

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Up to 50% of patients presenting with ST elevation myocardial infarction (STEMI) have multi-vessel coronary artery disease (MVCD), and these patients had significant stenosis in at least one of the non-infarct-related arteries (IRAs).1)2)3) There is no argument about performing primary percutaneous coronary intervention (P-PCI) of culprit lesion, however, it is still controversial about whether and when to do non-IRA lesions percutaneous coronary intervention (PCI).4)5)6)7) There are 2 PCI options to archive complete multi-vessel revascularization. First, multi-vessel single-staged PCI (SS PCI) which defined as non-IRA lesions PCI at the same time of IRA lesion P-PCI; Second, multi-vessel multi-staged PCI (MS PCI) which defined as staged non-IRA lesions PCI after IRA lesion P-PCI during the initial hospitalization. The 2015 American Heart Association (AHA)/American College of Cardiology Foundation (ACCF) guidelines for the management of STEMI recommended that PCI of a non-IRA may be considered in patients with STEMI and MVCD who are hemodynamically stable, either at the time of P-PCI or as a planned staged procedure (Class IIb, B–R)8); the current 2017 European Society of Cardiology (ESC) guidelines for the management of STEMI recommended that PCI of a non-IRA should be considered before hospital discharge (Class IIa, A) and non-IRA PCI during the index procedure should be considered in patients with cardiogenic shock (Class IIa, C).9) Although several studies revealed that multi-vessel MS PCI is associated with better outcomes than multi-vessel SS PCI,10)11)12) large data on the difference in clinical outcomes are needed. Thus, we conducted our study to compare the clinical outcomes between 2 different complete multi-vessel revascularization strategies in Korean patients with STEMI and MVCD: multi-vessel SS PCI versus multi-vessel MS PCI during the index hospitalization.
METHODS
Study design and population
This study population was derived from the Korea Acute Myocardial Infarction Registry (KAMIR)-National Institutes of Health (NIH). The KAMIR-NIH is a prospective, multicenter, on-line based observational cohort study that is still ongoing. Patients with a diagnosis of acute myocardial infarction (AMI) from 20 centers (tertiary university PCI-capable hospitals) have been enrolled from November 2011 to December 2015 in Korea and followed up through 2018. The KAMIR-NIH contains all consecutive characteristics and clinical outcomes of Korean patients with AMI and it reflects prognostic and surveillance index. Data were collected by the attending physician and trained clinical research coordinators through a web-based case report form in the clinical data management system.13)
We consecutively selected patients with STEMI and MVCD from the database. The STEMI was diagnosed by a new ST elevation in ≥ 2 contiguous leads, measuring >0.2 mV in leads V1–3 or 0.1 mV in all other leads on 12-lead electrocardiography (ECG) with a concomitant increase in troponin-I or -T. The MVCD was confirmed by coronary angiography that significant stenosis (presence of diameter stenosis ≥50%, visually estimated) is seen in at least 1 of the non-IRA. Among them, patients with culprit only P-PCI, multi-vessel partial revascularization, facilitated PCI or delayed PCI, defined as a PCI was not performed within 12 hours of ischemic symptom presentation, fibrinolytic therapy, conservative treatment or missing data were excluded. These patients were divided into 2 groups according to the timing of non-IRA lesions PCI. Per clinician decision, non-IRA lesions PCI was performed at the same time of IRA lesion P-PCI (multi-vessel SS PCI, namely) or the separated staged procedure (multi-vessel MS PCI, namely). This study was approved by the Institutional Review Board of our medical institution and all patients provided written informed consent for participation in the registry.
Study outcomes
The primary outcome was all-cause mortality and the secondary outcomes were major adverse cardiovascular event (MACE) and cardiac death during the one year of follow-up.
MACE was defined as a composite of all-cause death, recurrent myocardial infarction (MI), repeat revascularization components (target lesion or target vessel revascularization), stent thrombosis and stroke. Each of the components was assessed individually. The cardiac death was defined as death from arrhythmia, pump failure or mechanical complications including free wall rupture and ventricular septal rupture. Recurrent MI was defined as an elevation in troponin-I or T level above the 99th percentile of the upper normal limit with concomitant ischemic symptom or change of ECG. Target lesion revascularization (TLR) was defined as any repeat PCI to treat luminal stenosis occurred within 5-mm edge of the stent in the target lesion. Target vessel revascularization (TVR) was defined as repeat PCI outside the 5mm edge of the stent or any segment of the target vessel. Stent thrombosis was defined as definite development of a stent-related thrombotic event, according to the Academic Research Consortium (ARC) classification.14)
Statistical analysis
The analysis was performed to examine the differences in adverse outcomes between the 2 groups. Continuous variables were presented as mean±standard deviation (SD) or median with interquartile range (IQR), and they were compared using the independent t-test or Mann-Whitney U test between the 2 groups. Categorical variables were expressed as raw numbers and percentages. Categorical variables were compared with Pearson's χ2 or Fisher's exact tests between the 2 groups. To minimalize the effect of selection bias in the comparison between SS PCI and MS PCI group, the propensity score was estimated using a multivariable logistic regression model that contained 12 covariates which were significantly different between 2 groups. Model discrimination was measured by the c-statistic and calibration was assessed by the Hosmer-Lemeshow goodness-of-fit test (c-statistic: 0.559, Hosmer-Lemeshow: p=0.126). Matching was performed using a greedy matching protocol (1:1 matching without replacement) with a caliper width of 0.03. We matched 162 patients of SS PCI to 162 patients of MS PCI. We estimated standardized differences for covariates shown significant differences in Tables 1 and 2 before and after propensity score matching to assess the balance of the covariates between the matched SS PCI group and MS PCI group. After matching, none of the covariates showed a standardized differences exceeding 5%, suggesting that all of the measured covariates were well balanced between the matched groups (Supplementary Figure 1).
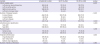
Table 1
Baseline characteristics of the patients

Values are number (%) for categorical values; median and interquartile rage (25–75%) or means±standard deviation for continuous variables.
ACE = angiotensin-converting enzyme; ARB = angiotensin II receptor blocker; CK-MB = creatine kinase-myocardial band; LVEF = left ventricular ejection fraction, MS PCI = multi-staged percutaneous coronary intervention; NT-proBNP = N-terminal prohormone of brain natriuretic peptide; SS PCI = single-staged percutaneous coronary intervention.
*Body mass index is defined as the weight divided by the square of the body height.
Table 2
Procedural characteristics
Values are number (%) for categorical values; means±standard deviation for continuous variables.
ACC = American College of Cardiology; AHA = American Heart Association; IRA = infarct-related artery; MS PCI = multi-staged percutaneous coronary intervention; SS PCI = single-staged percutaneous coronary intervention; TIMI = thrombolysis in myocardial infarction.
The cumulative events analyses were performed using time-to-event data by the Kaplan-Meier method, survival curves were compared using the log-rank test. Patients were censored at the time of event occurred or at last follow-up. Kaplan-Meier curves were plotted for the time to the occurrence of the clinical outcomes. A multivariate Cox proportional hazards regression was used to estimate hazard ratios (HRs), with 95% confidence interval (CI) in both all patients and patients of matched groups. Only variables with a p value <0.05 in the univariate analysis were used to evaluate HRs as estimates for each endpoint.
All statistical tests were considered 2-tailed and statistical significant was defined as a p value of <0.05. The Statistical Package for Social Sciences software, version 24.0 (SPSS, Inc., Chicago, IL, USA) was used for analyses.
RESULTS
Patients and characteristics
Between November 2011 and December 2015, total of 6,300 patients with a diagnosis of STEMI were enrolled and screened. Of 3,037 STEMI patients with MVCD, 2,418 patients were excluded for various reasons. Finally, 606 patients who were performed complete multi-vessel revascularization during the initial hospitalization were enrolled in our study. Among them, 254 patients (42%) underwent SS PCI and 352 patients (58%) underwent MS PCI (Figure 1).
Figure 1
Study population flow chart. The patients with STEMI and multi-vessel coronary artery disease were enrolled. Among them, 254 patients underwent multi-vessel SS PCI and 352 patients underwent multi-vessel MS PCI.
KAMlR–NIH = Korea Acute Myocardial Infarction Registry-National Institute of Health; MS PCI = multi-staged percutaneous coronary intervention; P-PCI = primary percutaneous coronary intervention; PCI = percutaneous coronary intervention; STEMI = ST elevation myocardial infarction; SS PCI = single-staged percutaneous coronary intervention.

Baseline characteristics are shown in Tables 1 and 2. Two treatment groups were similar in age, sex, the prevalence of diabetes, hypertension and dyslipidemia as cardiovascular risk factors (Table 1). The patients in the SS PCI group had lower ejection fractions and showed more incidence of severe left ventricular systolic dysfunction than those in MS PCI group. Regarding the in-hospital medication, beta-blocker, statin, and glycoprotein IIb/IIIa inhibitor were prescribed more frequently in the MS PCI group. Procedure-related characteristics are shown in Table 2. The number of diseased vessel and locations of culprit lesion on coronary angiography were significantly different between the 2 groups. A total number of the implanted stent at culprit lesion was similar between the two groups. After propensity-score matching, there were no significant differences in baseline clinical, procedural characteristics between the 2 groups, except in-hospital duration. (Supplementary Tables 1 and 2)
Clinical outcomes
We summarized the clinical outcomes during the 1-year of follow-up (Table 3). The mean follow-up duration was 347 days. In multivariate Cox regression analysis, the patients treated with MS PCI strategy had a significantly lower rate of all-cause mortality (adjusted HR, 0.42; 95% CI, 0.19–0.92; p=0.030) compared with those treated with SS PCI strategy at 1-year. While the overall clinical adverse event rates such as MACE, cardiac death, and its components were lower in the MS PCI group, there were no statistical differences between the two groups after adjustment. In the propensity-matched patients, MS PCI group showed a significantly lower rate of MACE than SS PCI (adjusted HR, 0.48; 95% CI, 0.24–0.96; p=0.038; Table 4).
Table 3
One-year clinical outcomes in all patients

Values are number (%) for categorical values.
MACE = major adverse cardiovascular event; MS PCI = multi-staged percutaneous coronary intervention; SS PCI = single-staged percutaneous coronary intervention; TLR = target lesion revascularization; TVR = target vessel revascularization.
*HR are for the multi-vessel MS PCI groups compared with multi-vessel SS PCI group; †Adjusted Cox hazard regression analysis included age, sex, medications (statin, glycoprotein IIb/IIIa inhibitor), initial heart rate, left ventricular ejection fraction, pre TIMI flow (0–1 vs. 2–3), Initial Killip class (I–II vs. III–IV), infarct related vessel (IRA), treatment of IRA lesion, number of vessel disease; ‡Subjects who had an adverse events in initial 30 days were excluded in 30 days to 1-year outcomes data. Cox hazard regression analysis also included same variables used in 30 days outcomes and 1-year outcomes; §MACE defined as a composite of all-cause death, myocardial infarction, stroke, TVR, TLR, stent thrombosis.
Table 4
One-year clinical outcomes in propensity score matched patients

Values are number (%) for categorical values.
MACE = major adverse cardiovascular event; MS PCI = multi-staged percutaneous coronary intervention; SS PCI = single-staged percutaneous coronary intervention; TLR = target lesion revascularization; TVR = target vessel revascularization.
*HR are for the multi-vessel MS PCI groups compared with multi-vessel SS PCI group; †Adjusted Cox hazard regression analysis included various clinical variables including age, sex, use of statin, left ventricular ejection fraction, Initial Killip class (I-II vs. III-IV), and Target vessel; ‡Subjects who had an adverse events in initial 30 days were excluded in 30 days to 1-year outcomes data. Cox hazard regression analysis also included same variables used in 30 days outcomes and 1-year outcomes.
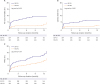
The Kaplan-Meier curves for cumulative event rates of clinical outcomes at 1-year of follow-up were shown according to the revascularization strategy (Figure 2 and Supplementary Figure 2). SS PCI group had a higher rate of all-cause mortality (27% vs. 12%), cardiac death (19% vs. 8%), and MACE (16.9% vs. 10.2%) at 1-year. When we compared the incidence of clinical outcomes divided into early (30 days events) and late stage (30 days to 1 year events) between SS PCI and MS PCI group, all-cause mortality, cardiac death, and MACE of SS PCI were significantly higher within 30 days, but not 30 days to 1 year in the Kaplan-Meier curve analyses. (Table 3 and Supplementary Figure 2).
Figure 2
Event rates of all-cause mortality, cardiac death and MACE for the entire patients at 1-year of follow-up. The Kaplan-Meier curves for cumulative event rates of all-cause mortality (A), cardiac death (B) and MACE (C) were shown according to the type of revascularization. Multi-vessel SS PCI group showed a higher rate of all-cause mortality (27% vs. 12%), cardiac death (19% vs. 8%), and MACE (16.9% vs. 10.2%) at 1-year of follow-up.
MACE = major adverse cardiovascular event; MS PCI = multi-staged percutaneous coronary intervention; SS PCI = single-staged percutaneous coronary intervention.
Subgroups analysis
In the pre-specified subgroup analysis, SS PCI group had an increased risk of adverse outcomes compared to MS PCI group, and the similar trend was shown in all subgroups (Supplementary Tables 3 and 4). As shown in the Figure 3, there were significantly higher rates of all-cause mortality in the subgroup of cardiogenic shock (HR, 4.60; 95% CI, 1.54–13.77; p=0.006), age ≥65 year (HR, 4.00; 95% CI, 1.67–9.58; p=0.002), Killip class III/IV (HR, 7.32; 95% CI, 1.68–31.87; p=0.008) and creatinine clearance ≤60 mL/min/1.73 m2 (HR, 2.81; 95% CI, 1.10–7.18; p=0.031) in the SS PCI group. The Kaplan-Meier curves of the subgroup for all-cause mortality and cardiac death at 1-year were showed in Supplementary Figure 3.
Figure 3
Subgroups analysis for all-cause mortality. The Cox regression analyses revealed that the multi-vessel SS PCI group had a higher rate of all-cause mortality compared to multi-vessel MS PCI group in all subgroups. Especially, high-risk patients such as cardiogenic shock, Killip class III/IV, creatinine clearance ≤60 mL/min/1.73 m2 in the multi-vessel SS PCI group had lower mortality rates in the multi-vessel MS PCI group.
CI = confidence interval; LVEF = left ventricular ejection fraction; HR = hazard ratio; MS PCI = multi-staged percutaneous coronary intervention; SS PCI = single-staged percutaneous coronary intervention.

DISCUSSION
We conducted our study to determine the optimal timing of non-IRA lesions PCI in Korean patients with MVCD and STEMI. The main findings of our study are that MS PCI strategy was superior to reduce 1-year all-cause mortality compared with SS PCI strategy in patients with STEMI and MVCD. Moreover, in patients with cardiogenic shock, age ≥65, Killip class III/IV or creatinine clearance ≤60 mL/min/1.73 m2, the risk of all-cause mortality was significantly decreased in MS PCI group than in SS PCI group. After propensity score matching, MS PCI showed a significantly lower rate of MACE than SS PCI.
It is well known that MVCD in the STEMI patients associated with a higher rate of adverse cardiac outcomes compared with single vessel disease.3)6) Non-IRA strategy of MVCD in the STEMI patients depends on whether or not there is a cardiogenic shock. According to the current ESC practice guidelines, non-IRA lesions PCI at the time of P-PCI was considered in patients with cardiogenic shock.9) Because SS PCI might improve hemodynamic stability, it should be considered during the primary procedure in patients with cardiogenic shock. However, this recommendation is based just on a consensus opinion (the level of evidence C). Also, no randomized clinical trials compared the 2 complete revascularization strategies. Moreover, some data which are not favor of SS PCI in cardiogenic shock patients were not included in current ESC STEMI practice guideline.15)16)17) Recently, several meta-analyses documented that SS PCI did not improve clinical outcomes over culprit lesion only PCI in patients with cardiogenic shock.15)16) Thiele et al.17) also reported random clinical trial that 1-year mortality did not differ significantly between culprit-lesion only PCI group and immediate multi-vessel PCI group in patients with AMI, cardiogenic shock, and MVCD. Their result archived improved clinical outcomes in all-cause mortality or renal replacement therapy in culprit-lesion-only PCI group over immediate multi-vessel PCI group (relative risk, 0.87; 95% CI, 0.76–0.99; p=0.048). Lee et al.18) reported with KAMIR-NIH registry that multi-vessel PCI (complete revascularization) showed more improved all-cause death and reduced non-IRA repeat revascularization than IRA only PCI, but the multi-vessel PCI group included about 40% of patients underwent MS PCI. However, these studies, unlike our study, are not also a comparison of 2 complete revascularization strategies.
In hemodynamically stable patients, recent guidelines recommended that non-IRA lesions routine revascularization should be considered before hospital discharge, but not proposed the optimal timing of revascularization (immediate vs. staged).8)9) This guideline's recommendation was derived from several meta-analyses and random clinical trials.19)20)21)22)23)24) The Complete Versus Culprit-Lesion Only Primary PCI (CvLPRIT) trial showed that in-hospital complete revascularization of significant non-culprit lesions resulted in improved clinical outcomes compared with the treatment of culprit lesion only.23) The Preventive Angioplasty in Acute Myocardial Infarction (PRAMI) trial also demonstrated that complete multi-vessel revascularization during the index procedure showed superior composite primary outcome compared with the culprit artery only P-PCI.24) The Third Danish Study of Optimal Acute Treatment of Patients with ST-Segment Elevation Myocardial Infarction - Primary PCI in Multivessel Disease (DANAMI-3 PRIMULTI) was compared fractional flow reserve (FFR)-guided complete revascularization with infarct-artery-only revascularization. The observed relative risk reduction in favor of complete revascularization was 44% (p=0.004).22) Smits et al.21) compared immediate FFR-guided complete revascularization and IRA only revascularization with ischemia-guided staged PCI. FFR-guided complete revascularization reduced the risk of a composite cardiovascular outcome as compared with IRA only revascularization. Most of these data compared complete revascularization strategies including SS PCI and MS PCI with IRA only revascularization.
Differ from these all reports, our study compared 2 complete revascularization strategies (immediate vs. staged). MS PCI showed improved 1-year clinical outcomes compared with SS PCI and showed clinical benefit in high-risk patients with cardiogenic shock, the elder (≥65 years), high Killip class (III/IV), low creatinine clearance (≤60 mL/min/1.73 m2). These better clinical outcomes in MS PCI group are likely to be explained by the following reasons. First, the enhanced thrombotic and inflammatory environment of STEMI contributes to a higher risk of procedural complications as compared with elective procedures.25)26)27) Factors that increase risk are related to the complexity and duration of the procedure in the case with multi-vessel PCI for STEMI. Second, when performing multi-vessel PCI of the significant non-IRA lesion, the PCI will be performed without objective evidence for the presence of myocardial ischemia. If SS PCI is performed on the lesions that are not accurately assessed the significance of coronary artery stenosis, it would not give a benefit in hemodynamically unstable conditions and high-risk patients.28) FFR-guided PCI could provide a clue of myocardial ischemia.21)22) Third, generally, contrast use increases in SS PCI, which may be less well tolerated in the patient with STEMI, especially radiocontrast nephropathy develops; it could aggravate clinical outcomes.29) Finally, unexpected peri-procedural complications in the non-IRA may be poorly tolerated due to the simultaneous impairment of the culprit and non-IRA lesions.
Selection of the complete revascularization strategy as SS PCI versus MS PCI was based on a physician decision and the reasons why a physician chose that treatment among 2 options were not prospectively collected. During the early period of patient recruitment in this study from 2011 to 2015, there were no strong recommendations for multi-vessel revascularization for STEMI patients with multi-vessel disease. So, decision of the treatment strategy between SS PCI and MS PCI is usually made by medical status of the individual patients and decision of cardiologists with different policies. As revascularization strategies depend on the operator's decision, we could not exclude the possibility that MS PCI group might have a less severe ischemic driven non-IRA lesion. In this study, matching of the 2 strategy groups was balanced with statistical power but cannot overcome the independency of randomization study. That is, we could not collect the reasons for non-IRA revascularization such as spontaneous ischemia or intermediate- or high-risk findings on the predischarge noninvasive test. Further study about FFR-guided revascularization should overcome this problem.
Although our data showed all subgroup shown in Figure 3 favors MS PCI strategy, we suggest that SS PCI strategy could be considered carefully in low-risk patients such as stable hemodynamics, the young (<65 years), low Killip class I/II, and relatively normal creatinine clearance (≥60 mL/min/1.73 m2) shown in Supplementary Table 3.
Our study has several limitations. First, our study is based on a prospective, observational registry, but a small-scale, non-randomized study. Although statistical adjustment including propensity score matching was performed, propensity score-matched patients were too small to evaluate the differences of the outcomes between two groups. This issue could lower the statistic power. A propensity score matching could not replace randomization when exploring clinical data with important clinical implication. Second, although the median hospitalization period of MS PCI group was 6 days, we do not know the exact time between the index procedure and staged PCI. Fourth, KAMIR registry has no angiographic core lab to describe the procedure. We could not find additional procedure time, difficulty of procedure, amount of used contrast, endurance of the patients, and significance of lesion. These limited data of the detailed angiographic findings and exact reason why involved physicians decided to perform SS vs. MS PCI hard to suggest clear-cut criteria to decide the strategy of PCI.
In conclusion, our study revealed that SS PCI was associated with worse clinical outcomes compared with MS PCI. MS PCI for non-IRA could be a better option for patients with STEMI and MVCD, especially high-risk patients. Although MS PCI is better option for all patients with STEMI and MVCD, SS PCI strategy could be considered carefully in low-risk patients such as stable hemodynamics, the young, low Killip class I/II, relatively normal creatinine clearance.
 XML Download
XML Download