

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Drug-induced liver injury (DILI) has been an increasing pharmacovigilance concern over recent decades. Although it is difficult to identify, the overall incidence of DILI is reported to range from 1 in 10,000 to 1 in 100,000 drug-exposed patients, and this figure is even lower for many drugs.1 The clinical manifestations of DILI vary from transient, asymptomatic elevation in liver enzymes to symptomatic, severe hepatic failure that requires liver transplantation.23 DILI can thus cause serious adverse clinical outcomes and is the leading cause for withdrawal of approved drugs from the market.45 As the mortality rate of DILI is approximately 10% and >15% of DILI cases are complicated by chronic liver injury including cirrhosis,678 it is crucial to accurately identify DILI and to determine the possible causative drug when liver function test (LFT) elevation occurs.
Considering that DILI is frequently subclinical and thus misdiagnosed, the actual incidence and characteristics of DILI remain unknown. For the treatment of DILI, identifying and stopping administration of the causative drug is essential. Therefore, understanding the epidemiological characteristics of DILI is important for early recognition of causative agents. Nevertheless, few studies for diagnosis of DILI in hospitalized patients were identified and such studies were limited by small sample populations. One of the reasons for the insufficiency of epidemiological data on DILI is that it is not easy to detect DILI cases when researching as well as when treating patients. The wide array of presentations, variety of causative agents, lack of objective diagnostic markers, and exclusion diagnosis complicate identifying DILI.9 A recent review of previous research on DILI diagnosis indicated that among 2,906 cases of initially assumed DILI, about a quarter of them were misdiagnosed or undiagnosed due to overt alternative causes or confounding variables.10 Several studies have attempted to identify DILI and improved the accuracy of diagnosis for DILI and its risk stratification using liver function parameters, diagnostic codes and text search names of suspected drugs.111213 However, these criteria are neither specific nor capable of predicting clinical courses. According to a meta-analysis published in 2018, the DILI algorithm in previous publications showed the overall positive predictive value (PPV) of about 15%.13
This study aimed to evaluate the epidemiological characteristics of DILI in Korea, and further develop and establish a universally applicable algorithm for the diagnosis of DILI based on electronic health records (EHRs).
MATERIALS AND METHODS
Patients and study protocol
From June 2015 to May 2016, a retrospective analysis was performed on patients admitted to 3 university hospitals in Korea as follows. Asan Medical Center with its 2,800 beds is one of the largest teaching hospitals in Korea; Seoul National University Bundang Hospital is also a large tertiary care hospital with 1,700 beds; and Seoul Metropolitan Government-Seoul National University Boramae Medical Center is a secondary hospital with 800 beds.
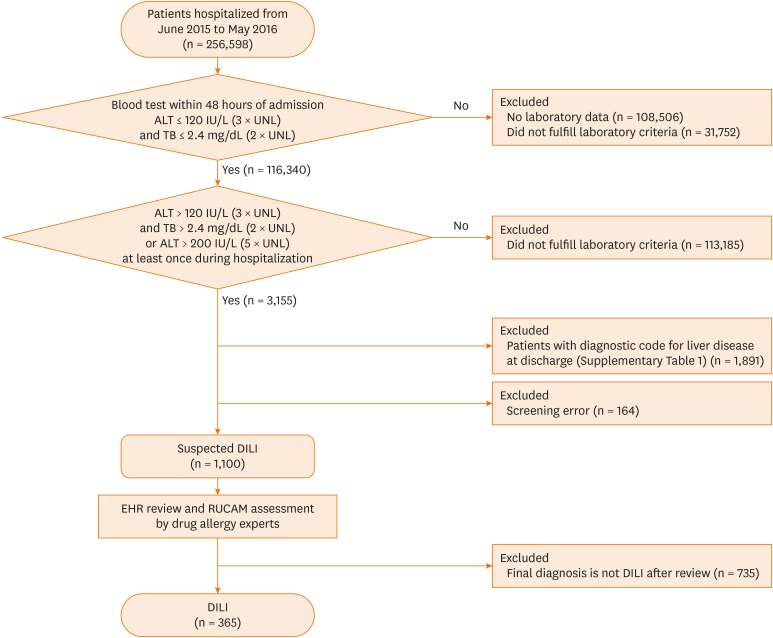
We developed a screening algorithm applicable for different EHRs based on recommendations from the international DILI expert group.14 The algorithm is illustrated in Fig. 1. First, patients who showed alanine transferase (ALT) ≤ 120 IU/L (3 times the upper limit of normal [ULN]) and total bilirubin (TB) ≤ 2.4 mg/dL (twice ULN) in blood test within 48 hours after admission were selected. Next, patients with 1) ALT > 120 IU/L and TB > 2.4 mg/dL or 2) ALT > 200 IU/L (5 times ULN) at least once during hospitalization were identified. Subsequently, patients with liver-related diseases, such as infection, malignancy, pancreaticobiliary disease, autoimmune disease and alcoholic hepatitis, as discharge diagnoses were excluded on the basis of International Classification of Diseases, 10th edition (ICD-10) codes, although chronic hepatitis B and C were not excluded considering the high prevalence in Korea (Supplementary Table S1). The remaining patients were included in the suspected DILI group.
Fig. 1
Algorithm flowchart identifying DILI in the hospitalized patients.
DILI, drug-induced liver injury; ALT, alanine transferase; UNL, upper limit of normal; TB, total bilirubin; EHR, electronic health record; RUCAM, Roussel Uclaf Causality Assessment Method.
For these cases, 2 or more drug allergy experts reviewed EHRs to confirm the diagnosis of DILI and to collect data on their clinical characteristics. Liver injury was categorized as hepatocellular, cholestatic and mixed based on the ratio of serum ALT to alkaline phosphatase (ALP). A hepatocellular pattern was defined as a ratio ≥ 5, a cholestatic pattern as a ratio ≤ 2, and a mixed pattern as a ratio > 2 and < 5.15 For each culprit agent, drug causality assessment was performed by using Roussel Uclaf Causality Assessment Method (RUCAM), which is the most widely used scale for diagnosing DILI.1516 A causal relationship between the causative drug and DILI is classified as highly probable (>8), probable (6–8), possible (3–5), unlikely (1–2) or excluded (<0).
After investigating common causative agents for DILI, crude incidences of DILI by drug were estimated using the number of patients taking prescription drugs. Patients with >1 prescription for a culprit drug in the computerized prescription program were defined as prescribed patients.
EHR system and data extraction
According to the study algorithm, data was extracted using a clinical data warehouse program, based on BESTcare 2.0 in Seoul National University Bundang Hospital and on the BESTcare 1.0 system in Seoul Metropolitan Government-Seoul National University Boramae Medical Center, which was developed by EZ Caretech Co. (Seoul, Korea). In Asan Medical Center, we used the ABLE (Asan BiomedicaL research Environment), an anonymized clinical research information system based on Microsoft SQL Server Parallel Data Warehouse.
Statistical analysis
All statistical analyses were performed using SPSS version 24.0 (SPSS Inc., Chicago, IL, USA). Categorical variables are presented as numbers and percentages, which were analyzed using the χ2 test and Fisher's exact test. Continuous variables are presented as mean ± standard deviation with ranges, which were analyzed using Student's t test, analysis of variance test or Mann Whitney U test with a 95% confidence interval (CI). Incident rate and 95% CI values were estimated from population size, and differences between groups were considered significant at P < 0.05. PPV was defined as the percentage of confirmed DILI cases from the total number of EHR cases identified by the study algorithm.
Ethics statement
The study was approved by the Institutional Review Boards (IRB) of Asan Medical Center (IRB No. S 2016-1507-0002), Seoul Metropolitan Government-Seoul National University Boramae Medical Center (IRB No. 26-2016-124/102) and Seoul National University Bundang Hospital (IRB No. B-1611/369-102). The present study used retrospective observational analysis, and informed consent was waived by the boards.
RESULTS
Performance of the screening algorithm
The flowchart of the screening process is provided in Fig. 1. Between June 2015 and May 2016, a total of 256,598 patients were admitted to the 3 hospitals; 108,506 patients (42.2%) who did not have laboratory data were excluded, with 1,100 (0.43%) among them were identified by the screening algorithm as suspected cases of DILI. The proportions of patients screened among the 3 hospitals were 0.39% (560 cases/144,457 inpatients) at Asan Medical Center, 0.42% (294 cases/69,571 inpatients) at Seoul National University Bundang Hospital and 0.57% (246 cases/42,570 inpatients) at Seoul Metropolitan Government-Seoul National University Boramae Medical Center.
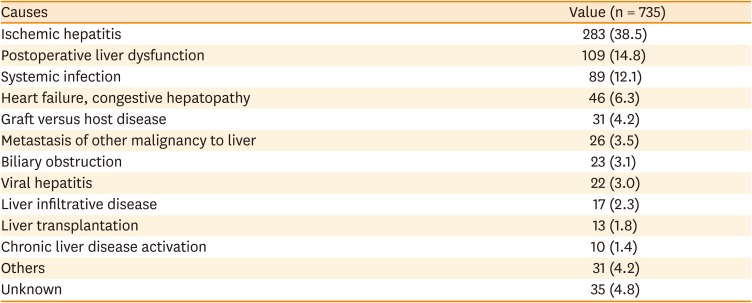
Of 1,100 suspected DILI cases, 735 were excluded after EHR review, and the remaining 365 cases (0.14%, 95% CI, 0.13–0.16) were identified as DILI. No significant differences were observed in proportions of DILI cases among hospitals (P = 0.392), and the PPV of our algorithm was 33.1%. The most common reasons for exclusion were ischemic hepatitis (n = 238, 32.4%), followed by postoperative liver dysfunction (n = 109, 14.8%). Other reasons included graft versus host disease, exacerbation of chronic liver disease, liver metastases and infiltrative liver disease (Table 1).
Table 1
Reasons for exclusion of suspected drug-induced liver injury cases
Clinical characteristics of DILI
The baseline demographics and clinical characteristics of DILI patients are shown in Table 2. The median age of patients was 52 years (range 0–92), of whom 84.1% (n = 307) were 18 years or older, and 64.4% (n = 235) were women. Ninety-one (26.5%) patients had solid cancers and 66 (18.1%) had hematologic malignancy such as acute leukemia and lymphoma. Furthermore, 88 (24.1%) patients had a history of adverse drug reactions, including 11 (3.0%) patients with DILI, and 201 patients (55.1%) had taken some medication before hospitalization (recent medication).
Table 2
Baseline demographical and clinical characteristics of subjects diagnosed as drug-induced liver injury
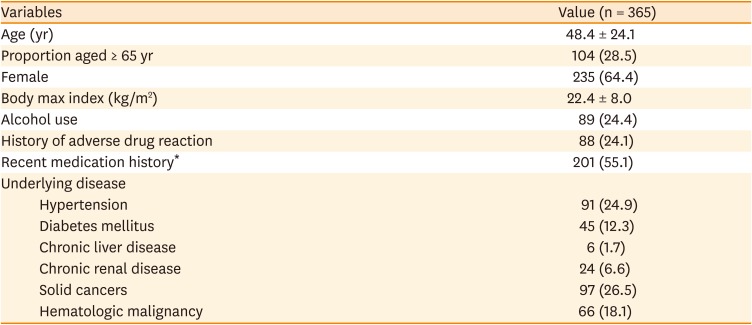
Table 3 shows the clinical characteristics and courses of DILI. The median duration between DILI diagnosis and normalization of ALT (< 40 IU/L) was 12 days. Although 223 patients recovered after discontinuing the culprit drug, records for 79 were incomplete due to discharge before full recovery, death or follow-up loss, thus classified as ‘Unknown.’ Eleven patients with severe clinical presentation were administered systemic steroids. DILI resolved in most patients (n = 273, 74.8%), though 76 (22.8%) patients who were discharged with improving status were classified as unknown due to lack of follow-up laboratory data. Among all DILI patients, 15 (4.1%) died during hospitalization, including 4 patients (1.1%) who were treated in an intensive care unit, but none underwent liver transplantation. Most patients experienced DILI as transient LFT elevations and recovered, and died due to underlying disease progression or uncontrolled infection. Two (0.5%) patients were considered to have died due to DILI-related causes: One patient developed DILI after receiving antituberculosis drugs for tuberculosis encephalitis, after which acute renal failure developed and died due to multi-organ failure despite receiving intensive care unit (ICU) care. The other patient had been receiving ICU care for acute respiratory distress syndrome from adenovirus infection, but developed DILI supposedly from valproate or antibiotics (imipenem-cilastatin); liver transplantation was considered, but the patient died due to uncontrolled infection.
Table 3
Characteristics, outcomes, and management of DILI
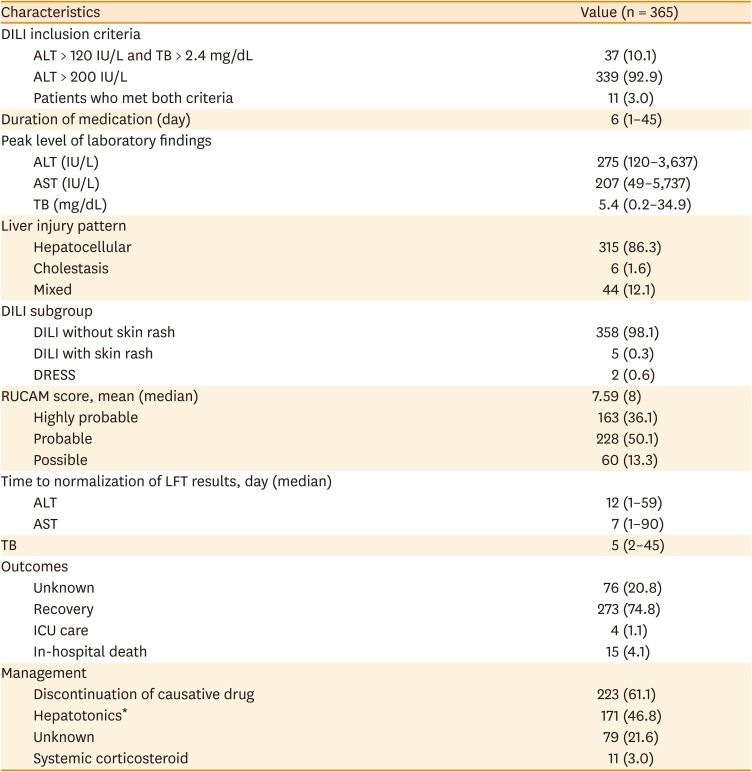
Values are presented as number (%) or median (range).
DILI, drug-induced liver injury; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DRESS, drug reaction with eosinophilia and systemic symptoms; LFT, liver function test; ICU, intensive care unit; RUCAM, Roussel Uclaf Causality Assessment Method; TB, total bilirubin.
*“Hepatotonics” included drugs commonly used for liver disease such as ursodeoxycholic acid, Carduus marianus extract (Legalon®), biphenyl dimethyl dicarboxylate-containing formulations (e.g., Godex®), and HepaMerz®.
Causative agents
A total of 453 drugs were suspected to be responsible for DILI. Usually a single drug was the causative agent, although sometimes several drugs were administered simultaneously. Thus, a single agent was identified in 298 cases and >1 drug was implicated in 67 cases. Among all cases, 314 cases (86.1%) of DILI causative agents were classified as probable or highly probable group after RUCAM assessment.
Fig. 2 shows the frequency of drug classes and individual agents that cause DILI. Major classes were antibiotics (n = 214, 47.2%), followed by chemotherapeutic agents (n = 87, 19.2%). Anticoagulation-related drugs included warfarin, new oral anticoagulant, heparin and low-molecular-weight heparin. Gastrointestinal (GI) medication included proton pump inhibitors, antacids and GI motility agents. Among antibiotics, piperacillin-tazobactam was the most common individual agent (n = 38, 8.4%).

Incidence by individual agents
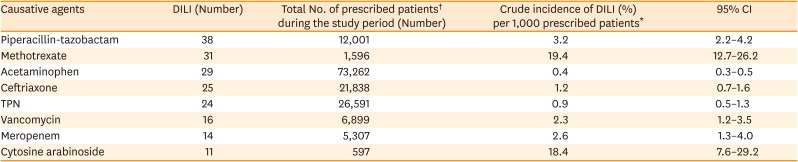
Total numbers of patients who received a prescription drug during the study period (prescribed patients) were analyzed to calculate the incidence of DILI by individual agent. Methotrexate was identified for 1.94% of patients who received prescriptions (19.4 cases per 1,000 prescribed patients), while cytosine arabinoside was administered in 1.84% (18.4 cases per 1,000 prescribed patients), indicating that the incidence of DILI caused by chemotherapeutic agents is relatively high. Among antibiotics, piperacillin-tazobactam was most commonly prescribed, with a DILI incidence of 0.32% (Table 4).
Table 4
Incidence of DILI by causative agent
Characteristics of DILI according to the RUCAM score and drug classes
Supplementary Tables S2 and S3 showed the clinical characteristics of DILI patients classified using the RUCAM scale and drug classes. Except for mean age which was high in the highly probable DILI group (P = 0.024), no significant differences by sex, alcohol-use history, underlying liver disease, recent medication or causative drug were observed. DILI caused by chemotherapeutics had relatively shorter drug exposure times (average 2.8 ± 2.1 days) based on the results of comparisons among the most common 3 drug classes (antibiotics, chemotherapeutics and acetaminophen).
DISCUSSION
In this retrospective, multicenter study, antibiotics and chemotherapeutic agents were found to be frequent causative agents of DILI in hospitalized patients. Piperacillin-tazobactam was the most common individual agent, although the incidence of DILI per prescribed patient was highest for chemotherapeutics despite a relatively short exposure time. Using our study algorithm to evaluate DILI based on EHR, about 0.48% of hospitalized patients were screened as suspected DILI, of whom 365 (0.14%) were identified with DILI after a retrospective EHR review. Therefore, the PPV of the algorithm reached 31.1%. Most patients recovered from DILI, and about 2 weeks were required for ALT results to normalize.
During the last few decades, DILI has been investigated using large-scale registries. The incidences of DILI reported in a population-based retrospective study in the UK and an outpatient hepatology clinic of a single center in Sweden were 2.4 per 100,000 persons per year17 and 2.3 cases per 100,000 inhabitants per year, respectively.18 The annual incidence of DILI was reported to amount to 13.4–19 of 100,000 inhabitants per year in France and Iceland.1920 Also, the estimated incidence of hospitalization for DILI in Korea was 12 per 100,000 persons per year according to a prospective multicenter study.21 In medical inpatients, the incidence was reported as 1.4%,22 but the actual number may be higher due to under-reporting and missed diagnoses. In our results, the incidence of DILI was 0.14% of inpatients, which is likely to be low because, unlike previous studies, we excluded the diagnosis of toxic hepatitis and included only those DILI cases that occurred during hospitalization.
Although laboratory criteria for defining DILI in previous studies were not entirely consistent, coherent values, such as the Council for International Organization of Medical Science (CIOMS) scale15 and Hy's law,22324 exist. The CIOMS scale defined at least 2 of 3 groups: 1) ALT > 2 times ULN, 2) direct bilirubin > 2 times ULN, or 3) combined increase in aspartate aminotransferase, ALP, and TB with one value above 2 times ULN. Previously, the Food and Drug Administration recommended levels of ALT > 3 times ULN as a sensitive threshold of DILI25; however, this value is nonspecific. In 2011, the international DILI expert working group suggested the following refined criteria14: 1) ALT > 5 times ULN, 2) ALP > 2 times ULN or 3) ALT > 3 times ULN and TB > 2 times ULN. The latter constellation of criteria is referred to as Hy's law, which was widely used to predict fulminant hepatic failure723; however, ALT > 5 times ULN has shown a stronger predictive power to detect DILI.1326 We referred to these current criteria to define DILI in the present study, except for ALP because these values were missing in the pilot study, and the purpose of this study was to develop a simple algorithm applicable in multiple centers.
Several previous investigations reported identification of DILI based on abnormal laboratory data using a computerized hospital information system.27282930 However, the meta-analysis of Tan et al.,13 performance of the DILI identification algorithm in 29 previous studies had low PPV, ranging from 1.0% to 40%. In 2000, Bagheri et al.31 studied 1,964 patients with LFT results over a 5-week period at a single center, and 147 patients were selected using ALT > 2 times ULN and ALP > 1.5 times ULN as criteria. Of these cases, 13 (8.8%) were identified as DILI. In 2005, Meier et al.22 estimated the incidence of DILI in medical inpatients over 5 years. A total of 6,383 patients were enrolled following CIOMS criteria. Of the 489 patients identified, 88 (17.9%) were diagnosed with DILI, and the incidence was 1.4% (95% CI, 1.0–1.7). Those studies were mostly limited to a single center or a short study period and did not include the criterion of ALT > 5 times ULN; in addition, no previous study investigated DILI after admission of patients with normal pre-admission liver functions.
In this study, of the 1,100 DILI patients identified, 33.1% were actual DILI cases, suggesting that the screening power of the study algorithm has improved compared to algorithms used in previous studies. Probably, criteria used by the international DILI working group were more specific than criteria used in previous investigations. However, the algorithm still requires expert review, and several problems remain for the automation of DILI diagnosis. Reasons for the exclusion of cases from the study were mainly ischemic hepatitis following hypoperfusion due to septic shock, cardiogenic shock or post-cardiopulmonary resuscitation. Elevated LFT results related to surgical procedures, such as cardiopulmonary bypass used in cardiac valve replacement or liver retraction in open surgery, were also the dominant causes. Therefore, to improve the sensitivity and specificity of the protocol, the above differential diagnoses should be considered. Most DILI patients recovered within 2 weeks after the causative drug was stopped. However, serious hepatic dysfunction (requiring systemic steroids) or ICU treatment, and even death, occurred. The overall mortality of DILI in the present study was 4.1%; however, previous studies reported this value to reach up to 30%, depending on the drug.32 Thus, it is essential to monitor elevated LFT results and discontinue unnecessary drug administration to prevent DILI.
Causative agents of DILI also vary. Previous studies have revealed that antibiotics account for 27%–65% of the causative drugs.33 Among the antibiotics, amoxicillin-clavulanate was the most common agent.26819 We found that antibiotics were the major class of causative agents, among which piperacillin-tazobactam was the most common single agent. The incidence of DILI associated with piperacillin-tazobactam administration was 3.2 cases per 1,000 prescription patients. Antituberculosis drugs were also noted in previous research.2834 Devarbhavi et al.3235 reported that antituberculosis drugs were the leading causes of DILI in India and that the overall mortality reached 30%. Considering the high prevalence of tuberculosis in Korea, antituberculosis drugs were expected to be a common cause; however, our findings do not provide any insight into this relationship, because tuberculosis is mainly diagnosed and treated in outpatient clinics. Furthermore, chemotherapeutic agents, such as methotrexate, were commonly administered drugs, probably due to the nature of the referral hospital where more severe cases are seen.
Our study has several limitations. First, we conducted a retrospective analysis using an arbitrarily designed protocol. Although drug allergy experts and hepatologist suggested this algorithm, based on profuse literature reviews and several discussions, the risk of selection bias existed. Initially, we considered obtaining sensitivity using the toxic and drug-induced hepatitis (K716) ICD code, but it was impossible due to the large number of missing values of diagnostic codes. Consequently, sensitivity, specificity and negative predictive values were difficult to obtain for the algorithm, and only the PPV of our algorithm was identified according to the method by Tan et al. (the number of patients finally diagnosed with DILI/the number of patients screened with the protocol).13 Furthermore, part of the data was classified as unknown due to the retrospective nature of the study, particularly regarding the management and prognosis of DILI. Secondly, we selected patients who had normal LFT values within 48 hours after admission and excluded several ICD-10 codes associated with liver and pancreaticobiliary disease, including toxic hepatitis. In doing so, DILI caused by herbal medication before admission and transferred DILI cases may have been excluded; therefore, the actual incidence of DILI could also have been underestimated. However, considering the low prevalence of DILI in previous investigations, the number of patients excluded was not high, thus the algorithm can provide informative epidemiological data to investigate DILI developed purely during hospitalization (incidental DILI). Thirdly, criteria related to ALP were not included in the screening algorithm due to many missing values in the pilot study. Finally, since this study was conducted at 3 university hospitals, the possibility of referral bias cannot be excluded. However, considering that these hospitals represent secondary to tertiary treatment facilities within the healthcare delivery system, the present study does provide meaningful information on the characteristics of DILI in patients from a medium-sized, community-based hospital to a major teaching hospital.
Elevated LFT results in hospitalized patients are a common manifestation that should always be considered to be a possible sign of an adverse drug reaction. The results of the present study are meaningful as they suggest a potential screening algorithm that is universally applicable in different centers to detect DILI based on EHR, especially cases developed during hospitalization. Furthermore, physicians should be aware of DILI in patients under long-term treatment especially when antibiotics or chemotherapeutic agents are administered. Further studies aimed at modifying the screening protocol to improve diagnosis and at identifying the mechanisms of DILI should be supported. In the near future, it would be very helpful to develop an automatic real-time monitoring system to identify DILI and suggest culprit drugs when elevated LFT values are detected on EHR; artificial intelligence and deep learning technology support could be used for these purposes.
In conclusion, the results of our retrospective analysis of EHR in hospitalized Korean patients suggest that the incidence of DILI is 0.14%. Antibiotics were found to be the most common causative drugs, and the incidence of DILI per prescription patient was high for chemotherapeutic agents. We presented a potential diagnostic algorithm to detect DILI occurring during hospitalization. Further studies are needed to modify criteria for more accurate identification of DILI.
 XML Download
XML Download