

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asymptomatic carotid stenosis increases the annual risk of ischemic stroke involving the ipsilateral carotid artery territory by 2% to 5%.1) To prevent asymptomatic carotid stenosis from causing future ischemic stroke, carotid artery stenting (CAS) has been performed since its development in the 1990s as an alternative to carotid endarterectomy (CEA). According to recent treatment guidelines, prophylactic CAS is recommended for patients with stenosis greater than 60% and for those whose risk of late ipsilateral stroke is expected high while CEA is ineligible.2) However, the role of CAS in the management of asymptomatic carotid stenosis has not been thoroughly evaluated, especially compared to medical treatment (MT). Therefore, the objectives of this systematic review were 1) to combine evidence from randomized controlled trials (RCTs) and prospective or retrospective nonrandomized, comparative studies (NRCSs) that compared CAS and CEA for asymptomatic carotid stenosis using a Bayesian cross-design meta-analysis; and 2) to indirectly compare clinical effectiveness between CAS and MT using a Bayesian network meta-analysis.
METHODS
Data sources and searches
We searched the MEDLINE, Cochrane Library, and Embase databases from inception until December 31, 2017, for all comparative studies that compared between CAS and CEA, between CEA and MT, or between CAS and MT. We developed MEDLINE search strategy (Supplementary Table 1) and modified it for the other two databases appropriately. We also manually searched bibliographies of systematic and narrative reviews.
Study selection
We selected studies meeting the following pre-specified criteria: 1) the trial enrolled adults (aged 18 years or older) who had asymptomatic atherosclerotic narrowing of the lumen of the carotid bifurcation or the extracranial part of the internal carotid artery between 50% and 99%; 2) the trial enrolled patients without ipsilateral carotid territory symptoms within the preceding 6 months, and 3) the trial was a full-text English language paper published in a peer-reviewed journal. We accepted definitions of asymptomatic carotid stenosis used in each study. We excluded studies reporting mixed populations of symptomatic and asymptomatic patients when data were unavailable for each group separately. Trials for which the only abstract from conference proceedings was available were also excluded. We contacted authors of potentially relevant studies to clarify ambiguities on eligibility and to request relevant unpublished data. The Preferred Reporting Items for Systematic review and Meta-Analyses statement was followed.
Data extraction and quality assessment
Data were extracted into a structured data extraction form. The risk of bias was assessed using the Cochrane Collaboration tool for RCTs, and the Risk of Bias Assessment tool for Non-randomized Studies for NRCSs.
Data synthesis and analysis
Baseline demographics, trial design, and outcomes were extracted from each trial. To assess the safety of each treatment strategy, we reviewed information on myocardial infarction, stroke in any territory (ipsilateral of contralateral, major or minor) between randomization (index hospitalization for NRCSs) and 30 days after treatment. For patient who did not undergo carotid revascularization, this period was defined as the first 30 days after randomization, or according to the definition used in the trial. To evaluated combined safety and long-term efficacy, we also reviewed the composite of death, myocardial infarction, any stroke during periprocedural period, or ipsilateral stroke occurring thereafter, and ipsilateral stroke (including any stroke during the periprocedural period). Definitions of individual outcome followed those defined in each individual trial.
Statistical analysis
For RCTs, the intention-to-treat principle was followed whenever applicable. The longest available follow-up data from individual studies were used. To combine evidence from disparate sources (RCTs and NRCSs), a Bayesian cross-design analysis was used. In this analysis, we adopted a strategy to incorporate systematic difference of different study designs,3) by imposing prior constraints to random-effects models to reflect our prior opinions about designs, i.e., estimates from RCTs might be less biased than estimates from NRCSs and more weight should be assigned to evidence from RCTs than that from NRCSs. The model was depicted in detail in Supplementary Data. For additional analyses, not only a fixed-effect model, but we also used 2-level and 3-level hierarchical Bayesian models considering study-level and design-level random effects. A random-effect model involving an informative prior derived from the results of NRCSs was also used to combine evidence from RCTs and NRCSs. To compare clinical outcomes of these three different treatment strategies, we used the Bayesian network meta-analysis proposed by Lu and Ades4) In this analysis, we included only RCTs that compared between CAS and CEA, between CEA and MT, or between CAS and MT. Odds ratios (ORs) with 95% credible intervals (CrIs) was presented as summary statistics. To evaluate heterogeneity in outcomes between the two study designs (RCT and NRCS), we conducted an exploratory meta-regression analysis by adding the covariate of study design to the model. Non-informative prior distributions were selected to allow the data to dominate final results, unless otherwise specified. Data were analyzed with WinBUGS v.1.4.3 (MRC Biostatistics Unit, Cambridge, UK) and R programming. We ran Markov chain Monte Carlo samplers in WinBUGS, running three chains with different starting values. A burn-in phase of 20,000 iterations was followed by 50,000 updates, where the number of burn-in iterations was chosen according to Brooks-Gelman-Rubin method for convergence check. Pairwise ORs were estimated from the median of the posterior distribution with CrIs taken from 2.5 and 97.5 percentiles. Results were considered significant when CrIs of ORs did not include 1. For meta-regression, CrIs not including 0 were considered significant.
RESULTS
The search identified 10,154 citations. We evaluated the full text of 22 trials that met our eligibility criteria (Figure 1). There were 4 RCTs5)6)7)8) and 14 NRCSs9)10)11)12)13)14)15)16)17)18)19)20)21)22) that compared between CAS and CEA and 4 RCTs23)24)25)26) comparing between CEA and MT. However, for CAS versus MT, no RCT was found through our search strategy. Characteristics of relevant RCTs are shown in Table 1 and those of relevant NRCSs are shown in Supplementary Table 2. In each study, definitions of ‘asymptomatic status’ and procedural characteristics in each study was generally heterogeneous. Risks of bias for RCTs and NRCSs are summarized in Supplementary Tables 3 and 4, respectively.
Figure 1
Summary of evidence search and selection.
CAS = carotid artery stenting; CEA = carotid endarterectomy; CENTRAL = Central Register of Controlled Trials; MT = medical treatment; NRCS = nonrandomized comparative study; RCT = randomized controlled trial.
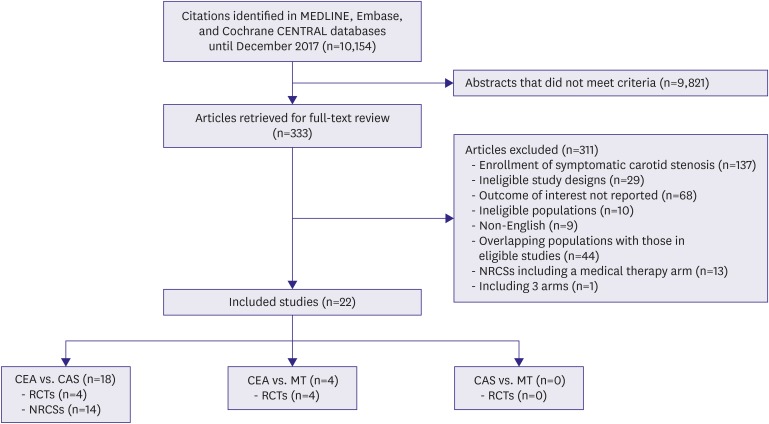
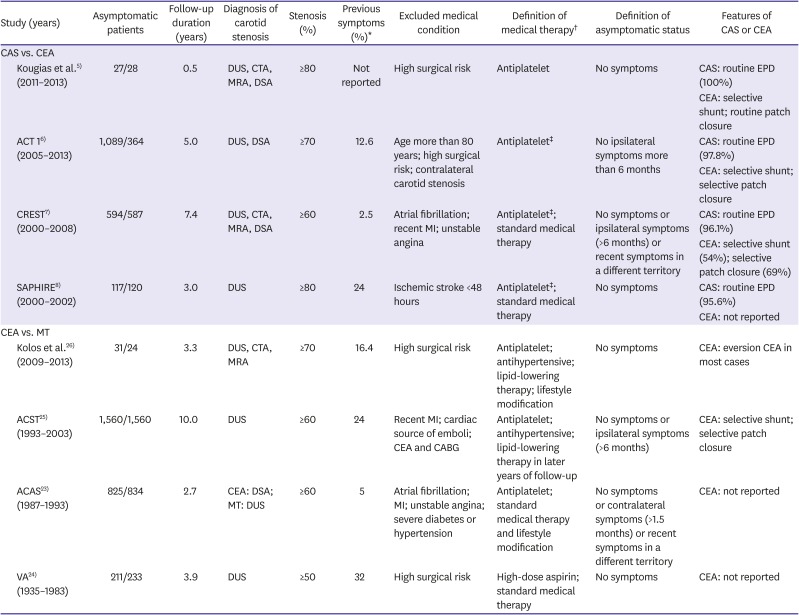
Table 1
Summary characteristics of randomized controlled trials
| Study (years) | Asymptomatic patients | Follow-up duration (years) | Diagnosis of carotid stenosis | Stenosis (%) | Previous symptoms (%)* | Excluded medical condition | Definition of medical therapy† | Definition of asymptomatic status | Features of CAS or CEA | |
|---|---|---|---|---|---|---|---|---|---|---|
| CAS vs. CEA | ||||||||||
| Kougias et al.5) (2011–2013) | 27/28 | 0.5 | DUS, CTA, MRA, DSA | ≥80 | Not reported | High surgical risk | Antiplatelet | No symptoms | CAS: routine EPD (100%) | |
| CEA: selective shunt; routine patch closure | ||||||||||
| ACT 16) (2005–2013) | 1,089/364 | 5.0 | DUS, DSA | ≥70 | 12.6 | Age more than 80 years; high surgical risk; contralateral carotid stenosis | Antiplatelet‡ | No ipsilateral symptoms more than 6 months | CAS: routine EPD (97.8%) | |
| CEA: selective shunt; selective patch closure | ||||||||||
| CREST7) (2000–2008) | 594/587 | 7.4 | DUS, CTA, MRA, DSA | ≥60 | 2.5 | Atrial fibrillation; recent MI; unstable angina | Antiplatelet‡; standard medical therapy | No symptoms or ipsilateral symptoms (>6 months) or recent symptoms in a different territory | CAS: routine EPD (96.1%) | |
| CEA: selective shunt (54%); selective patch closure (69%) | ||||||||||
| SAPHIRE8) (2000–2002) | 117/120 | 3.0 | DUS | ≥80 | 24 | Ischemic stroke <48 hours | Antiplatelet‡; standard medical therapy | No symptoms | CAS: routine EPD (95.6%) | |
| CEA: not reported | ||||||||||
| CEA vs. MT | ||||||||||
| Kolos et al.26) (2009–2013) | 31/24 | 3.3 | DUS, CTA, MRA | ≥70 | 16.4 | High surgical risk | Antiplatelet; antihypertensive; lipid-lowering therapy; lifestyle modification | No symptoms | CEA: eversion CEA in most cases | |
| ACST25) (1993–2003) | 1,560/1,560 | 10.0 | DUS | ≥60 | 24 | Recent MI; cardiac source of emboli; CEA and CABG | Antiplatelet; antihypertensive; lipid-lowering therapy in later years of follow-up | No symptoms or ipsilateral symptoms (>6 months) | CEA: selective shunt; selective patch closure | |
| ACAS23) (1987–1993) | 825/834 | 2.7 | CEA: DSA; MT: DUS | ≥60 | 5 | Atrial fibrillation; MI; unstable angina; severe diabetes or hypertension | Antiplatelet; standard medical therapy and lifestyle modification | No symptoms or contralateral symptoms (>1.5 months) or recent symptoms in a different territory | CEA: not reported | |
| VA24) (1935–1983) | 211/233 | 3.9 | DUS | ≥50 | 32 | High surgical risk | High-dose aspirin; standard medical therapy | No symptoms | CEA: not reported | |
ACAS = Asymptomatic Carotid Atherosclerosis Study; ACST = Asymptomatic Carotid Surgery Trial; ACT 1 = Asymptomatic Carotid Trial; CABG = coronary artery bypass grafting; CAS = carotid artery stenting; CEA = carotid endarterectomy; CREST = Carotid Revascularization Endarterectomy Versus Stenting Trial; CTA = computed tomography angiography; DSA = digital subtraction angiography; DUS = duplex ultrasonography; EPD = embolic protection device; MI = myocardial infarction; MRA = magnetic resonance angiography; MT = medical treatment; SAPPHIRE = Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy; VA = Veterans Affairs.
*Can include any 1 or more of the following: symptoms related to contralateral carotid or other vascular territory or endarterectomy in the contralateral carotid artery; †The definition of standard medical therapy was not provided by trials; ‡CAS received dual-antiplatelet and CEA received single-antiplatelet treatment.
CAS versus CEA
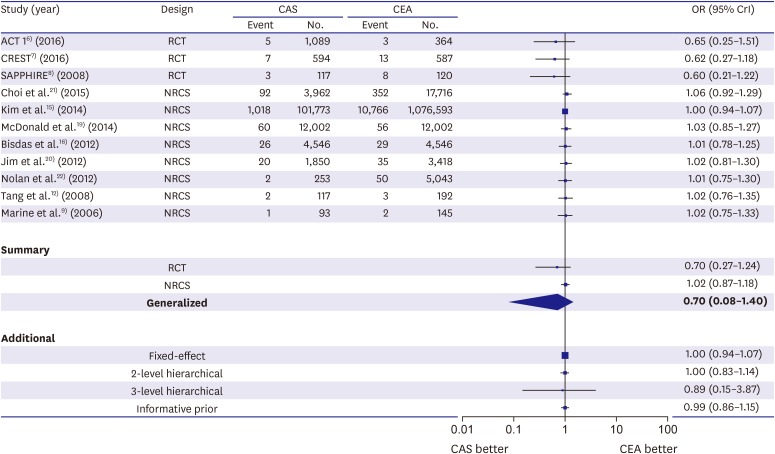
Generalized estimates showed that CAS tended to have a higher risk of periprocedural stroke than CEA (Figure 2). This tendency was consistently observed across RCTs and NRCSs (β, −0.01; 95% CrI, −0.83–0.79). Figure 3 shows a trend of increased risk for periprocedural myocardial infarction with CEA. However, significant heterogeneity was observed between RCTs and NRCSs (β, 0.75; 95% CrI, 0.10–1.45). The observed tendency seemed to mainly come from RCTs whereas ORs maintained around 1 across NRCSs with relatively narrow 95% CrIs. For the composite outcome (composite of death, myocardial infarction, or any stroke during periprocedural period, or ipsilateral stroke thereafter) and ipsilateral stroke, there has been no NRCS reporting on them. Therefore, synthesis of evidence was carried out with the RCTs. Estimates from fixed-effect and 2-level hierarchical models were reported. The risks for the composite outcome and ipsilateral stroke were also insignificantly different between CAS and CEA (Supplementary Figures 1 and 2).
Figure 2
The risk of any periprocedural stroke with stenting versus endarterectomy. Data are expressed on a logarithmic scale. The size of central markers reflects the weight of each study.
ACT 1 = Asymptomatic Carotid Trial; CAS = carotid artery stenting; CEA = carotid endarterectomy; CREST = Carotid Revascularization Endarterectomy versus Stenting Trial; CrI = credible interval; NRCS = nonrandomized comparative study; OR = odds ratio; RCT = randomized controlled trial; SAPPHIRE = Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy.
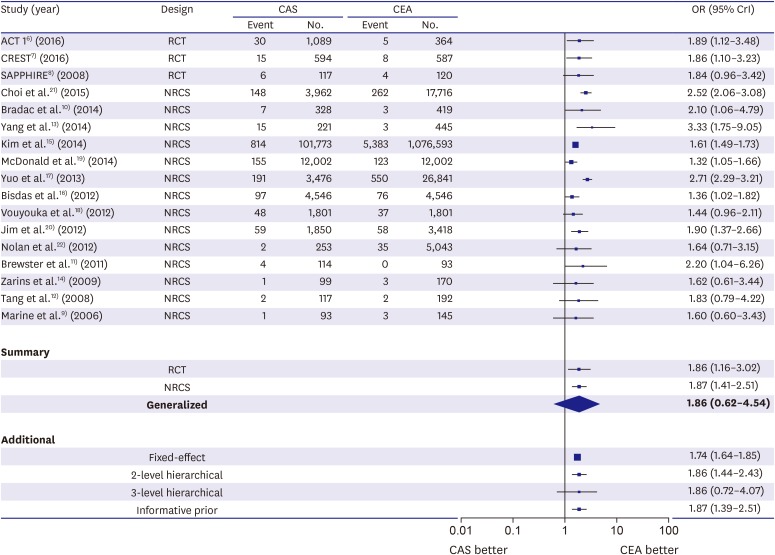
Figure 3
The risk of periprocedural myocardial infarction with stenting versus endarterectomy. Data are expressed on a logarithmic scale. The size of central markers reflects the weight of each study.
ACT 1 = Asymptomatic Carotid Trial; CAS = carotid artery stenting; CEA = carotid endarterectomy; CREST = Carotid Revascularization Endarterectomy versus Stenting Trial; CrI = credible interval; NRCS = nonrandomized comparative study; OR = odds ratio; RCT = randomized controlled trial; SAPPHIRE = Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy.
CAS versus MT
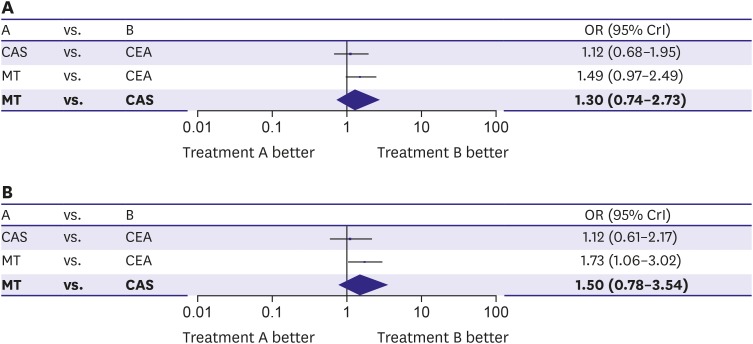
We performed an indirect analysis using a Bayesian network meta-analysis (Supplementary Figure 3). For studies comparing CEA and MT where the composite outcome (composite of death, myocardial infarction, or any stroke during periprocedural period, or ipsilateral stroke thereafter) was not reported, the composite of death, any stroke during periprocedural period, or ipsilateral stroke was used in network meta-analysis models as a substitute. Each trial's results for the composite outcome and ipsilateral stroke are summarized in Table 2 and Supplementary Table 5, respectively. OR for MT versus CAS showed the risk of the composite outcome was higher with MT than with CAS. This tendency did not reach statistical significance (Figure 4). Results for long-term ipsilateral stroke were similar to those for the composite outcome.
Table 2
Combined evidence table for combined safety and efficacy outcome*
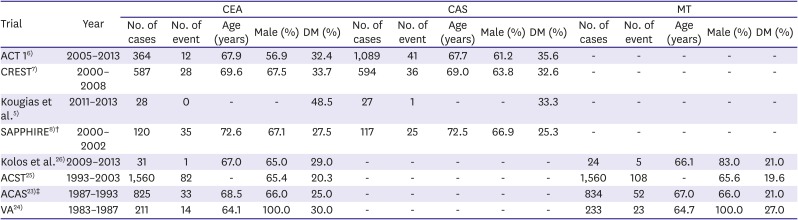
| Trial | Year | CEA | CAS | MT | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of cases | No. of event | Age (years) | Male (%) | DM (%) | No. of cases | No. of event | Age (years) | Male (%) | DM (%) | No. of cases | No. of event | Age (years) | Male (%) | DM (%) | ||
| ACT 16) | 2005–2013 | 364 | 12 | 67.9 | 56.9 | 32.4 | 1,089 | 41 | 67.7 | 61.2 | 35.6 | - | - | - | - | - |
| CREST7) | 2000–2008 | 587 | 28 | 69.6 | 67.5 | 33.7 | 594 | 36 | 69.0 | 63.8 | 32.6 | - | - | - | - | - |
| Kougias et al.5) | 2011–2013 | 28 | 0 | - | - | 48.5 | 27 | 1 | - | - | 33.3 | - | - | - | - | - |
| SAPPHIRE8)† | 2000–2002 | 120 | 35 | 72.6 | 67.1 | 27.5 | 117 | 25 | 72.5 | 66.9 | 25.3 | - | - | - | - | - |
| Kolos et al.26) | 2009–2013 | 31 | 1 | 67.0 | 65.0 | 29.0 | - | - | - | - | - | 24 | 5 | 66.1 | 83.0 | 21.0 |
| ACST25) | 1993–2003 | 1,560 | 82 | - | 65.4 | 20.3 | - | - | - | - | - | 1,560 | 108 | - | 65.6 | 19.6 |
| ACAS23)‡ | 1987–1993 | 825 | 33 | 68.5 | 66.0 | 25.0 | - | - | - | - | - | 834 | 52 | 67.0 | 66.0 | 21.0 |
| VA24) | 1983–1987 | 211 | 14 | 64.1 | 100.0 | 30.0 | - | - | - | - | - | 233 | 23 | 64.7 | 100.0 | 27.0 |
ACAS = Asymptomatic Carotid Atherosclerosis Study; ACST = Asymptomatic Carotid Surgery Trial; ACT 1 = Asymptomatic Carotid Trial; CAS = carotid artery stenting; CEA = carotid endarterectomy; CREST = Carotid Revascularization Endarterectomy Versus Stenting Trial; DM = diabetes mellitus; MT = medical treatment; SAPPHIRE = Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy; VA = Veterans Affairs.
*Composite outcome of periprocedural death, stroke, myocardial infarction, or nonperiprocedural ipsilateral stroke; †Because data on asymptomatic carotid stenosis were not reported separately, those for the mixed population (patients with symptomatic and asymptomatic carotid stenosis) were presented; ‡Age was estimated from the frequency distribution table.
Figure 4
Stenting versus medical treatment for asymptomatic carotid stenosis. Data are expressed on a logarithmic scale. (A) The composite of death, stroke, or myocardial infarction during periprocedural period and ipsilateral stroke during long-term follow-up. (B) The risk for any periprocedural stroke plus nonperiprocedural ipsilateral stroke. The size of central markers reflects the weight of each study.
CAS = carotid artery stenting; CEA = carotid endarterectomy; CrI = credible interval; MT = medical treatment; OR = odds ratio.
Study-level characteristics
To investigate whether CEA alone was the common factor affecting outcomes in comparisons of CEA vs. CAS and CEA vs. MT, we identified possible confounders (proportion of male subjects, average age of participants, proportion of diabetic subjects, and year of first randomization) that might differ across treatment arms and affect outcomes (Table 2 and Supplementary Table 5). In terms of age, CEA participants used as comparators against CAS patients were similar to CEA participants compared against MT patients. Except for the Veterans Affairs trial which enrolled only male patients, proportions of male patients were similar between the two CEA participants groups (CEA participants used as comparators against CAS versus those against MT). The proportion of diabetic patients was higher in the comparison of CEA participants vs. CAS patients than that in the comparison of CEA participants vs. MT patients. Most CEA participants used in the comparison with MT patients underwent CEA in the 1980s and the 1990s whereas those used in comparison with CAS patients underwent CEA in the 2000s and 2010s. To simulate the progress of modern MT, we additionally performed network meta-analyses, with the event rates of MT groups in CEA-versus-MT trials reduced by 15%, 30%, 45%, and 60%. The reductions were based on recent studies that reported 60%–70% decline in annual stroke rates in medically treated asymptomatic carotid stenoses from 1995 to 2010.2)27) Results for the composite outcome and ipsilateral stroke are shown in Supplementary Figures 4 and 5, respectively. For both outcomes, only 30% to 45% reduction of event rates in MT groups had ORs around 1.
DISCUSSION
In this study comparing safety and efficacy between CAS and CEA, we performed Bayesian cross-design analysis including data from 4 RCTs and 14 NRCSs. The risk for periprocedural stroke tended to increase with CAS compared to CEA. Unlike a periprocedural stroke, the estimates for periprocedural myocardial infarction were heterogeneous across RCTs and NRCSs. Despite a trend of increased risk with CEA in RCTs, the risk for periprocedural myocardial infarction was similar in NRCSs. Regarding the comparison between CAS and MT, indirect comparisons using a Bayesian network meta-analysis indicated a tendency to lower risk for the composite outcome with CAS than that with MT. However, the tendency did not reach statistical significance.
In general, our analyses produced similar results to those reported by other trials and meta-analyses.6)7)8)28) However, for a few outcomes, considerable heterogeneities were observed between estimates from RCTs and NRCSs. This seemed to weaken the validity of combining evidence from disparate sources.
Concerning periprocedural stroke, CAS tended to have a higher risk than CEA in our analyses. Recently, Sardar et al.28) have performed a meta-analysis using 5 trials that enrolled 6,526 patients with symptomatic and asymptomatic carotid stenosis. They reported a significantly higher risk for periprocedural stroke with CAS than that with CEA. Their analysis stratified by symptomatic status revealed similar results for asymptomatic carotid stenosis.
Despite such drawback of CAS, it has been advocated against CEA, with which the risk for periprocedural myocardial infarction has been reported to be higher than CAS by previous studies.6)7)8)28) For example, Sardar et al.28) have revealed in their recent meta-analysis that CEA is associated with a higher risk for periprocedural myocardial infarction regardless of the symptomatic status of carotid stenosis. Similarly, in our analyses, the risk for periprocedural myocardial infarction tended to be higher with CEA. Interestingly, significant heterogeneity was observed between estimates from RCTs and NRCSs. Estimates from the former favored CAS, while ORs from the latter consistently maintained around 1 with fairly narrow credible intervals. There are three possible explanations for such similar risks observed in NRCSs. First, in real-world practice, routine evaluations for perioperative cardiovascular risk might allow high risk patients to receive CAS or MT, rather than CEA. Second, coronary stenosis found by such evaluation might be revascularized preoperatively which protect high risk patients from undergoing myocardial infarction caused by hemodynamic instability during CEA. Finally, the NRCSs were not designed originally to assess the risk of periprocedural myocardial infarction. Therefore, asymptomatic elevation of cardiac enzymes after CEA might not have been captured. These hypotheses suggest that in situations where preoperative evaluation and management are normally working, concerns about periprocedural myocardial infarction associated with CEA would not matter. This supports recent ESC guideline that puts CEA ahead of CAS for patients with average surgical risk.2) Furthermore, the risk for periprocedural myocardial infarction and stroke should be discussed via multidisciplinary approaches before revascularization.
In the absence of an RCT comparing CAS and MT, we indirectly compared them via Bayesian network meta-analyses. In terms of the composite outcome, a trend of lower risk with CAS was observed. However, several features were observed that might have weakened the validity of our network analyses. First, most CEA-versus-MT studies took place in the 1980s and 1990s before several improvements in MT such as dual antiplatelet therapy, statins, and angiotensin-converting enzyme inhibitors took place, whereas CAS-versus-CEA studies were conducted after these improvements. Although this might be suspected of a violation of the exchangeability assumption of indirect comparison, its effects on our results were not expected to be remarkable, given the similar occurrence of clinical events between the two CEA groups of CEA-versus-MT and CEA-versus-CAS studies. Second, our indirect comparison actually indicated the beneficial effect of CAS over outdated medical therapy. In fact, the risk of stroke has been reducing in patients who receive medical therapy alone. Raman et al.27) have analyzed 26 studies on asymptomatic carotid stenosis, each of which included a MT group. In their study, meta-regression analyses showed that the incidence rate of ipsilateral stroke was statistically significantly lower in studies that completed recruitment between 2000 and 2010 than in those that completed recruitment earlier (1.13% vs. 2.38% per year, respectively; p<0.001). Given advances in modern medical therapy, maybe the probability of beneficial effect accompanied by CAS have been overestimated. This was supported by our simulations to determine how event rate reduction in the MT groups might affect the results of indirect comparisons between CAS and MT. Therefore, it seems reasonable that the recent ESC guideline restricts indications for CAS to patients whose clinical and/or imaging characteristics suggest an increased risk of late ipsilateral stroke. Ongoing European Carotid Surgery Trial 2 (ECST-2) and CREST-2 will shed light on these issues.
The present study has several limitations. First, our results are subjected to limitations inherent to meta-analysis involving pooling of data from different trials with different study protocols, definitions of clinical outcomes, and baseline characteristics of patients. As a result, there was wide variability in the risk profile and lesion complexity of included patients, the use of the embolic protection device, types of stents used, and proficiency of participating operators. The disparate nature of these two study designs (RCT vs. NRCS) and limited number of the studies that reported data on characteristics of patients and procedures precluded subgroup and meta-regression analyses to address these issues. Second, in our network meta-analysis, the number of trials included was relatively small. It has been recognized that indirect comparisons performed in a network meta-analysis may give misleading results when trial numbers are small.29) Finally, in simulations for event rate reduction in the MT groups of CEA-versus-MT trials, we arbitrarily assumed that clinical outcomes of CEA would not improve by advances in medical therapy. However, remarkable differences were not observed in occurrence of the composite outcome or ipsilateral stroke between the two CEA groups of CEA-versus-MT and CEA-versus-CAS studies, which might have limitedly supported that assumption.
In conclusion, CAS tended to have higher risk of periprocedural stroke than CEA. Although the risk for periprocedural myocardial infarction tended to be higher with CEA than that with CAS in RCTs, similar risks between them in NRCSs indicated that the risk was not much different under usual preoperative evaluation and management for cardiovascular risk. In indirect comparison between CAS and MT, the tendency to have higher risk for the composite outcome with MT might have been overestimated considering difference in study age between CEA-versus-MT and CEA-versus-CAS trials.
 XML Download
XML Download