

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Stroke prevention is the principal management priority in patients with atrial fibrillation (AF) given its association with a 5-fold increase in stroke risk, and that 1 in 5 cases of stroke can be attributed to this arrhythmia.1)2) The non-vitamin K antagonist oral anticoagulants (NOACs) have been shown at least as effective and safe as warfarin with a lower incidence of intracranial hemorrhage.3) The preferred use of NOACs is recommended in guidelines,4)5)6) albeit with gradual uptake of their prescription in routine practice.7) Recent studies have suggested that the availability of NOACs may improve rates of use of overall oral anticoagulation (OAC) rate in patients with AF.8)9) Previously Lee et al.10) reported the differences in the utilization of antithrombotic therapy based on geographical regions and income levels among Korean population. However, social inequalities of OAC in different medical systems after introduction of NOAC have not been evaluated in large-scale nationwide studies. Accordingly, we analyzed data from the Korean National Health Insurance Service (NHIS) data to assess how the availability of NOACs has affected overall rate and social inequalities of OAC usage. We describe the temporal trends in OAC use, including both warfarin and NOACs, and patient factors associated with prescription of warfarin, NOACs. Second, we assessed the extent of practice-level variation in OAC and NOAC usage according to different medical systems.
METHODS
This nationwide study is based on the national health claims database established by the NHIS of Korea.11)12) The NHIS is the single insurer managed by the Korean government, and the vast majority (97.1%) of the Korean population are mandatory subscribers, with the remaining 3% of the population being medical aid subjects. Since 2006, information of Medical Aid beneficiaries has been incorporated into a single NHIS database. Therefore, the data extracted from the NHIS claims database are indeed based on the entire Korean population, in a nationwide cohort. The NHIS claims database includes diagnoses, procedures, biochemical test results, prescription records, and demographic information. The database is open to researchers, whose study protocols are approved by the official review committee. We confirmed diagnoses by using the International Classification of Disease, Tenth Revision (ICD-10) codes. This study was approved by the Institutional Review Board of Yonsei University Health System (4-2016-0179). The International Review Board waived the requirement to obtain informed consent, and this study was conducted in accordance with the tenets of the Declaration of Helsinki.
Study population
In the Korean NHIS data, 1,034,099 patients with prevalent AF who were aged ≥18 years were identified during the period from January 1, 2002 to December 31, 2016. The following were exclusion criteria: 1) those who ever received treatment with OAC before AF diagnosis (n=115,997), to exclude patients who had taken OAC for reasons other than AF such as venous thrombosis and 2) those with any of following conditions such as mitral valve stenosis and prosthetic valve replacement (ICD-10 codes I050, I052, I342; n=29,562). Finally 888,540 patients were included in the analysis (Figure 1). The annual prevalence of AF was calculated by dividing the number of AF patients of each year with exception for AF patients who died in previous year by the number of total Korean residents of that year. The annual incidence of AF was the number of incident cases of AF divided by the number of person-years at risk among all Korean residents of that year who had never been diagnosed as AF. AF was identified with ICD-10 codes; I48 (AF and atrial flutter), I48.0 (AF), and I48.1 (atrial flutter). To ensure accuracy, diagnosis was established based on one inpatient or 2 outpatient records of ICD-10 codes in the database.13)14) To evaluate the accuracy of our definition of AF, we conducted a validation study in 2 hospitals with 628 randomly chosen patients with the ICD-10 code I48. The patients were ascertained to have AF if it was documented by electrocardiogram examinations. The positive predictive value was found to be 94.1%.

Baseline comorbidities and endpoints
Baseline comorbidities were identified from medical claims according to ICD-10 codes and prescription codes and all comorbidities were established based on one inpatient or 2 outpatient records of ICD-10 codes in the database, similar to previous studies based with NHIS cohort. Hypertension, diabetes mellitus, heart failure, peripheral arterial disease, a history of myocardial infarction, a history of stroke and/or transient ischemic attack (TIA), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and end-stage renal disease (ESRD) were all assessed. The CHA2DS2-VASc score (2 points each for age 75 years or older and previous TIA or stroke; and 1 point each for heart failure, hypertension, age 65 years or older, diabetes mellitus, vascular disease, and female sex) for each subject was estimated at the end of the screening period, and every year during the follow-up period. Definitions of comorbidities are presented in Supplementary Table 1. Economic status was categorized into 3 groups based on the total amount of national health insurance premiums paid by the insured individual in each year, which is proportional to the individual's income: low, intermediate, and high economic status.15)
The primary outcome was prescription of any OAC (warfarin, dabigatran, rivaroxaban, or apixaban). The rates of OAC use calculated by the continued use of OAC in each period with considering prescription date and amount. The difference in the rates of OAC use according to the different criteria was presented in Supplementary Figure 1. Secondary outcomes included prescription of any NOAC (dabigatran, rivaroxaban, or apixaban) and of the individual NOACs. Prescription data were obtained from NHIS outpatient encounter documentation. For patients with multiple encounters, the last encounter was used in the analysis.
Statistical analysis
In Korea, NOACs were partially and fully reimbursed by the national insurance system in January 2013 and July 2015, respectively. We then examined temporal trends in the rates of use of any OAC, warfarin, and NOACs. For each month during the study period, we determined the proportion of patients who received therapeutic OAC with warfarin, dabigatran, rivaroxaban, or apixaban. If patients had >1 visit per month, the last study visit from each patient in each month was used for the analysis. A Cochrane-Armitage test for trend analysis was then performed to evaluate for changes in rates of use of any OAC over time.
We then examined the association between patient-level variables and the use of OAC. We used separate hierarchical, multivariable logistic regression models to better understand the individual contributions of patient factors to OAC use. Patient-level variables for this model included demographics (age and sex), comorbid conditions and risk factors (hypertension, diabetes mellitus, dyslipidemia, heart failure, previous stroke or TIA, vascular diseases, CKD or ESRD, COPD, and the use of antiplatelet agents). We also calculated the total CHA2DS2-VASc score.
To assess the effect of practice level on OAC use, we divided medical institutions by scale as follows: tertiary referral hospital, secondary care hospital, primary care hospital, and other healthcare facilities such as public health center, nursing hospital, etc. Then we compared the changes in the utilization rates of any OAC, warfarin, and NOACs within one year after the AF diagnosis of each practice level by year, among patients with more than 2 points of CHA2DS2-VASc score. Statistical analyses were performed using SPSS version 23.0 statistical package (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics and temporal trends in overall OAC use
Patients were categorized by reimbursement, and their characteristics were compared (Table 1). In general, patients after full reimbursement of NOAC had higher rates of comorbidities, and higher CHA2DS2-VASc scores.
Table 1
Baseline characteristics
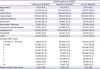
Values are mean±standard deviation or number (%).
NOAC = non-vitamin K antagonist oral anticoagulant; TIA = transient ischemic attack; CKD = chronic kidney disease; ESRD = end-stage renal disease; COPD = chronic obstructive pulmonary disease; CHA2DS2-VASc = congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, prior stroke, transient ischemic attack, or thromboembolism, vascular disease, age 65–74 years, sex category (female).
![]()
In all population, overall OAC use increased from 13.2% to 23.4% (p for trend <0.001), and NOAC use increased from 0% to 14.6% (p for trend <0.001). OAC use increased from 13.2% to 18.0% before the full reimbursement of NOAC (p for trend <0.001), and further increased to 23.4% after the full reimbursement of NOAC (p for trend <0.001). Compared with pre-reimbursement (0.48%), the annual increase of OAC was significantly higher after partial (1.16%, p<0.001) and full reimbursement of OAC (3.72%, p<0.001) (Figure 2A). In the subgroup of AF patients with CHA2DS2-VASc score ≥2, the rate of use of overall OAC increased from 14.6% in 2010 to 28.1% in 2016 (p for trend <0.001). The annual increase of OAC was 0.60%, 1.38% and 4.85% at before, after partial and full reimbursement of NOACs. The annual increase of OAC significantly increased after partial (p<0.001) and full reimbursement of OAC (p<0.001) (Figure 2B).
 | Figure 2Temporal trends in overall oral anticoagulation prescription in total atrial fibrillation population (A) and patients with CHA2DS2-VASc score ≥2 (B).NOAC = non-vitamin K antagonist oral anticoagulant; CHA2DS2-VASc = congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, prior stroke, transient ischemic attack, or thromboembolism, vascular disease, age 65–74 years, sex category (female).
|
Warfarin use also increased from 13.0% to 15.6% before the full reimbursement of NOAC (p for trend <0.001), but finally decreased to 8.8% during the study period. Any NOAC use increased from 0% to 14.6% (p for trend <0.001).
Reimbursement of NOAC and OAC use
In all patients, patient characteristics associated with OAC use are shown in Figure 3A. In the multivariate models, patient factors associated with lower rates of use of OAC included CKD or ESRD, COPD, vascular disease, use of antiplatelet agents, female sex and diabetes mellitus. Patient factors associated with higher rates of use of OAC included heart failure, hypertension, previous stroke or TIA, dyslipidemia and age older than 65 years. Partial (adjusted odds ratio [OR], 1.58; 95% confidence interval [CI], 1.56–1.60) and full reimbursement of NOAC (adjusted OR, 2.04; 95% CI, 2.00–2.09) were independently associated with higher OAC use in total population.
 | Figure 3Adjusted patient factors associated with overall OAC use within 1 year from AF diagnosis in total AF population (A) and patients with CHA2DS2-VASc score ≥2 (B).CKD = chronic kidney disease; ESRD = end-stage renal disease; COPD = chronic obstructive pulmonary disease; TIA = transient ischemic attack; NOAC = non-vitamin K antagonist oral anticoagulant; OAC = oral anticoagulant; CI = confidence interval; AF = atrial fibrillation; CHA2DS2-VASc = congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, prior stroke, transient ischemic attack, or thromboembolism, vascular disease, age 65–74 years, sex category (female).
|
In patients with CHA2DS2-VASc score ≥2, patient factors associated with lower rates of use of any OAC included use of antiplatelet agents, CKD or ESRD, COPD, vascular disease, female sex, diabetes mellitus and hypertension (Figure 3B). Higher rates of use of any OAC included heart failure, previous stroke or TIA, dyslipidemia and age older than 65 years. Partial (adjusted OR, 1.60; 95% CI, 1.58–1.63) and full reimbursement of NOACs (adjusted OR, 2.10; 95% CI, 2.04–2.15) was independently associated with higher OAC use.
Practice level variation and social inequalities in OAC use
Significant practice-level variation was evident in the use of OAC. Figure 4 illustrates the temporal trends in OAC initiation within 1 year after AF diagnosis according to the practice level. The use of any OAC in eligible patients ranged from 4.9% to 22.8% in 2010, and from 7.2% to 44.0% in 2016 according to the practice level. The difference of OAC usage between tertiary referral hospital and nursing or public health centers increased from 17.9% in 2010 to 36.8% in 2016 (Figure 4A). The rate of OAC use significantly increased from 22.8% to 44.0% in tertiary referral hospitals (p<0.001), from 17.9% to 36.7% in secondary care hospitals (p<0.001), and from 11.0% to 25.2% at primary care hospitals (p<0.001). OAC use remained without improvement in other healthcare facilities such as nursing hospital or public health center.
 | Figure 4Practice level variation in total OAC (A), warfarin (B), and NOAC (C) use for AF patients with CHA2DS2-VASc score ≥2.OAC = oral anticoagulant; NOAC = non-vitamin K antagonist oral anticoagulant; AF = atrial fibrillation; CHA2DS2-VASc = congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, prior stroke, transient ischemic attack, or thromboembolism, vascular disease, age 65–74 years, sex category (female).
*Others include nursing hospital, public health centers, etc.
|
Warfarin use increased from 2010 to 2014, before the full reimbursement of NOAC, but finally decreased in 2016 compared to 2010 at all practice-levels (Figure 4B). In 2016, the rate of NOAC use ranged from 5.5% to 37.2% according to the practice level (Figure 4C). NOAC use increased dramatically from 0% to 37.2% at the tertiary referral hospital, 31.8% at secondary care hospitals, 20.9% at primary care hospitals, and 5.5% at other healthcare facilities (for all, p for trend <0.001). Practice level variation in the prescription rate of individual NOAC among AF patients along time elapse is presented in Supplementary Figure 2.
In addition, we further analyzed OAC usage according to the patients' economic status (Figure 5). The increase in NOAC use was slightly higher in patients with high economic status compared to the others, but the use of NOAC showed an even trend across the 3 economic status groups, without significant difference.

DISCUSSION
In Korean AF patients, we found that the rate of overall OAC use increased from 15.6% to 26.9% following the introduction and reimbursement of NOACs. Second, the full reimbursement of NOACs was strongly associated with higher OAC use, which suggests that the change in insurance policy for NOACs might have contributed to improved overall OAC prescription rates among eligible AF patients. Finally, significant practice variation was present in OAC and NOAC usage among different medical systems. This finding shows increased social inequalities of OAC usage after the introduction of NOAC despite full reimbursement of NOAC.
The study illustrates how incentivisation of NOAC use by offering reimbursement improves OAC uptake. Underuse of OAC in patients with AF is not uncommon,16)17) and is known to be associated with increased risk of stroke and systemic thromboembolism.18)19) Before 2014, <20% of the incident and prevalent AF patients in Korea were prescribed OAC.16)17) Similar to other recent reports,20)21) we found that overall rates of OAC for AF increased following the introduction of NOACs. Given that randomized clinical trials have demonstrated relative safety and efficacy of the NOACs compared with warfarin, especially evident amongst Asian patients,22) and these alternatives to warfarin have likely contributed to increased rate of OAC utilization. Our results suggested the early trends in adoption of NOACs persist, although they appear to be used more as de novo therapy for those who were not previously anticoagulated, rather than as a transition from warfarin.
In Korea, NOACs were partially reimbursed by the national insurance system in January 2013. In period of partial reimbursement, insurance benefits were applied only to patients whose international normalized ratio level did not achieve therapeutic level even with considerable dose adjustment. Overall OAC prescription rates increased during this period, but only to a limited extent. The increase in OAC prescription at this time might be mainly due to expansion of consensus on the prescription of anticoagulants rather than the application of insurance benefit itself.
Despite the considerable increase in overall OAC use observed in the present study, several challenges remain regarding the effective and sufficient use of OAC for eligible AF patients. Although overall OAC use increased during our study period, a large number of patients with AF without a documented contraindication to OAC were still not receiving OAC.
Significant practice-level variation existed for overall OAC and NOAC use. Although NOAC was dramatically increased in tertiary referral hospitals, its increase was minimal in primary care, nursing and public health centers. This result is in consistent with a data from the ORBIT-AF (Outcomes Registry for Better Quality of Care in the Treatment of AF) registry, which demonstrated higher rates of OAC utilization among patients with AF seen by electrophysiology specialists compared with general cardiologists and primary care providers.23) Electrophysiology specialists in referral medical institutions are seemingly more aggressive in terms of stroke prevention, and they adhere better to treatment guidelines compared with general practitioner providers. This might represent a higher likelihood of patients without contraindication to OAC being referred to electrophysiology practices and an enhanced attention to the need for OAC by electrophysiology providers.21) One additional possibility for the difference in OAC utilization is likely to be due to differences in age distribution between the practice levels. The mean age of patients in nursing hospital or public health center was significantly higher than those in tertiary referral hospital (78.9±11.3 vs. 64.0±15.4 years, p<0.001). Previous studies demonstrated that extreme old age is associated with underutilization of OAC among AF patients.24)25) The present study also shows that which practice level is associated with NOAC use over time. Further research is needed to reduce variation and improve use of OAC for patients at risk of stroke associated with AF, by streamlining primary and secondary patient management pathways.26) This is of particular importance, given that a significant portion of patients at high risk of stroke related to AF receive no OAC therapy.27)
Our study results should be interpreted in the context of the following limitations, given the natures of the nationwide registry database we used. First, baseline AF diagnosis and other comorbidities were dependent on the ICD-10 codes; therefore, the diagnosis of AF could be inaccurate although the method for the diagnosis has been validated in previous studies, and our internal validation found a high correlation with actual AF diagnosis. Second, although our analysis provided some insights regarding the effect of national insurance system on the change of treatment pattern we observed, we could not account for all variables that might have influenced the use of OAC. Third, the present nationwide study only enrolled the entire Korean population, whether the results can be extrapolated to other populations remains uncertain. Fourth, the present study investigated only up to 1.5 years after the expansion of NOAC insurance coverage in Korea. Future studies of data after 2017 will further expand the issues discussed in this study. Despite these limitations, this study had a large sample size and included a long follow-up period of the entire Korean adult population.
The introduction of NOACs in routine practice for stroke prevention in AF was associated with improved rates of overall OAC use for AF. However, significant practice-level variations in OAC and NOAC use remained producing social inequalities of OAC despite full reimbursement.
 XML Download
XML Download