and HBsAb levels in all participants to ascertain that patients did not have HBV disease.
We examined the HBsAb concentrations for all patients and compared those who were tested for HBsAb concentration prior to GFD onset (usually at diagnosis) and those who were tested after initiation of the elimination diet, while accounting for GFD adherence.
Statistical analysis
The data were analyzed using BMDP software (BMDP Statistical Software, 1993; University of California Press, Los Angeles, CA, USA). Pearson's chi-square test or Fisher's exact test (two-tailed) was used for analysis of between-group differences in discrete variables, and analysis of variance (ANOVA) was used for continuous variables, using the Brown-Forsythe calculation when Levene's test indicated a significant difference between the variances. In order to adjust for the effect of age and sex, we used Analysis of Covariance (ANCOVA) to compare equality of adjusted means. The HBsAb concentrations were found to have a non-Gaussian distribution, so a log-transformation was applied to HBsAb concentration, which enabled us to calculate the Pearson's correlation between age and log (HBsAb). A p-value of ≤0.05 was considered significant.
Approval for this retrospective chart review was granted by Rabin medical center's institutional review board.
RESULTS
Overall, 413 CD patients were evaluated, of which 156 underwent hepatitis B serology testing before GFD initiation and 257 were tested after initiation of GFD. None of the subjects had a history of past HBV infection or evidence of HBV disease. Adherence to GFD could not be ascertained for 20 subjects, due to lack of serological tests or inadequate data on GFD adherence, and these subjects were thus excluded. An additional 20 (8.4%) subjects on GFD were not yet in serological remission and were therefore also excluded from the analysis. Finally, 217 GFD-compliant CD subjects were included in the analysis (Table 1).
Table 1
Patient characteristics and HBsAb concentration
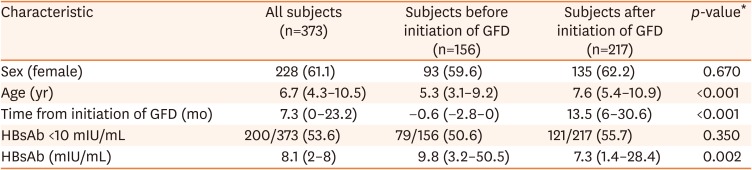
Low HBsAb concentration rates were similar between those tested before and after GFD initiation (p=0.350). When considering only those on the GFD for more than a year, HBsAb concentration was low in 74 of 119 (62.2%) participants. When comparing this subgroup to those tested prior to initiation of GFD, this difference was not statistically significant (p=0.060). ANCOVA showed that the only factor that correlated with HBsAb concentration was age at the time of HBsAb testing, with an inverse association. Neither GFD status nor sex showed any significant association.
DISCUSSION
Our study found that in previously vaccinated pediatric CD subjects, being in clinical remission on a GFD did not influence the rates of low HBsAb concentrations. This lack of association remained even when considering only subjects adhering to a GFD for more than a year. Age at the time of HBsAb measurement was the only variable that correlated inversely with HBsAb concentration in our cohort.
Although the average absolute HBsAb concentration was higher in CD subjects prior to initiation of GFD, these subjects were also significantly younger than those already on GFD. Several studies have demonstrated that HBsAb levels decline with time from immunization [10111213]. Indeed, our data corroborate this finding in pediatric CD subjects.
Prior to conducting this study, we hypothesized that at the time subjects had active intestinal inflammation due to undiagnosed CD, measured HBsAb concentrations would be low, but that in subjects who are in remission under a GFD, the concentrations would be higher. Possible explanations for this would be either loss of protective antibodies through an inflamed small bowel or decreased production by immune memory cells. A study by Ertekin et al. [7] has shown higher rates of low HBsAb in previously immunized CD not adherent to GFD compared to GFD adherent subjects. Our study, however, did not demonstrate a difference between those who were adherent to GFD and those tested before GFD initiation.
While low HBsAb levels discovered years after vaccination could be explained by poor response to the vaccine itself, one should also consider whether CD subjects have a different response to the vaccine as compared to healthy subjects. However, in several re-vaccination studies, both CD subjects and controls were found to have a similar response [1415]. Moreover, Nemes et al. [16] has shown poor response to primary immunization in CD subjects prior to GFD initiation compared to CD subjects adherent to GFD as well as to controls. They concluded that the carriage of human leukocyte natigen (HLA)-DQ2 by itself does not impair the immunological response. However, in CD patients consuming gluten, the saturation of HLA-DQ2 with gliadin may decrease the binding of the HBV vaccine antigen, thus negatively affecting T-cell activation and the subsequent B-cell antibody production. In our study all subjects were immunized at infancy, with at least two doses prior to gluten exposure and development of CD. Hence, it may be plausible that they experienced the same response rate as other infants.
An important limitation of our study stems from its retrospective design. We cannot confirm that all subjects indeed responded to the primary immunization schedule in infancy, nor could we perform serial testing of HBsAb concentrations to evaluate the decline of HBsAb concentration over time for each patient. Likewise it was not possible to tell whether there was any loss of formed antibodies through the inflamed mucosa in our subjects.
In conclusion, our study has demonstrated that adherence to GFD and being in serologic remission does not affect HBsAb concentration in children with CD. Since older age is the only factor associated with declining HBsAb concentrations, studies assessing the presence of memory B cells in CD patients lacking protective concentrations may help to assess the need for and type of re-vaccination schedules.
 XML Download
XML Download