

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Elevated blood pressure is a major preventable cause for cardiovascular diseases, including ischemic heart disease, stroke, heart failure, atrial fibrillation, and peripheral arterial disease, and a leading cause of all-cause mortality worldwide.1 Lifestyle modification is important for the prevention and treatment of elevated blood pressure. This includes weight loss,2 increased physical activity,3 and reduced alcohol consumption,4 which can reduce cardiovascular disease risk.
Alcohol is mainly metabolized by alcohol dehydrogenase (ADH) and acetaldehyde dehydrogenase. There are genetic differences in these enzymes in different ethnic groups. The aldehyde dehydrogenase 2 (ALDH2) variant is common in East Asians, and the activity of ALDH2 varies by about 3–5 fold according to rs671,5 a missense ALDH2 mutation. Mutations in ALDH2 are closely related to the avoidance of alcohol drinking. Inactive ALDH2 causes alcohol flush reactions such as erythema, nausea, and rapid heart rate as a result of aldehyde accumulation after alcohol consumption.67 Active ALDH2 carriers who do not develop alcohol flushing tend to be drinkers with a greater amount of alcohol intake.8910
Many previous studies have evaluated the association between the ALDH2 rs671 polymorphism and blood pressure.9111213141516 In some studies,911121416 the ALDH2 genotype was considered as an instrumental variable of alcohol consumption. However, the ALDH2 genotype modifies the effects of alcohol via aldehyde accumulation. Therefore, it is necessary to evaluate the relationship between alcohol consumption and blood pressure through stratification analyses according to the ALDH2 genotype. In this study, we evaluated the associations between alcohol consumption and blood pressure and hypertension after stratifying the ALDH2 genotype.
METHODS
Study population
This study was based on the Dong-gu Study, the framework of which has been described elsewhere.17 Briefly, the Dong-gu Study involved 9.260 participants aged ≥ 50 years who live in Gwangju, the metropolitan city in Korea. Of these, 495 participants with myocardial infarction or stroke were excluded. ALDH2 genotyping was missing for 31 participants and information on alcohol consumption was missing for 131 participants. Ultimately, 8,526 participants without missing values were included in the analyses.
Blood pressure measurement and definition of hypertension
Blood pressure was measured by trained investigators three times at the right upper arm using a mercury sphygmomanometer after the participants had rested for ≥ 5 minutes. We used the mean of the three blood pressure measurements in the analyses. Hypertension was defined as either systolic blood pressure (SBP) ≥ 140 mmHg or diastolic blood pressure (DBP) ≥ 90 mmHg or taking antihypertensive medication.
Assessment of lifestyles and comorbidities
Information on variables such as lifestyle and disease history was obtained through interview questionnaires. The frequency and amount per occasion of alcohol consumption were investigated; a non-drinker was defined as a participant who consumed less than one drink per month. Alcohol consumption was coded as non-drinker, less than one standard drink per day, or one or more standard drinks per day. Smoking status was coded as never, ex-smoker, or current smoker. Physical activity was coded as walking for at least 30 minutes on at least 5 days per week or not. Body mass index (BMI) was calculated in kilograms per meter squared from weight and height measured in a standing position without shoes. A history of diabetes was assessed using questionnaires.
Genotyping
Genomic DNA was extracted from peripheral blood using a QIAamp DNA Blood Mini Kit (QIAGEN, Valencia, CA, USA), according to the manufacturer's protocol. rs671 was genotyped by high-resolution melting (HRM) analyses, using a Rotor-Gene 6000TM (Corbett Research, Sydney, Australia). The forward primer (5′-TTGGTGGCTACAAGATGTCG-3′) and reverse primer (5′-CAGGTCCCACACTCACAGTTT-3′) polymerase chain reaction (PCR) primers producing a 97-bp amplicon. The reaction mixture for HRM included 200 nM PCR primers, 1 µM SYTO 9 fluorescent dye (Invitrogen, Carlsbad, CA, USA), 0.5U F‐Star Taq DNA polymerase (BioFACT), and 40 ng genomic DNA in 10 µL reaction volumes. The cycling conditions comprised an initial denaturation at 95°C for 5 minutes, followed by 40 cycles of 95°C for 5 seconds and 58°C for 30 seconds.
Statistical analysis
The baseline characteristics of the study population are presented according to gender and ALDH2 genotype. General characteristics are expressed as means ± standard deviations or number (%). The general characteristics of the participants were compared using t-tests for continuous variables, and χ2 tests for categorical data. Genotype was categorized as active ALDH2 (GG) and inactive ALDH2 (GA/AA). All analyses were carried out by gender. Multivariate linear regression was performed to assess the associations between ALDH2 and alcohol consumption and SBP and DBP. Multivariate logistic regression was performed to assess the associations between ALDH2 genotypes and alcohol consumption and hypertension.
RESULTS
Table 1 shows the baseline characteristics according to the ALDH2 genotype and gender. The GG, GA, and AA genotype frequencies were 69.0%, 28.4%, and 2.6%, respectively, and were in Hardy–Weinberg equilibrium (P = 0.141). Inactive ALDH2 carriers were significantly older and had a lower alcohol consumption and lower DBP than active ALDH2 carriers in both genders. They had a lower BMI and SBP and a higher prevalence of hypertension, and diabetes only in men.
Table 1
General characteristics of study subjects according to genotype of ALDH2 rs671
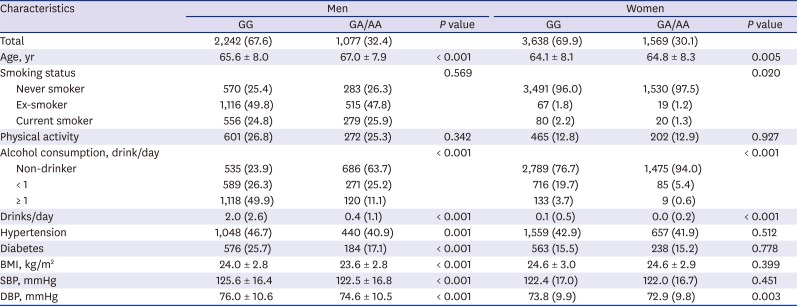
Table 2 shows the odds ratios (ORs) for hypertension in participants who were inactive ALDH2 carriers compared to active ALDH2 carriers. In the crude model, the ORs in men and women were 1.27 (95% confidence interval [CI], 1.10–1.47) and 1.04 (95% CI, 0.92–1.17), respectively. After adjusting for age, the risk difference was greater in model 1, and the ORs were 1.34 (95% CI, 1.16–1.56) in men and 1.09 (95% CI, 0.96–1.23) in women. In the final model, the ORs were 1.24 (95% CI, 1.06–1.45) in men and 1.08 (95% CI, 0.95–1.22) in women.
Table 2
Association between ALDH2 rs671 polymorphism and HTN according to gender

All values are given as odds ratio (95% confidence interval) or number (%).
Model 1 was adjusted for age. Model 2 was further adjusted for smoking, physical activity, diabetes mellitus, and body mass index.
ALDH2 = aldehyde dehydrogenase 2, HTN = hypertension.
aP value for interaction term between gender and ALDH2 rs671 genotype in model 2.
Table 3 shows the SBP and DBP according to ALDH2 genotypes and gender. The association between SBP and ALDH2 genotype was modified by gender (P for interaction = 0.002). In men, inactive ALDH2 carriers had a lower SBP and DBP, while in women, SBP did not differ significantly according to ALDH2 genotype, and inactive ALDH2 carriers genotype had a lower DBP.
Table 3
Association between ALDH2 rs671 polymorphism and blood pressure according to gender
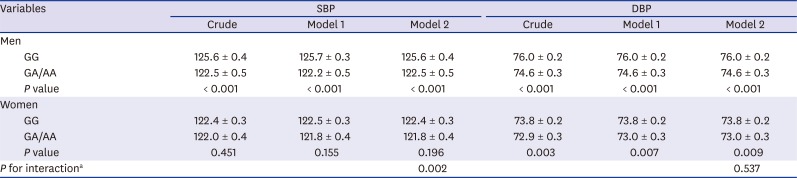
Values are given as adjusted mean ± standard error.
Model 1 was adjusted for age. Model 2 was further adjusted for smoking, physical activity, diabetes mellitus, and body mass index.
ALDH2 = aldehyde dehydrogenase 2, SBP = systolic blood pressure, DBP = diastolic blood pressure.
aP value for interaction term between gender and ALDH2 rs671 genotype in model 2.
Table 4 shows the association between alcohol consumption and the risk of hypertension according to ALDH2 genotypes and gender. The association between alcohol consumption and risk of hypertension was only significant in men who had the active ALDH2 genotype, while not significant in women.
Table 4
Association between alcohol consumption and HTN, stratified by gender and ALDH2 rs671 genotype
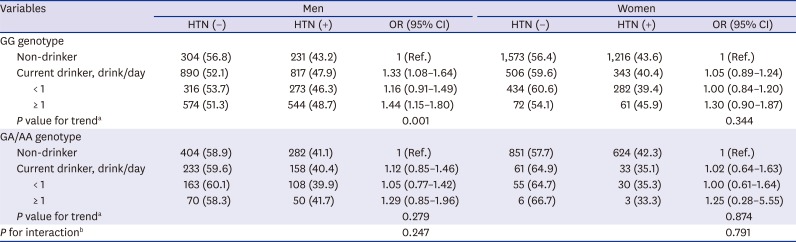
All models were adjusted for age, smoking history, physical activity, diabetes mellitus, and body mass index.
ALDH2 = aldehyde dehydrogenase 2, HTN = hypertension, OR = odds ratio, CI = confidence interval.
aTrend test from non-drinker, < 1 drink/day, to ≥ 1 drink/day; bP value for interaction term between alcohol consumption (non-drinker and current drinker) and ALDH2 rs671 genotype.
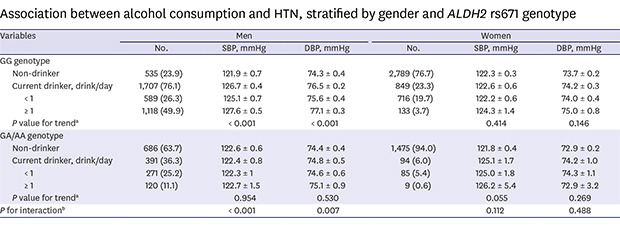
Table 5 shows the dose-response relationship between alcohol consumption and blood pressure for each ALDH2 genotype. The ALDH2 genotype modified the association between alcohol consumption and SBP (P for interaction < 0.001) and DBP (P for interaction = 0.007) in men, but not in women. The association between alcohol consumption and blood pressure was not significant in women, while in men, both SBP and DBP increased with alcohol consumption in the active ALDH2 carrier. By contrast, the inactive ALDH2 carrier was not related to alcohol consumption or blood pressure.
Table 5
Association between alcohol consumption and blood pressure, stratified by ALDH2 rs671 genotype
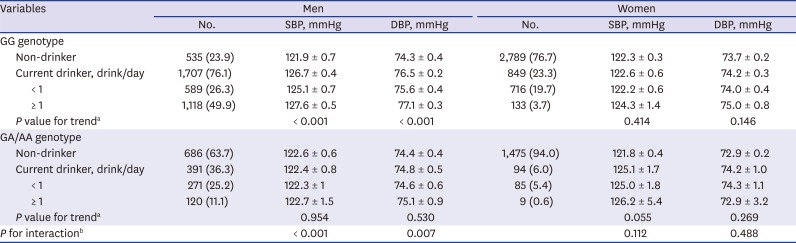
Values are adjusted mean ± standard error after adjusting for age, smoking history, physical activity, diabetes mellitus, and body mass index.
ALDH2 = aldehyde dehydrogenase 2, SBP = systolic blood pressure, DBP = diastolic blood pressure.
aTrend test from non-drinker, < 1 drink/day, to ≥ 1 drink/day; bP value for interaction term between alcohol consumption (non-drinker and current drinker) and ALDH2 rs671 genotype.
DISCUSSION
In this study, active ALDH2 carriers were associated with a high risk of hypertension in men. The association between alcohol consumption and SBP was dose-dependent in active ALDH2 carriers. However, there was no significant association between the ALDH2 polymorphism and hypertension and blood pressure in women.
In previous studies, active ALDH2 carriers had a higher risk for hypertension than inactive ALDH2 carriers.911121316 The difference in blood pressure according to the activity of ALDH2 can be explained by the difference in alcohol consumption. In previous studies, active ALDH2 carriers included a high prevalence of drinkers or greater alcohol consumption.8910 In our study, compared to inactive ALDH2 carriers, active ALDH2 carriers have 1.7 more drinks per day in men. In women, however, the amount of alcohol consumption was so small that the difference in consumption by the ALDH2 genotype was not significant.16 By contrast, Zhang et al.14 found no significant association between ALDH2 genotype and blood pressure in both never and current drinkers. In their study, there was an overadjustment bias due to the unnecessary adjustment of the frequency of alcohol consumption, an intermediate variable, in the association between ALDH2 genotype and blood pressure.18 In our study, active ALDH2 carriers had a 3.1 mmHg higher SBP and 1.4 mmHg higher DBP than inactive ALDH2 carriers in men. Ota et al.15 reported a 3.3 mmHg higher SBP and 2.6 mmHg higher DBP in active ALDH2 carriers compared to inactive ALDH2 carriers. In the study of Isomura et al.,12 the SBP and DBP of active ALDH2 carriers were 1.8 and 1.3 mmHg higher than those of inactive ALDH2 carriers, respectively. We also found a dose-response relationship between alcohol consumption and blood pressure in active ALDH2 carriers. Similarly, meta-analysis studies of observational studies and clinical trials found a positive dose-response relationship between the amount of alcohol consumption and incidence of hypertension,19 and reducing alcohol consumption led to lower blood pressure.4 Chronic alcohol consumption increases blood pressure via increased sympathetic nerve activity, reduced antioxidants, and impaired vascular relaxation.20
In our study, the ALDH2 genotype modified the association between alcohol consumption and blood pressure. There were dose-response relationships between alcohol consumption and SBP and DBP in active ALDH2 carriers, but no significant relationship in inactive ALDH2 carriers. In inactive ALDH2 carriers, it is not clear why blood pressure did not increase with the amount of alcohol consumption. Based on our results, we postulate that other blood pressure lowering effects of ethanol metabolites, such as aldehyde, counteract the ethanol-induced blood pressure increase. After alcohol consumption, inactive ALDH2 carriers have a fivefold higher peak blood aldehyde level than active ALDH2 carriers. Aldehyde lowers blood pressure in the early phase after drinking alcohol. In an animal study, an inactive ALDH2-like disulfiram-treated group had a lower blood pressure than a control group after ethanol administration.21 Few studies have evaluated the dose-response relationship between alcohol consumption and blood pressure according to the ALDH2 genotype. In contrast with our results, Ota et al.15 reported a significant positive association between the amount of alcohol consumption and SBP only in inactive ALDH2 carriers. However, their study population was small and consisted of only men workers with high alcohol consumption.
In inactive ALDH2 carriers, the difference in the amount of alcohol consumption among categories of alcohol consumption was not sufficiently large, so the association between alcohol consumption and blood pressure may not have been evaluated sufficiently. Drinkers who are inactive ALDH2 carriers consume less alcohol than drinkers who are active ALDH2 carriers.10 Because the difference in alcohol consumption between drinkers and non-drinkers in the inactive ALDH2 carrier is less than that of the active ALDH2 carrier, the effects of drinking on the increase in blood pressure were weak in inactive ALDH2 carriers. In our study, of those who drank more than one drink per day, those with the inactive ALDH2 genotype drank 2.88 drinks per day, whereas those with the active ALDH2 genotype had 3.89 drinks per day. The binge-drinking rate was 64.5% in the drinkers with the active ALDH2 genotype, but 28.5% in those with the inactive genotype (data not shown).
The main strength of our study was the large sample size, which enabled us to evaluate the association between alcohol consumption and blood pressure according to ALDH2 genotypes. The limitation of our study is that other polymorphisms affecting alcohol metabolism, such as ADH 1B (ADH1B), were not evaluated in this study. However, ADH1B polymorphism was not significantly associated with a high risk of hypertension13 or high blood pressure14 in previous studies.
In conclusion, there was a positive dose-response relationship between alcohol consumption and blood pressure in active, but not in inactive, ALDH2 carriers. Further studies are needed to clarify the mechanism of effect modification of the ALDH2 rs671 polymorphism on the association between alcohol intake and blood pressure.
 XML Download
XML Download