

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Epinephrine is widely used for the treatment of severe anaphylactic reactions in the form of epinephrine-containing autoinjectors. There are risks of incorrect use or accidental injections of epinephrine. Injection into digits where terminal arteries are distributed can result in vasoconstriction, which can cause severe digital ischemia, followed by pain, numbness, deepithelialization, wound infection, and potential necrosis.
To reverse epinephrine-induced digital ischemia, phentolamine is a well-established specific competitive antagonist1. However, for many reasons, this drug is not available at all hospitals for the emergency treatment of epinephrine-induced digital ischemia. Since pure phentolamine was not available at our institution, Standro (1 mL; phentolamine mesylate 0.6 mg, alprostadil 6 µL, papaverine 17.64 mg; Shin Poong Pharm. Co., Seoul, Korea), which is used to treat erectile dysfunction, was used as an alternative.
Although there are several reports of the use of phentolamine as an antidote for epinephrine234, the use of a phentolamine-alprostadil-papaverine complex has not been reported to date. We discuss a case of infiltration of the phentolamine complex solution into the puncture site for the successful reversal of the local ischemic effects of epinephrine.
CASE REPORT
The consent for the publication and the use of her images was obtained from the patient's guardian. This report does not contain any personal information that could lead to the identification of the patient.
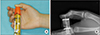
A 12-year-old girl accidentally injected epinephrine into her right thumb using an auto-injector, Epi-Pen (0.3 mL, 1:1000 epinephrine; Dey Laboratories, Napa, CA, USA). One hour later, she arrived at the emergency department. The Epi-Pen was still embedded in the volar pulp of the thumb on arrival and she complained of pain and numbness in the injected finger. The entire distal phalanx and distal half of the proximal phalanx were pale and cold compared to the other fingers, and the skin did not blanch in response to pressure (Fig. 1).
In the emergency room, the patient's body temperature was 36.5℃; blood pressure, 100/60 mmHg; pulse rate, 97 beats per minute; respirations, 20 breaths per minute; and peripheral capillary oxygen saturation, 95%. She did not claim any underlying diseases, including vasoconstrictive disorders, thrombotic disorders, or a previous surgical history of the digits.
Two hours later, an attempt was made to remove the Epi-Pen in the emergency room, but only the frame was removed, while the needle remained. We decided to remove the remaining needle in the operating room under C-arm guide in case it penetrated the cortical bone (Fig. 2).
Three hours after the initial injection, a brachial plexus block was provided in the operating room for anesthesia and also for sympathetic blockade of upper extremity vessels to increase blood flow to the fingers. The needle was removed successfully, but the thumb was still pale and cold compared to the adjacent finger, and no capillary filling was present. Attempts to obtain Doppler pulses, and peripheral capillary oxygen saturation from the pulse oximeter both failed (Fig. 3).
A temporary thumb spica splint was applied to immobilize the thumb. Then, 1 mL of Eglandin (alprostadil 10 µg; Mitsubishi Tanabe Pharma Korea Co., Seoul, Korea) was administered intravenously for the vasodilation of peripheral vessels. Furthermore, an infrared heat lamp was used to prevent a drop in temperature, which can lead to vasoconstriction.
At 4.5 hours after the initial accident, there were still no improvement in blood flow in the thumb. Although phentolamine is effective for reversing epinephrine-induced digital ischemia, it was not available at our institution in an emergency setting. However, Standro (a phentolamine-papaverine-alprostadil complex), a drug used for erectile dysfunction, was available immediately.
After the placement of 0.1 mL drop of Standro solution directly on the punctured wound, circulation immediately returned, as evidenced by the pink coloration. Although the thumb was still cold and residual numbness remained, the patient reported a marked decrease in pain.
A 6.5 hours later, a physical examination showed normal sensation and warmth of the thumb (Fig. 4). The patient was discharged the next day with only mild tenderness on her fingertip. One week after the injection, the punctured wound healed without remarkable sequelae. A physical examination showed a normal range of motion of the thumb, normal sensation, and an absence of pain or tenderness (Table 1).
DISCUSSION
Epinephrine is a sympathomimetic catecholamine that acts to increase peripheral resistance via α1 receptor-dependent vasoconstriction. It is frequently used to treat anaphylactic reactions to bee stings, status asthmaticus, and other types of anaphylaxis1. It can also be used in local anesthesia in wide-awake hand surgery56. For anaphylaxis and asthma, 0.3 mg of epinephrine is conventionally used (0.3 mL, 1:1000 dilution) and autoinjectors are commonly carried by patients with severe allergies. However, the accidental discharge of epinephrine into a digit with terminal arteries may cause profound vasoconstriction, followed by prolonged ischemia, which can lead to skin sloughing, infection, and ischemic necrosis.
Phentolamine is a nonselective α-adrenergic antagonist that binds to postsynaptic α-adrenergic receptors. This interferes with catecholamine activity and thereby causes vasodilation due to α1 blockade178. In addition to epinephrine-induced digital ischemia2349, phentolamine is used to treat a diverse group of conditions, including hypertensive emergencies, pheochromocytoma, cocaine-induced cardiovascular complications, erectile dysfunction, and reflex sympathetic dystrophy. However, phentolamine may induce severe hypotension due to its peripheral vasodilatory properties and its routine practical use is limited7. Phentolamine reverses the effects of epinephrine when administered by several methods, including direct infiltration at the injected site, injection along the digital arteries, and the standard digital block technique. Digital ischemia has been treated using 0.5–2.5 mg of phentolamine2349. Patients treated with up to 10 mg of phentolamine do not develop hemodynamic changes210. In our case, 0.1 mL of Standro contained 0.06 mg of phentolamine, 0.6 µL of alprostadil, and 1.76 mg of papaverine. Both phentolamine and alprostadil were within safe dosage for children. Although a safe dosage of papaverine for children has not been established yet, a drop of solution at the focal wound did not seem to influence systemic adverse effects.
Standro is a mixture of phentolamine, alprostadil, and papaverine. It is administered via intracavernosal injection in patients with erectile failure. Alprostadil (prostaglandin E1) and papaverine both have vasodilatory properties by relaxing vascular smooth muscles1. These similar effects on vessels may explain the synergistic effect in our case, despite the very small amount of Standro solution.
Before administering phentolamine, we attempted to restore blood flow using an infrared heat lamp, warm water immersion, intravenous administration of prostaglandin E1, and the sympathetic blockade of vessels of upper extremity during brachial plexus block. Nonetheless, none of these approaches was effective. Moreover, Hinterberger and Kintzi3 reported that amyl nitrite inhalation, metacarpal nerve block, and topical nitroglycerin paste are ineffective.
In conclusion, in a case of the accidental injection of epinephrine into a digit, profound ischemia was quickly and safely reversed by the local administration of Standro (a phentolamine complex) to the area of accidental injection. Accordingly, when pure phentolamines are unavailable, an alternative phentolamine-containing complex may be a good option for treatment. Furthermore, with the growing interest in local anesthesia in wide-awake hand surgery, these experiences may aid in reversing of unexpected vasospasm issues. In cases of wide-awake hand surgery with 1:100,000 concentrations of epinephrine, although temporary circulatory issues may occur, they often resolve without the need for phentolamine rescue56. However, reverse treatment should be prepared in patients with known peripheral vascular disease, diabetes, Raynaud's phenomenon, Berger's disease, calcinosis, sclerodactyly, or other conditions that may adversely affect the perfusion of the digits.




 XML Download
XML Download