

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is a common heterogeneous disease characterized by chronic airway inflammation. The prevalence of asthma is increasing in many countries.123 It is estimated that there are about 300 million asthma patients worldwide and that the number is still increasing.1 Despite advances in prevention and treatment, asthma exacerbation remains a major threat to asthmatic patients. Hospitalization due to asthma exacerbation contributes largely to the healthcare expenses of asthmatic patients. According to research in the US, the costs of emergency department visits and hospitalization due to asthma exacerbation accounted for up to 80% of the direct costs of asthma patients.4
In China, little is known about the hospitalization of patients for asthma exacerbation. According to a domestic epidemiology study, the prevalence of asthma in mainland China is rapidly increasing in recent years,3 while risk factors of asthma exacerbation were not sufficiently investigated. This study aimed to investigate the clinical characteristics and outcomes of such patients in mainland China, with a view to improving control of the disease and lowering its economic burden.
MATERIALS AND METHODS
Study design
This is a retrospective study supervised by China Asthma Research Network (CARN) and conducted in 29 provincial hospitals in 29 provinces (autonomous regions/municipalities) across mainland China. The STROBE checklist was followed when this study was designed and conducted.5 The inclusion criteria were: 1) patients ≥14 years old; 2) hospitalized for asthma exacerbation; 3) diagnosed with asthma at least 3 months before admission according to the GINA criteria6; and 4) hospitalized between January 1, 2013 and December 31, 2014. If a patient was hospitalized more than once during the study period, only the last hospitalization was included. The criteria for the severity of asthma exacerbation was based on the Guidelines for the prevention and treatment of asthma published by the Chinese Medical Association of Respiratory Disease in 2008.7 An exemption from the informed consent of the study was approved by the Ethics Committee of China-Japan Friendship Hospital (ethics No. 2015-99).
Data collection
The flowchart of the study is shown in Fig. 1. Due to the lack of a commonly shared hospital information system in China so far, the investigators at each center searched the electronic medical record system for their hospital and enrolled patients who met the inclusion criteria. Information about the demographic features (age, sex), pre-admission conditions (history of smoking and hospitalization or emergency care due to asthma exacerbations during the previous year, and daily treatment), exacerbation details (triggering factor and severity), and outcomes were evaluated. The information on comorbidities was based on formal diagnoses extracted from the medical records, and the diagnosis of comorbidities, such as chronic obstructive pulmonary disease (COPD), was made by the doctors when the patients were hospitalized according to the international or domestic guidelines generally accepted. Non-adherence was defined as irregular use of the prescribed medications of asthma before the hospitalization.
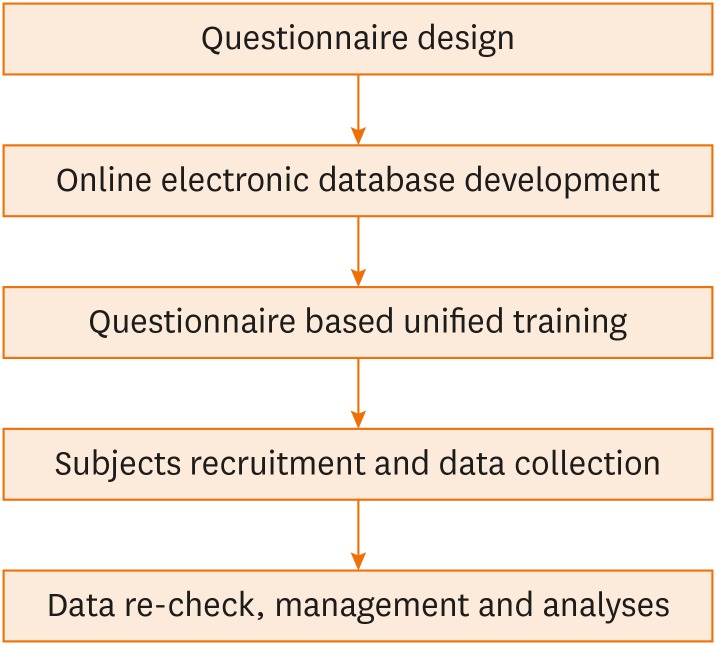
A questionnaire was designed and distributed among all CARN members (experts, specialists, or healthcare professionals) for validation prior to the final version was CARN-approved for use in this study. Accordingly, an online electronic database was developed. Investigators at each participating center were trained on how to enroll the patients, extract the information, and complete the questionnaire, for standardization and quality control. They completed the questionnaire on paper for each case, after which the data were input into the online electronic database. The paper questionnaires at each site were then mailed to the steering institution of this nationwide study, where two independent investigators double-checked the data in the database to ensure accuracy.
The number of patients hospitalized for asthma exacerbation each month and the total number of monthly respiratory hospitalizations in each center over the study period were also recorded.
Data analysis
IBM SPSS Statistics 24.0 (SPSS, Inc., Chicago, IL, USA) and GraphPad Prism 5.0 (GraphPad Software, San Diego, CA, USA) were utilized for analyses. For non-normally distributed data, median and quartiles were used for description. Numerical data with a non-normal distribution were compared using the Mann-Whitney U test. Differences between categorical variables were tested using the χ2 test. Logistic regression was used to examine the effects of various factors on the severity of asthma exacerbation. P values < 0.05 were considered statistically significant.
RESULTS
Demographic characteristics
In all, 3,240 asthmatic patients were included (57.7% females; 42.3% males). According to the common geographic division of China, of all the patients enrolled, 396 were from Northeast China, 532 from North China, 426 from Central China, 648 from East China, 235 from South China, 725 from Northwest China, and 278 from Southwest China. Most patients were non-smokers. Current smokers and ex-smokers accounted for 10.4% and 13.4%, respectively (Table 1). Further analyses by age group showed that, in each age group, there were more females than males. The percentage of having a smoking history was higher in patients in older age groups; and for every age group, male patients were more likely to be smokers (Table 2).
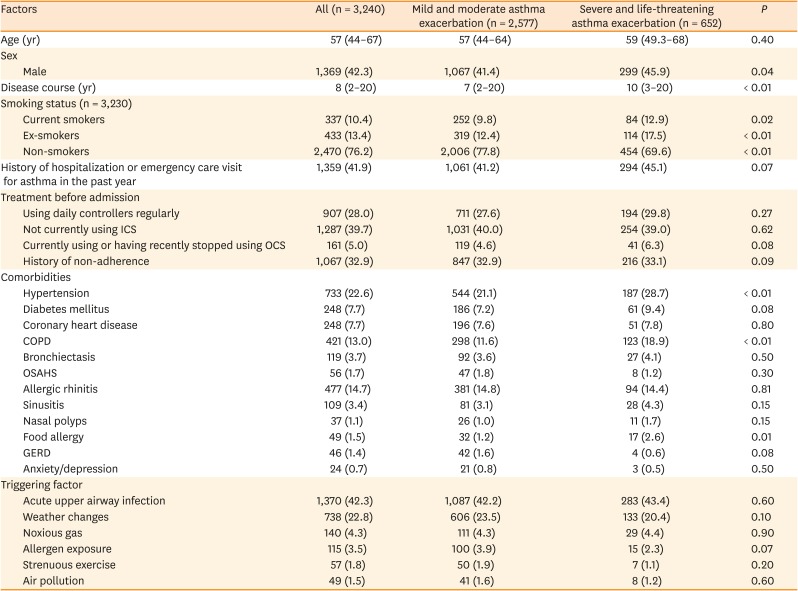

Table 1
Demographic and clinical characteristics of the study patients
Values are presented as median with quartiles or number of patients (%).
ICS, inhaled corticosteroid; OCS, oral corticosteroid; COPD, chronic obstructive pulmonary disease; OSAHS, obstructive sleep apnea and hypoventilation syndrome; GERD, gastroesophageal reflux disease.
![]()
Table 2
Sex and smoking history differences in different age groups
![]()
History of treatment before hospitalization and comorbidities
About half of the patients had a history of hospitalization or emergency department visit for asthma in the previous year. Only 28.0% of the patients regularly used daily controller medications, including inhaled corticosteroid (ICS), long-acting β2-agonist (LABA), ICS/LABA, oral leukotriene receptor antagonists, oral corticosteroid (OCS), and theophylline. One thousand two hundred and eighty-seven patients (39.7%) were not using ICS currently, 161 patients (5.0%) were using OCS currently or until recently, and 1,067 (32.9%) patients had a history of non-adherence.
Comorbidities are summarized in Table 1. The prevalence of hypertension, diabetes mellitus, and coronary heart disease was 22.6%, 7.7%, and 7.7%, respectively. Of the patients, 13.0% had COPD, while 14.7%, 3.4%, and 1.1% had allergic rhinitis, sinusitis, and nasal polyps, respectively. Fifty-six (1.7%) of the patients had obstructive sleep apnea and hypoventilation syndrome, 49 (1.5%) had food allergy, 46 (1.4%) had gastro-esophageal reflux disease, and 24 (0.7%) had psychiatric problems such as depressive and anxiety disorders.
Details of the exacerbations
Factors triggering the exacerbation are summarized in Table 1. Acute upper airway infection triggered nearly half of all exacerbations. The first 6 leading triggering factors, in sequence, were acute upper airway infection, weather changes, noxious gas, allergen exposure, strenuous exercise, and air pollution. Most patients had mild to moderate exacerbations, with severe and life-threatening exacerbation accounting for about one-fifth of all cases.
Risk factors for severe asthma exacerbation
After excluding 11 patients who lacked complete information on severity, the remaining patients were categorized into 2 groups (mild-to-moderate and severe-to-life-threatening) based on the severity of exacerbation (Table 1). The characteristics of these 2 groups were compared using the Mann–Whitney U test (for age and disease course) or the χ2 test (for other factors). As shown in Table 1, patients in the more severe group had older median ages, although the difference was not significant. The disease course of patients in the more severe group was significantly longer (P = 0.0003). More patients in the severe group were male and had a smoking history (either current smokers or ex-smokers). Patients with more severe exacerbations were more likely to have hypertension, COPD, and food allergy (all P < 0.05). The differences in medication use before hospitalization and triggering factors between the 2 groups failed to reach statistical significance.
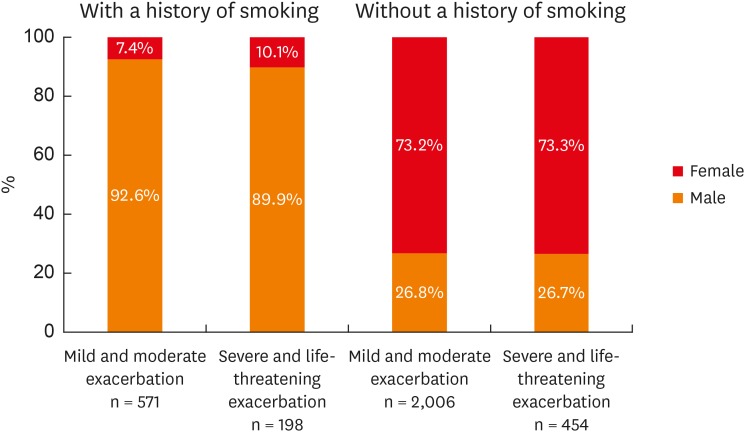
Although the severer group included more males than the less severe group, this difference may be related to the higher incidence of smoking history in male patients. Thus, we subdivided patients according to smoking history; this analysis showed that, in both patients with and without a smoking history, female patients were more likely to be in the severe group, but the differences were not significant (Fig. 2).
A multivariate analysis was performed to further evaluate the potential risk factors for the severity of asthma exacerbations. As shown in Table 3, a smoking history, comorbidities of hypertension, COPD, and food allergy were independent risk factors for severe exacerbation.
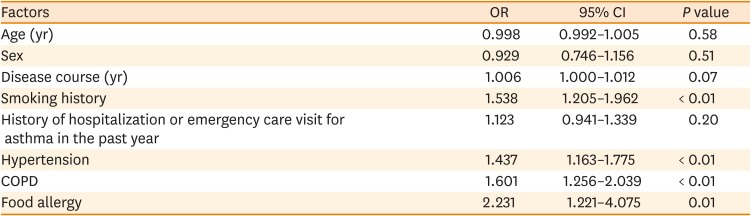
Table 3
Multivariate analysis of risk factors for the severity of asthma exacerbation (mild or moderate vs. severe or life-threatening)
![]()
Seasonality of hospitalization
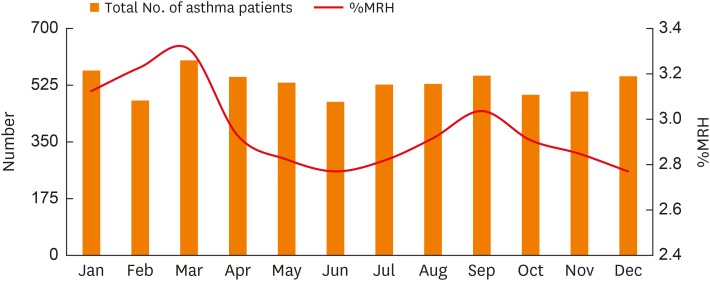
We calculated the number of patients hospitalized for asthma exacerbation each month and its proportion in the monthly respiratory hospitalizations over the study period (Fig. 3). The number of patients hospitalized for asthma exacerbation and its proportion in the monthly respiratory hospitalizations varied with seasonal changes; 2 peaks were obvious, one in March and the other in September. Further analysis showed that the proportion of hospitalization of asthma exacerbation in the monthly respiratory hospitalizations was higher in the northern cities, and that the seasonal fluctuations in the hospitalizations of asthma exacerbation in the northern cities were more obvious than in the southern cities (Supplementary Fig. S1).
Outcomes
The mean length of hospital stay was 8 (range, 6 to 11) days. Seventy-three (2.3%) patients were admitted to the intense care unit, and 73 (2.3%) patients underwent mechanical ventilation. Eight patients died during hospitalization, with an overall mortality of 0.25% (Table 4). These 8 patients were hospitalized during the period November to March; of these patients. 3 had metabolic or cardiovascular comorbidities, such as hypertension, diabetes mellitus, and coronary arterial disease. 2 had infectious diseases, such as tuberculosis and invasive pulmonary aspergillosis. And 2 died due to cardiac complications.
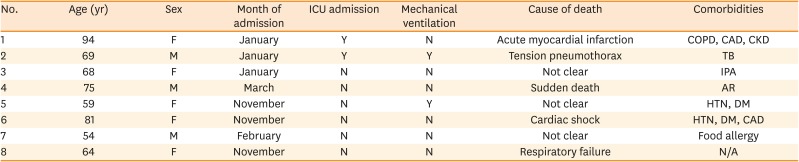
Table 4
Details of patients who died during the study period
ICU, intensive care unit; F, female; M, male; COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease; CKD, chronic kidney disease; TB, pulmonary tuberculosis; IPA, invasive pulmonary aspergillosis; AR, allergic rhinitis; DM, diabetes mellitus; N/A, not applicable.
![]()
DISCUSSION
This retrospective study summarized the clinical characteristics and outcomes of patients hospitalized for asthma exacerbation in 29 provincial hospitals in 29 provinces, autonomous regions, or municipalities throughout mainland China. No previous multi-center large-scale study of asthma inpatients on the present study topic in mainland China has been reported. The results of this study provide insights into this patient population, which may facilitate disease control and lower the economic burden of asthma exacerbation in the future.
For adults, the prevalence of asthma was higher in women than in men.6 Several previous studies that included inpatients hospitalized for asthma exacerbation also showed a similar tendency.89 The reasons for this sex-related difference are not clear, but may involve hormonal changes and genetic susceptibility.10 In this study, there were more female than male patients, but the male patients tended to have more severe exacerbations. This may be because male patients were more likely to have a smoking history. Further analyses that discriminated between patients with and without a smoking history showed that the differences between the sexes in terms of disease severity were not significant.
There is a close relationship between tobacco smoking and asthma. For asthmatic patients, smoking is related to poor asthma control,11 an accelerated lung function decline,12 and a poor response to inhaled or systemic corticosteroids.13 An epidemiological study performed in 8 provinces of China in the period 2010-2012 showed that, among asthmatic patients >14 years old, 34.5% were smokers. Compared to nonsmokers, asthma patients who had a smoking history had a lower control rate, and a higher rate of hospitalization and emergency department visits.14 The ratio of patients with a smoking history was 23.5% in this study, which was lower than in the previous study.14
In this study, the proportion of patients who used daily controller medications regularly before hospitalization was relatively low. It is recommended that all patients with persistent asthma use long-term control medications such as ICS daily.6 A meta-analysis showed that, even for patients with well-controlled asthma, the withdrawal of low-dose ICS was related to an increased risk of asthma exacerbation.15 More than one-third of patients overall and about half of the patients who had a history of hospitalization or emergency department visit for asthma exacerbation in the previous year were not using ICS before hospitalization, indicating that many of the patients were not using the recommended medications. This may have led to poor control of the disease and frequent exacerbations.
Asthma symptoms vary with seasons. This study showed that the number of patients hospitalized for asthma exacerbation had seasonal fluctuations, with 2 obvious peaks in March and September, similar to previous studies. Two studies that included patients hospitalized for asthma exacerbation in the US and Canada showed that, for elderly patients, hospitalization peaked during winter, while for younger patients, the peak occurred around September.1617 A study in Korea showed that there were spring and autumn peaks of asthma exacerbation for children and adults, respectively, but only 1 winter peak for the elderly patients. The association between asthma exacerbation and influenza was greatest in patients aged over 60 years old.18 The increased hospitalization of the elderly asthma patients in winter may be caused by the increased prevalence of airway infection, which is a strong triggering factor of asthma exacerbation. The increased hospitalization rate of school-age children in September has been ascribed to epidemics of respiratory viral infection after school starts.19 However, several studies in China have reported that there was a strong relationship between asthma symptoms and airborne pollen levels. Yao and Zhang20 revealed that the peak of the concentration of airborne autumn pollen in North China occurred between August and September, and that most outpatients with hay fever or asthma in that period were allergic to Mugwort or Humulus pollen. As autumn pollen allergens are the most important allergic pollen for asthmatic patients in China, the September hospitalization peak may be explained by pollen allergy, but further studies are needed to prove it. Further analyses comparing the difference between the northern and southern cities showed that the seasonal fluctuations in hospitalization of asthmatics in the southern cities were less obvious than in the northern cities. The reasons for the results may be colder temperature, higher rates of respiratory infections, and more serious air pollution in the winter of northern cities.
The prevalence of asthma is increasing worldwide, but several studies have reported that asthma mortality is decreasing in some countries.2122 Kaur et al.8 reported that the mortality of asthmatic inpatients during the period 2001-2010 in the US was 1%. In England, Watson et al.23 reported that the mortality of adult asthmatic inpatients during the period 2000-2005 was 1.3%. In the present study, the mortality of asthmatic inpatients was 0.25%, which is lower than that reported in other countries. Higher levels of comorbidities have been associated with the increased mortality in elderly asthmatic patients.24 Most of the 8 patients who died in our study had comorbidities, such as hypertension, diabetes mellitus, and coronary artery disease; of these, 2 died from cardiac complications. Two of the patients had infectious comorbidities: tuberculosis and invasive pulmonary aspergillosis, respectively. Asthma exacerbation was the primary cause of hospitalization of these patients, but the comorbidities may contribute to the worsening of the disease. As many patients received systemic glucocorticoids during hospitalization, they were at high risk of developing infections, such as tuberculosis or aspergillosis, which may further worsen the condition of the patients. All of the deceased patients had been admitted to the hospital from November to March, which are the coldest months in most of mainland China. Several studies have reported that the mortality of asthmatic patients increased during winter, perhaps due to the high prevalence of respiratory viral infections.8
The study had some limitations. First, this is a retrospective study, and the information was extracted from medical records, which may introduce some bias as medical records may not cover the complete history of the patients. Secondly, all the medical centers participating in this study were provincial hospitals located in the capitals of provinces, autonomous regions, or municipalities. There may be a regional imbalance, so that these centers may not comprehensively reflect the situation in some less-developed areas. More extensive studies are needed to obtain more detailed information about asthmatic patients.
This study involving 29 hospitals located in 29 regions that covered most parts of China improved our understanding of patients hospitalized for asthma exacerbations in this country and provided evidence for decision-making. In these Chinese patients, severe exacerbations of asthma were related to a history of smoking, comorbid hypertension, COPD, and food allergy; the exacerbations were mostly triggered by acute upper airway infection which peaked during March and September each year. We noted the underuse of daily controller medications among patients before hospitalized for asthma exacerbation. Regardless of rapid and wide-spreading patient education on self-management of asthma in China during recent years, the low patient adherence to daily controller medications as revealed in this study indicated more educational efforts and considerations should be needed.
 XML Download
XML Download