

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Tobacco use remains a common habit with increasing numbers worldwide. Although there has been a steady global reduction in the prevalence of daily smoking since 1980, a significant elevation in the number of smokers has been reported concurrently due to population growth.1) In particular, Korea is a country with a high prevalence of daily smoking and high cigarette consumption.1) Cigarette smoking is a well-known risk factor of the progression of cardiovascular diseases (CVDs),2) and arterial stiffness may play a underlying pathophysiological mechanism.3)
Smoking is a modifiable lifestyle risk factor for CVD unlike the other risk factors, such as age, sex, and ethnicity.4) Cigarette smoking is related with arterial stiffness,3) however, the effect of smoking cessation on arterial stiffness has not been clarified. One UK study reported a significant reduction in augmentation index (AIx) in successful quitters 4 weeks after smoking cessation compared to relapsed smokers.5) In contrast, no significant difference was investigated in brachial-ankle pulse wave velocity between baseline and 12 months later in a Chinese primary care clinical study.6) Another Netherland study reported 2 years of smoking cessation did not significantly affect to a lower progression in intima-media thickness nor to an improved results of dynamic vessel wall properties.7) It remains unclear whether smoking cessation is protective for the development of the arterial stiffness.
Therefore, this study aimed to investigate whether there is an association between smoking cessation and arterial stiffness assessed using radial AIx, an estimate of vascular wave reflection and provides a comprehensive assessment of arterial stiffness.
METHODS
The Cardiovascular and Metabolic Diseases Etiology Research Center (CMERC) study constructed 2 prospective cohorts, a cohort consisting of a general population (the CMERC cohort) and high-risk patients (CMERC-HI cohort). This cross-sectional study obtained baseline data from the CMERC cohort. Korean adults aged 30–64 years who were free of myocardial infarction, heart failure, or stroke participated in this study. All participants completed health questionnaires and examinations. The sampling and measurement procedures in the CMERC cohort have been described in detail previously.8) Data were collected from 4,060 participants (1,426 men, 2,634 women) between the 2013 and 2017 baseline survey and final analyses were available for 1,169 men. Women were excluded due to the small number of smoking history (n=2,634). Participants taking antihypertensive drugs (n=254) due to its effect on blood pressure and those for whom key variables were missing (n=3) were also excluded.
Information on demographic health-related behaviors and medical history were obtained based on participants' self-reports through a face-to-face interview. Physical activity was evaluated using the International Physical Activity Questionnaire-Short Form - Korean version,9) which consists of walking frequency and duration, moderate-intensity activity, vigorous activity, and sedentary activity during the past 7-day. Participants were stratified into 3 groups based on sedentary time (<4, ≥4 and <7, ≥7 hours/day). Participants were classified as current regular alcohol drinkers, former drinkers, or non-drinkers. History of diseases such as diabetes and hypertension was identified through self-reporting of a physician's diagnosis. Current medication information was also obtained from the participants. People using anti-hypertensive medications were not included for the present study. Physical examinations including measurements of body size, composition, and blood pressure were conducted by trained research personnel. Participants rested for ≥5 minutes before the blood pressure measurement, and systolic blood pressure (SBP) and diastolic blood pressure (DBP) were repeatedly measured 3 times at 2-minute intervals in the right arm using an automated oscillometric device (HEM-7080; Omron Health, Matsusaka, Japan). The mean blood pressure of second and third-time measurements was used in the analysis. Pulse pressure (PP) was attained from the difference between SBP and DBP. Biochemical analyses of a fasting blood sample were assessed in the baseline CMERC cohort.
All participants were interviewed using standardized questionnaires to obtain information regarding cigarette smoking. Trained interviewers conducted face-to-face interviews and questionnaire surveys according to the protocol. Details about lifetime smoking experience, current smoking, and smoking amount and duration were obtained from individuals. Smoking status was self-reported as current, former, or non-smoker. Former smokers were categorized into 3 subgroups according to years since smoking cessation: < 1, 1 to <10, and ≥10. The cumulative smoking exposure (i.e., smoking pack-years [SPY]) was calculated from self-reports of cigarette smoking from the questionnaire. Cumulative smoking exposure was estimated as daily packs smoked multiplied by the number of years smoked.
Arterial stiffness was assessed by radial AIx, which was calculated using a non-invasive device (HEM-9000AI; Omron Healthcare Co., Ltd., Kyoto, Japan). The participants were asked to assume a seated position after taking at least a 5-minute rest and remain still and relaxed during all measurements. Radial AIx was calculated as follows: (Second peak SBP−DBP)/(First peak SBP−DBP)×100 (%).10)
Since radial AIx was affected by heart rate, the index was corrected to 75 beats/minute. Waveform data were confirmed by well-trained technicians.
Statistical analyses
We used the analysis of variance for normally distributed continuous variables, the Kruskal-Wallis test for skewed distributed variables, and the χ2 test for categorical variables to compare the demographic characteristic of individuals according to 5 smoking status groups. Adjusted means of AIx was attained from using analysis of covariance. First, the associations between smoking status (non-smokers [reference group], former smokers, and current smokers) and arterial stiffness, AIx, was investigated by multivariate linear regression. Adjustments were made for age, height, weight, SBP, DBP, diabetes diagnosis, low-density lipoprotein cholesterol, alcohol intake, and sedentary time. Second, subgroup analyses stratified by smoking status according to the duration of smoking cessation (non-smokers [reference group], former smokers [<1, 1 to <10, ≥10 years], and current smokers) were conducted. Third, whether there were multiplicative interactions between former smoking status and cumulative smoking exposure (SPY, continuously) or age (<55, ≥55) was investigated, and linear trends according to smoking status, from non-smokers to current smokers, were also examined.
We conducted several sensitivity analyses. First, we performed subgroup analyses to investigate cumulative smoking exposure. Former smokers were stratified into 3 groups according to tertile value of smoking pack-years (≤8, >8 and <20, and ≥20). Second, to examine whether our findings differed by the duration of smoking cessation, we applied various cutoffs. Third, to examine whether our findings differed from the participants who took anti-hypertensive medication, we included those participants in the analyses. Fourth, we conducted the analysis also for the female participants (n=2,257) after excluding the ones with taking anti-hypertensive medication. All statistical analyses were performed using SAS software version 9.4 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
The general characteristics of the study participants stratified by smoking status are presented in Table 1. The mean age of the former smokers (52.1 years) was higher than that of the non-smokers (47.8 years) and current smokers (45.7 years). Former smokers tended to have higher SBP, DBP, PP, and AIx values than the current and non-smokers. In addition, there was a linear trend of AIx according to smoking status.
Table 1
Descriptive characteristics of study participants

Values are presented as mean±standard deviation or number (%).
AIx75 = augmentation index adjusted for 75 beat/minute; BMI = body mass index; DBP = diastolic blood pressure; HbA1c = hemoglobin A1c; HDL = high density lipoprotein; LDL = low density lipoprotein; SBP = systolic blood pressure.
*Obtained from upper-arm blood pressure; †Hypertensive patients but not taking anti-hypertensive medication.
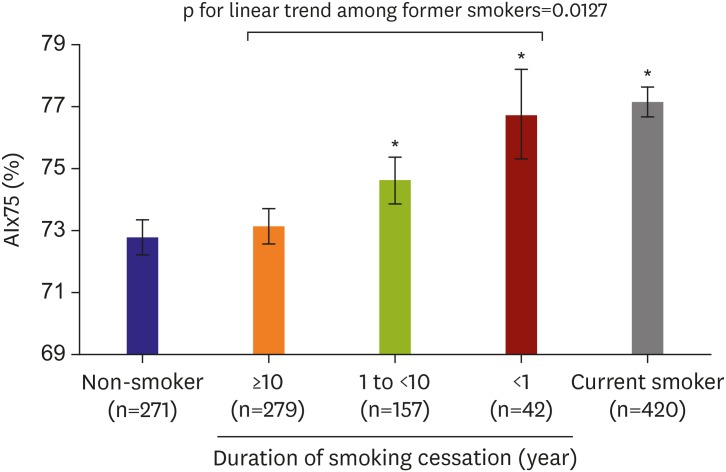
Table 2 presents the association between smoking status and arterial stiffness. Current smokers showed significantly higher AIx (β=4.34, standard error=0.74, p<0.001) compared to non-smokers, but not in former smokers (β=1.23, standard error=0.72, p=0.089). After considering duration of smoking cessation, the altered association was investigated between former cigarette smoking and arterial stiffness. A significant increase in AIx in individuals who quit smoking less than 1-year prior (β=3.94, standard error=1.54, p=0.011) and those with a duration of 1–9 years (β=1.87, standard error=0.94, p=0.047) compared to non-smokers. In addition, a linear trend of AIx according to smoking status considering the duration of smoking cessation was found (p<0.001). Figure 1 shows the adjusted mean AIx values according to the smoking status. There was a dose-response elevation of AIx that those who quit smoking for a shorter duration showed higher values. There were no significant multiplicative interactions between former smoking status and smoking pack-years (p=0.101) or age (p=0.366). In sensitivity analyses using cumulative smoking exposure, different durations of smoking cessation categorized by former smoking status, and including subjects taking anti-hypertensive medication, similar results were obtained (Supplementary Figure 1). In addition, the results of the female participants mostly aligned with those of the primary analyses except that former smokers less than a year showed a lower AIx value compared to non-smokers (Supplementary Table 1).
Table 2
Association between smoking status and augmentation index

Figure 1
Adjusted means of augmentation index according to smoking status. Adjusted for age, systolic blood pressure, diastolic blood pressure, height, weight, diabetes diagnosis, low-density lipoprotein cholesterol, alcohol intake, and sedentary time.
AIx75 = augmentation index adjusted for 75 beat/minute.
*Statistically significant compared to non-smokers (p<0.05).
DISCUSSION
The present study investigated that the AIx of former smokers did not differ significantly from that of non-smokers. However, the dose-response association between smoking cessation and AIx was revealed after considering the duration of smoking cessation. The shorter the duration after smoking cessation, the higher were the AIx values. In particular, participants who quit smoking less than 1-year prior showed similar AIx values to those of current smokers, while those who quit smoking more than a decade prior showed AIx values similar to those of non-smokers.
Arterial stiffness improved in former smokers according to cessation duration. In other words, former smokers who abstained from smoking for >10 years showed a reduction in arterial stiffness to the level of non-smokers, pointing toward improved vascular function. Although it is hard to conclude the definite duration of smoking cessation needed to reverse arterial stiffness, the longer duration of cessation seemed to benefit the arterial stiffness in our study. In our sensitivity analyses, various cutoffs of smoking cessation years were applied and ≥10 years of smoking cessation found to be the most similar level of AIx compared with that of non-smokers among various cutoff values. Our finding that former smokers with a longer duration of smoking cessation had a similar level of arterial stiffness compared to non-smokers is consistent with previous studies. According to the cross-sectional study of hypertensive patients, the duration of smoking cessation was significantly related to improvements in arterial stiffness including pulse wave velocity, AIx, and transit time.11) Another UK study of 20 patients who participated in the smoking clinic at a hospital found that successful smoking quitters had significant reductions in AIx after 4 weeks of tobacco smoking abstinence compared to relapsed smokers.5)
Arterial stiffness can be determined by 3 components of the arterial wall: first, quantitative structural components such as the proportion of elastin and collagen; second, qualitative structural components such as cross-linking of glycated collagen; and third, functional components such as vasoconstrictor tone exercised by smooth muscle cells.4) Smoking can affect every physiological aspect of arterial stiffening through many potential mechanisms, such as endothelial dysfunction, increased oxidative stress, and inflammation.2) A relevant mechanism related to the reversible smoking cessation effect is the autonomic nervous system (ANS) activated by smoking exposure.12) The elevated ANS is correlated with increased blood pressure and peripheral resistance, a result of the concurrent interaction with the weakened baroreflex sensitivity that accompanies aging.13) Through acute smoking exposure, nicotine leads to a predominance of sympathetic nerve activity12) that can contribute to the risk of peripheral vasoconstriction and an accelerated heart rate.14) Several studies in agreement with our result reported the possibility of a reversible effect of smoking cessation in relation to the sympathetic nervous system. Chronic habitual smokers15) and heavy smokers16) showed improved results in heart rate variability, a measure of the interplay between the sympathetic and parasympathetic nervous systems, within 7 days of smoking cessation. In addition, the sympathetic nerve activity patterns of former smokers were not distinguished from those of non-smokers, which had an implication that smoking effect may be reversible to the normalized sympathetic nerve activity.17)
The changeable effect of smoking cessation on arterial stiffness may also be explained by the role of nitric oxide synthesis related to the sympathetic nervous system.18) Impaired nitric oxide synthesis is reportedly a detrimental factor in the regulation of vasomotor tone and blood pressure19) through a loss of vasodilator tone at the vascular smooth muscle cells and by progressing central neural vasoconstrictor outflow.20) The central action of nitric oxide, reducing sympathetic vasoconstrictor outflow to the sympathetic neurons, and peripheral action of nitric oxide, directly decreasing peripheral vascular smooth muscle tone, contribute to vasodilation or decreased arterial stiffness.20) One study supports the fact that the effect of smoking cessation is correlated with a normalized nitric oxide level. By achieving smoking cessation, the plasma nitric oxide concentration in former smokers was not significantly different from that of the non-smokers.21) Another study reported that the elevated oxidative stress assessed by the level of nitric oxide gradually return to normal after a long period of smoking cessation.22) In addition, several studies reported the interactions between nitric oxide and cardiac autonomic control in animal data23) or human data.24) Nitric oxide appears to work as a sympatholytic agent,23) attenuating central sympathetic outflow and lowering cardiac responses to sympathetic stimulation.25) Considering the moderating role of nitric oxide on the sympathetic nervous system, it is reasonable to assume that there might be a reversible effect of smoking cessation on arterial stiffness through an ANS mechanism.
However, there are several limitations should be considered. First, as in all cross-sectional studies, we cannot conclude that there is a causal effect of smoking cessation on AIx. Unmeasured factors such as environmental smoking may be responsible for this relationship.26) Second, we utilized the radial AIx, a surrogate measurement of wave reflection. there are some data supporting that radial AIx reflects vascular stiffening and aging,10) it may not be considered as a standard measurement of arterial stiffness.27) Third, smoking information including current status, duration of smoking cessation, and the number of cigarettes smoked were self-reported, which might lead to some misclassification bias. However, the validity of self-reported smoking status had been proven through many studies.28)29) Fourth, the interpretation of results in this study is limited to male participants. However, in spite of the limited statistic power, we found a similar trend of results with primary analyses in sensitivity analyses with female participants. Fifth, the analyses were based on small numbers of former smokers who quit smoking more than 10 years prior, which limited the power of our statistical analysis. Finally, we found no study, in the literature, evaluating the simultaneous changes on nitric oxide synthesis and sympathetic nervous system, and this could limit our explanation of possible mechanisms.
We found a significant dose-response association between the duration of smoking cessation and AIx in male subjects recruited from the general population. Therefore, our findings may help inspire current smokers to modify their smoking habits to delay or reverse disease progression. Nonetheless, the effect of smoking cessation on arterial stiffness should be further evaluated in longitudinal studies in the future.
 XML Download
XML Download