

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Percutaneous coronary intervention (PCI) using a metallic stent is the conventional treatment of coronary artery disease. Compared with the bare-metal stents (BMSs), the first-generation drug-eluting stent (DES) has remarkably decreased the rates of restenosis and target lesion revascularization (TLR).1)2) Nevertheless, there was a concern about late stent thrombosis (ST) which is associated with the delayed endothelialization and hypersensitivity reaction from the polymer used in the first-generation DES.3)4) To overcome this limitation, the newer-generation DES with a biocompatible durable polymer or those with a biodegradable polymer have been developed and quickly adopted. Recent trials demonstrated the enhanced safety and efficacy of these newer-generation DES compared with first-generation DES.5)6)7)
Recently, Genoss DES™ stent (Genoss Company Limited, Suwon, Korea) comprising a cobalt-chromium (CoCr) platform with a thin strut thickness, sirolimus, and an abluminal biodegradable polymer has been developed. In a previous first-in-man trial, the Genoss DES™ stent exhibited similar angiographic and clinical outcomes at a 9-month follow-up, compared with Promus Element (Boston Scientific, Natick, MA, USA).8) However, the sample size of this trial was small to offer solid evidence of the safety and efficacy of this Genoss DES™ stent. Hence, we are conducting the prospective registry of the Genoss DES™ stent to elucidate the clinical outcomes in terms of the efficacy and safety of the Genoss DES™ in an unselected cohort of subjects from a real-world population.
We report the results of this registry among subjects eligible for a 12-month follow-up to offer the substantial evidence of the safety and efficacy of this stent owing to the rapid and extensive dissemination of the Genoss DES™ stent.
METHODS
Genoss DES™ prospective registry
The Genoss DES™ prospective registry (ClinicalTrials.gov Identifier: NCT03045913) is an ongoing, prospective, single-arm, observational, multicenter trial that aims to enroll 2,000 subjects and follow them clinically for 12 months from 16 centers in South Korea since November 2016. In this registry, subjects aged ≥19 years presented with stable angina or acute coronary syndrome who were successfully implanted the Genoss DES™ for at least one significant coronary stenosis within 1 month were eligible. The primary exclusion criteria were limited to intolerance to medication, allergy to stent component, or planned surgery within the 12 months after the index PCI, cardiogenic shock during the index PCI, life expectancy <12 months, and the implantation of a combination of different types of DES or BMS.
In this analysis, we enrolled subjects eligible for 12-month follow-up and the last patient was enrolled on May 31, 2018. All subjects fulfilled all eligibility criteria and provided written informed consent for participation. This study protocol (CR216010) was approved by the local Institutional Review Board.
Genoss DES™ stent
The Genoss DES™ is a sirolimus-eluting stent with abluminal biodegradable polymer and CoCr platform.8) The L605 CoCr alloy platform features open-cell 2 links with a uniform architecture that provides high-level flexibility, optimized radial force, and enhanced conformability but is resistant to shortening. In addition, the thin strut thickness (70 µm for a stent with a diameter of 2.25–2.50 mm and 78 µm for a stent with a diameter of 2.75–5.00 mm) is adopted. The stent is designed to release nearly 70% of its initial drug payload (1.15 µg/mm2) within the first 30 days following implantation. To attain the desired drug release profile and minimize the amount of polymer, a 3-µm ultrathin coating is applied to only the abluminal side of the stent; this biodegradable coating comprises a proprietary blend of poly(lactic-co-glycolic acid) and poly(L-lactic acid), which are almost completely degradable within 9 months.
Study procedure
PCI was conducted using standard interventional techniques. Based on the current guideline, a dose and duration of dual antiplatelet therapy with aspirin plus clopidogrel (alterable with prasugrel or ticagrelor) were encouraged to be followed.9)10) No restrictions exist regarding the number, severity, or location of lesions, or the number of stents used. The use of additional pharmacological agents, thrombectomy device, and intravascular ultrasound (IVUS), optical coherence tomography, or pressure wire were at the operators' discretion. During multivessel PCI or bifurcation PCI, plain old balloon angioplasty (POBA) with or without drug-coated balloon (DCB) in conjunction with the Genoss DES™ implantation was permitted. Procedural success was defined as achievement of <30% residual diameter stenosis of the target lesion assessed by visual inspection. A clinical follow-up visit was scheduled at 1, 6, and 12 months after the index procedure. All subjects were followed either by office visit or telephone contact as necessary.
Study endpoints
The primary endpoint was a device-oriented composite outcome (DOCO) comprising cardiac death, target vessel-related myocardial infarction (MI), and clinically indicated TLR at 12-month clinical follow-up. The secondary endpoints were patient-oriented composite outcome (POCO) comprising any death, any MI, and any revascularization; each component of DOCO and POCO; and Academic Research Consortium-defined ST at 12-month clinical follow-up. All definitions of endpoints are provided elsewhere.11)
Statistical analysis
Continuous variables were expressed as mean±standard deviation (SD) or median (interquartile range) and categorical variables were expressed as number (percentages). We evaluated the event-free survival based on the unadjusted Kaplan-Meier method. The clinical follow-up was censored at the date of the last follow-up or at 365 days, whichever came first. Of note, the data for subjects lost to follow-up were censored at the time of the last contact. In a subgroup analysis, we categorized subjects according to age, sex, acute MI, hypertension, diabetes, chronic kidney disease, smoking, prior MI, PCI at any in-stent restenosis (ISR) lesion, PCI at any chronic total occlusion (CTO) lesion, PCI at any bifurcation lesion, use of IVUS, use of DCB or plain balloon, use of any stent diameter ≤2.5 mm, and use of any stent length >30 mm. We compared each subgroup with the log-rank test without statistical adjustment because the event rate was sporadic and thus the Cox proportional hazard model could not be used. All statistical analyses in this study were performed using SPSS (version 20; IBM Corp., NY, USA).
RESULTS
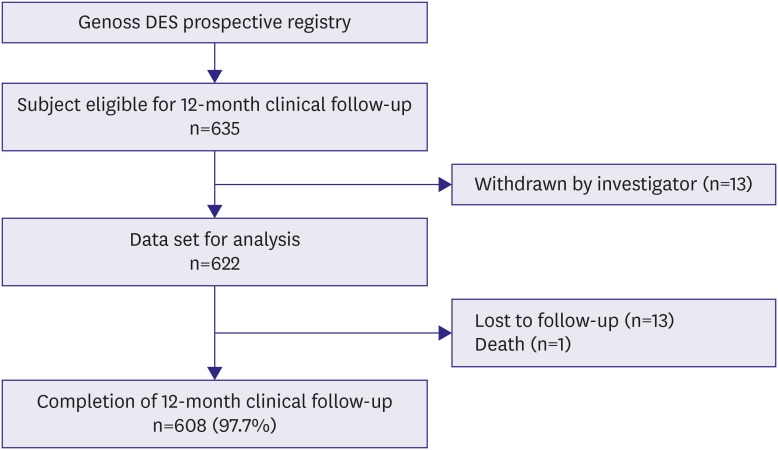
In this ongoing registry, 1,125 subjects were enrolled at the timing of analysis. Of these, 635 subjects were eligible for 12-month follow-up. After excluding 13 subjects for several reasons as shown in Figure 1, 622 subjects were finally analyzed for clinical outcomes.
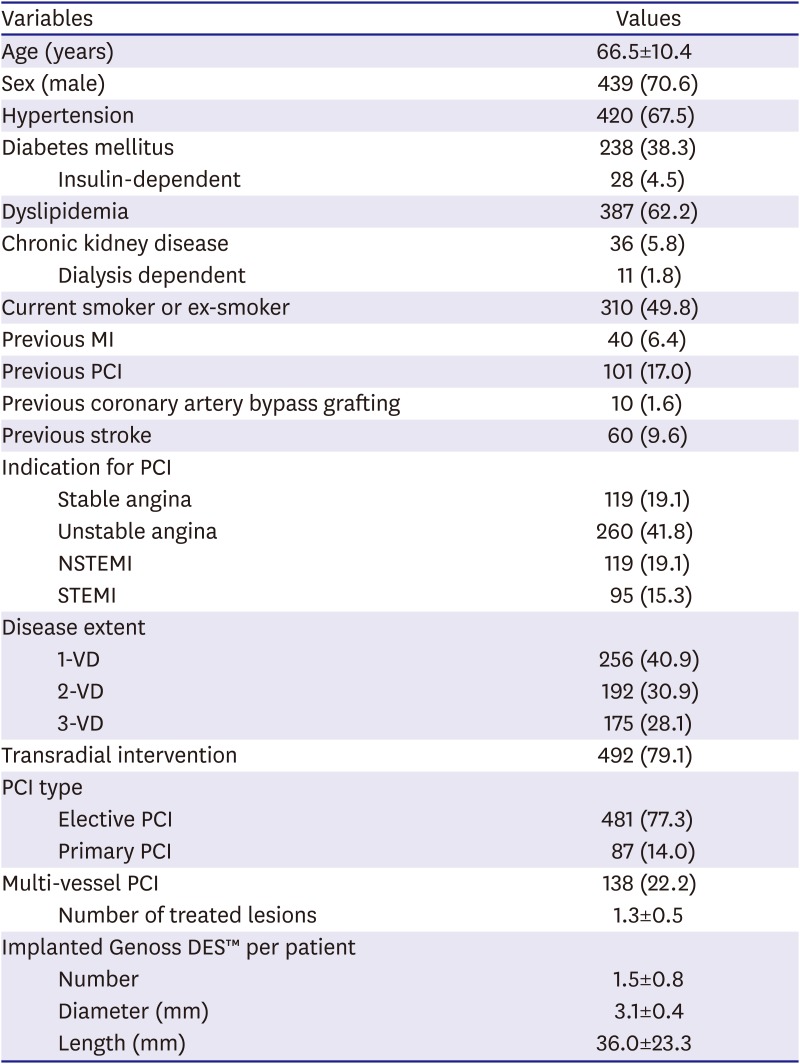
The baseline, angiographic, and procedural characteristics of the study population are summarized in Table 1. The mean age of subjects was 66.5±10.4 years, 70.6% were males, 67.5% had hypertension, and 38.3% had diabetes. A history of MI and PCI was observed in 6.4% and 17.0% of subjects, respectively. The indication for PCI was ACS in 76.2% of subjects. The multivessel disease was observed in 59.0% of subjects, but the multivessel PCI was performed in 22.2% of subjects. As 15.3% of subjects were presented with ST-segment elevation MI, 14.0% underwent primary PCI. The implanted stent number, diameter, and length per patient were 1.5±0.8, 3.1±0.4 mm, and 36.0±23.3 mm, respectively.
Table 1
Baseline, angiographic, and procedural characteristics of patients enrolled in the Genoss DES™ registry (n=622)
The angiographic and procedural characteristics of lesions are summarized in Table 2. Overall, 753 lesions were treated in 622 subjects, and ISR lesions were included in 5.0% of lesions. We observed thrombotic lesions in 10.6% of lesions, and thrombectomy was performed in 5.7% of lesions. In addition, American College of Cardiology/American Heart Association-type B2/C lesions were 72.4%. Most frequently treated lesions were located at the left anterior descending coronary artery (48.6%). As POBA or DCB was allowed, 1.6% of lesions were treated with Genoss DES™ plus POBA or DCB. In addition, PCI for CTO and PCI for bifurcation lesions were performed in 4.2% and 10.9% of lesions, respectively. The procedural success rate was 97.9% because of 16 lesions of suboptimal PCI.
Table 2
Angiographic and procedural characteristics of lesions implanted with Genoss DES™ (n=753)
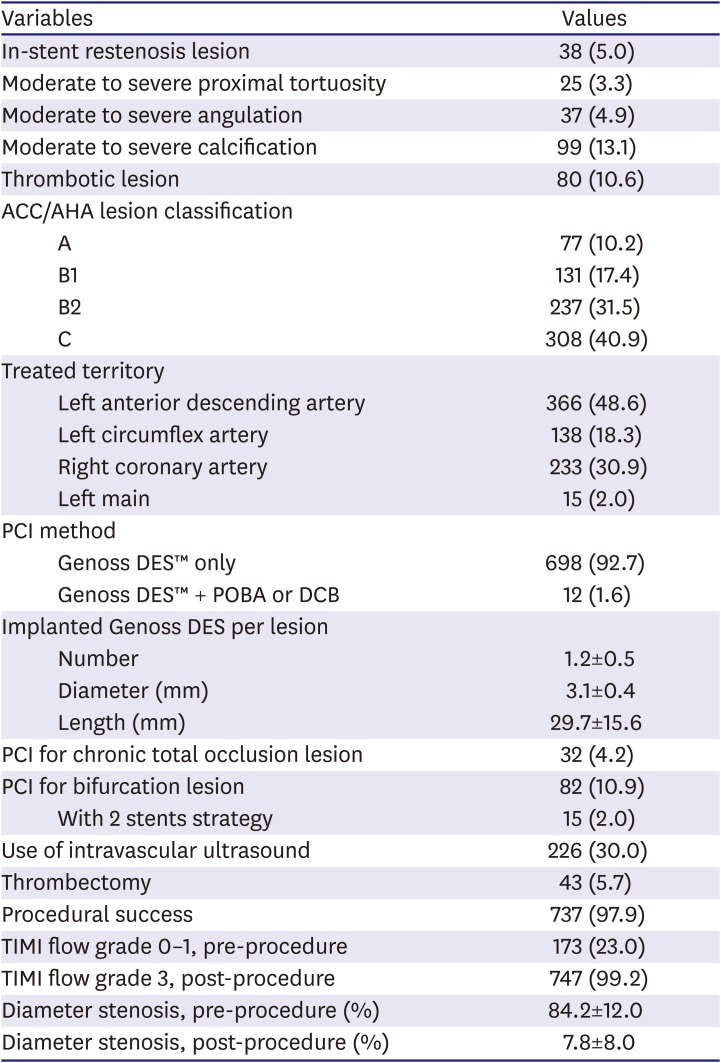
Values are mean±standard deviation or number (%).
ACC = American College of Cardiology; AHA = American Heart Association; DCB = drug-coated balloon; DES = drug-eluting stent; PCI = percutaneous coronary intervention; POBA = plain old balloon angioplasty; TIMI = thrombolysis in myocardial infarction.
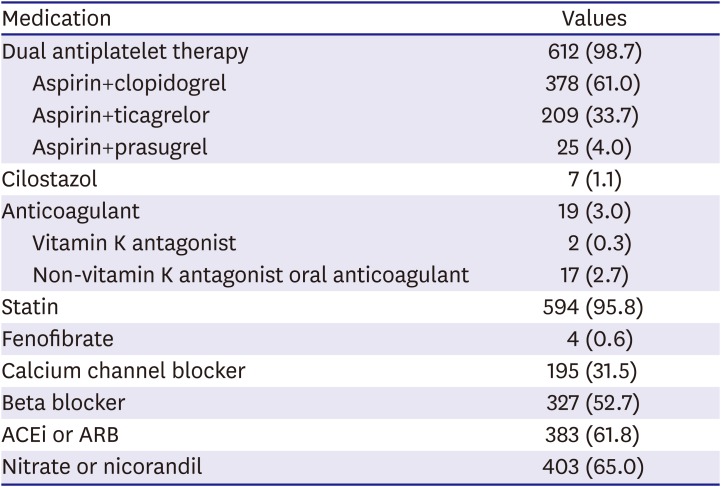
Medications among 620 survivors at discharge are presented in Table 3. The use of dual antiplatelet was 98.7%. Most commonly used dual antiplatelet therapy was aspirin plus clopidogrel (61.0%) and followed by aspirin plus ticagrelor (33.7%). The use of statin was 95.8%.
Table 3
Discharge medications among survivors at discharge (n=620)
The clinical outcomes at 12-month follow-up are presented in Table 4. Details of patients experienced with adverse clinical events are summarized in a Supplementary Table 1. The 12-month follow-up could be attained in 97.7% of subjects and the median follow-up duration was 365 days (interquartile range: 343–365 days). The primary endpoint, DOCO, occurred only in 4 (0.6%) subjects and it was mainly derived by TLR (0.5%). POCO occurred in 24 (3.9%) of subjects at the 12-month follow-up. Definite and probable ST was observed in 4 (0.6%) subjects. Figure 2 illustrates the Kaplan-Meier survival curves of DOCO, POCO, TLR, and definite and probable ST. Table 5 presents the subgroup analysis for DOCO. Results were not different between the subgroups except any use of stent diameter ≤2.5 mm and any use of stent length >30 mm. However, the statistical differences in TLR rate were not observed when the per-lesion analyses were performed (3/669 [0.4%] in the group of stent diameter >2.5 mm vs. 0/84 [0%] in the group of stent diameter ≤2.5 mm, p>0.999; 1/487 [0.2%] in the group of stent length <30 mm vs. 2/266 [0.8%] in the group of stent length ≥30 mm, p=0.556).
Table 4
Clinical outcomes at 12-month follow-up (n=622)
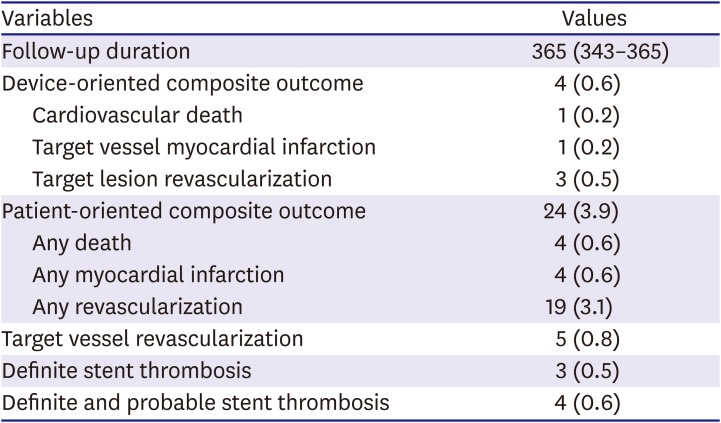
Figure 2
The Kaplan-Meier survival curves. Event rate was estimated based on the unadjusted Kaplan-Meier method. (A) DOCO; (B) POCO; (C) TLR; and (D) definite and probable stent thrombosis.
DOCO = device-oriented composite outcome; POCO = patient-oriented composite outcome; TLR = target lesion revascularization.
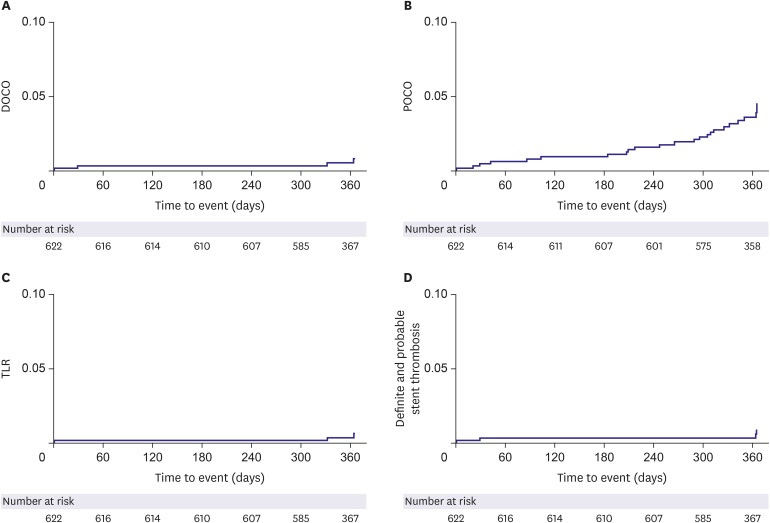
Table 5
Subgroup analysis for device-oriented composite outcome
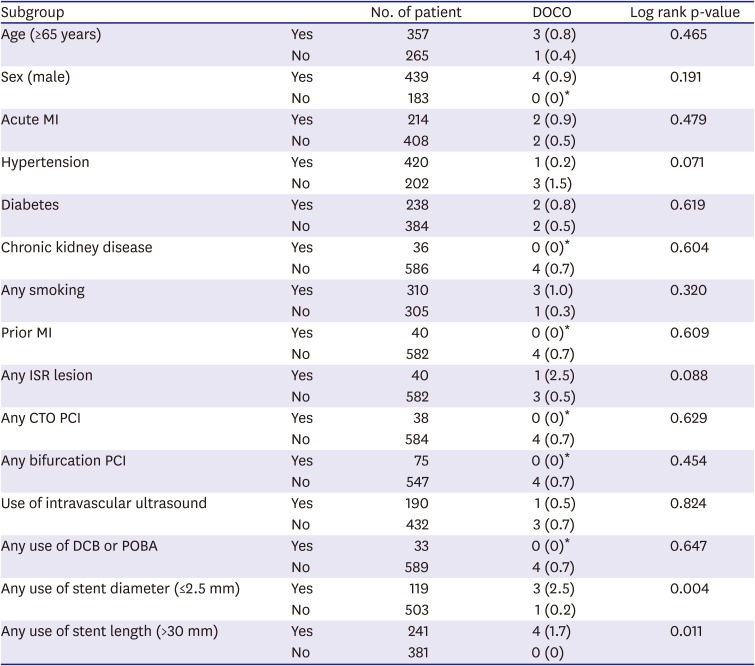
DOCO values are number (%). Event-free survival rate was estimated based on the unadjusted Kaplan-Meier method.
CTO = chronic total occlusion; DCB = drug-coated balloon; DOCO = device-oriented composite outcome; ISR = in-stent restenosis; MI = myocardial infarction; PCI = percutaneous coronary intervention; POBA = plain old balloon angioplasty.
*No statistics are computed because all cases are censored.
DISCUSSION
This analysis of the Genoss DES™ prospective registry presents the safety and efficacy of the Genoss DES™ stent in real-world practice. The primary findings are as follows: 1) the treatment of coronary artery disease with the Genoss DES™ stent resulted in very low clinical event rates, with DOCO of 0.6% and definite and probable ST of 0.6% at 12-month follow-up; 2) the rate of cardiovascular death, target vessel MI, and clinically driven TLR was 0.2%, 0.2%, and was 0.5% at 12-month follow-up, respectively; and 3) low clinical events were consistent across all subgroups any use of stent diameter ≤2.5 mm and any use of stent length >30 mm.
In a previous first-in-man trial, in which 38 and 39 subjects were randomly assigned to the Genoss DES™ group and the Promus Element group, respectively, only 1 patient of each group underwent TLR, and there were no cardiovascular death, target vessel MI, and ST at the 9-month follow-up.8) Despite the fact that the Genoss DES™ prospective registry included subjects at high risk for the clinical event such as acute MI, CTO, ISR lesion, left main disease, and long lesion, the clinical event rate was minimal. This study validated the results of the first-in-man trial in real-world practice.
The favorable result mentioned above could be associated with the strut thickness. In a meta-analysis of 10 randomized control trials in which the newer-generation ultrathin strut DES (defined as strut thickness <70 µm) were compared with second-generation thicker struts, newer-generation ultrathin strut DES correlated with a 16% decline in the target lesion failure (relative risk [RR], 0.84; 95% confidence interval [CI], 0.72–0.99) driven by less MI (RR, 0.80; 95% CI, 0.65–0.99) compared with thicker strut second-generation DES.12) In addition, ultrathin strut DES correlated with qualitatively lower rates of any ST (RR, 0.72; 95% CI, 0.51–1.01). Compared with the Orsiro stent (Biotronik, Bülach, Switzerland), which is the one of newer-generation ultrathin strut DES, the strut thickness of the Genoss DES™ stent (70 µm) is marginally higher than that of the Orsiro stent (60 µm).13) However, the polymer thickness Genoss DES™ stent (3.0 µm) is thinner than that of the Orsiro stent (7.4 µm). In addition, the polymer coating of the Orsiro stent is circumferential, while that of the Genoss DES™ stent is abluminal. Accordingly, the total thickness (strut thickness+polymer) is thinner in the Genoss DES™ stent and, thus, more favorable results could be anticipated.
In the Genoss DES™ stent, sirolimus was loaded at a concentration of 1.15 µg/mm2, and the polymer was designed to release approximately 70% of the total drug amount within 30 days of implantation and are entirely resorbable within 9 months. These properties of the polymer and drug-eluting kinetics could decrease the neointimal hyperplasia, with the likelihood of ST because of polymer hypersensitivity. In the first-in-man trial, in-stent late lumen loss was only 0.11±0.25 mm after 9 months of the Genoss DES™ stent implantation, with no ST.8)
In this trial, 3 cases of TLR were observed and 2 of them were related to the definite ST. However, 1 case of ST was acute definite ST and it was revealed that this ST was associated with the edge dissection. Except for this case, only 2 cases of TLR were observed around 1 year after the index procedure.
Despite the all-comer nature of the study population, the event rates of this trial were low, which may raise the question of under-reporting of clinical events. There may be several reasons. First, we did not include the procedure-related MI and thus, the rate of clinical outcomes, especially in MI, could be lower than previous studies. Second, more potent P2Y12 antagonists such as ticagrelor and prasugrel were used in this trial, which may be related to the lower ischemic event and might contribute to the lower clinical outcomes.14)15) Third, about 80% of PCI was performed using transradial access which is associated with a lower risk of adverse clinical events especially in patients with ST-segment elevation MI.16) Fourth, an ethnic or genetic protective factor might be related to lower clinical event. East Asians paradox, in which East Asian patients have a similar or even a lower rate of ischemic events after PCI compared with white patients, may contribute to our results.17)18) Finally, considering the lower rate of severely calcified (23% vs. 5%) and bifurcated lesions (35% vs. 11%) in our study compared with a BIOSCIENCE trial,19) it could be possible that the operator would select the familiar stent rather than the Genoss DES™ stent whenever the operator faced the challenging lesions because of lack of enough efficacy and safety evidence of the new device.
In a recently published BIOSCIENCE trial, all-comer subjects (n=3,514) treated with ultrathin-strut biodegradable polymer Orsiro sirolimus-eluting stents or Synergy everolimus-eluting stents (Boston Scientific, Marlborough, MA, USA) versus thin-strut durable polymer Resolute Integrity zotarolimus-eluting stents (Medtronic, Santa Rosa, CA, USA) were compared.19) The rate of DOCO at 12-month follow-up was 4.0% in Orsiro stent, 4.2% in the Synergy stent, and 4.5% in Resolute stent in this trial. However, the DOCO was mainly driven by periprocedural MI, and the rate of TLR was only 1.6% in Orsiro stent, 1.5% in the Synergy stent, and 1.5% in the Resolute stent. Considering the rate of TLR, the results of our trial were in line with those of BIOSCIENCE trial.
This study has several limitations. First, this study is represented by the nonrandomized design and lacks comparator for a direct comparison. Second, this registry enrolled subjects from Korean centers only and, thus, results should be validated in different ethnics and regions. Third, this interim analysis was not prespecified. Although this prospective registry is ongoing, this study aims to offer substantial evidence of the safety and efficacy of the Genoss DES™ stent owing to the rapid and extensive dissemination of the Genoss DES™ stent. Because of a relatively small number of subjects and thus, the final results could be different. Finally, we could not adjust any confounders and provide predictors of the primary endpoint during subgroup analysis using the multivariate analysis, such as multiple logistic regression or Cox regression, because of the extremely low event rate and the small number of samples.
In conclusion, this trial demonstrates that the Genoss DES™ stent in real-world practice is safe and effective for treating subjects with coronary artery disease.
 XML Download
XML Download