

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anaphylaxis is a rapid and potentially fatal systemic response and is characterized by sudden degranulation of mast cells and basophils initiated by an immunological or non-immunological response.12 It is a relatively rare allergic disease, with a known prevalence ranging from 0.05% to 2%,3 and its causes, pathophysiology, and severity can vary greatly. Moreover, there are no biomarkers with which to guarantee a diagnosis of anaphylaxis. During anaphylaxis, the release of immunological mediators, such as histamine, tryptase, prostaglandin, and leukotriene, produce symptoms ranging from urticaria and angioedema at the mildest severity to dyspnea, loss of consciousness, and shock at the greatest severity. In result, patients can experience emotional stress leading to various mental diseases.4
Posttraumatic stress disorder (PTSD) is a psychiatric disorder with a reported lifetime prevalence of 6.8% in Americans.5 Its essential features comprise exposure to a traumatic event, re-experiencing the event, avoidance of stimuli reminding an individual of the trauma, and hyperarousal.6 One study reported that people who had suffered from anaphylactic shock could develop PTSD and other psychosocial dysfunctions.7 Since the trauma experienced during an anaphylaxis event can have a direct effect on the quality of life, investigating the psychological burden placed on patients with anaphylaxis is warranted.
PTSD has been found to exhibit relationships with diseases in which immune activation plays an important role, and some have speculated that alteration of inflammatory profiles, as observed in anaphylaxis, may contribute to the development of PTSD.891011 Various inflammatory mediators are involved in the pathogenesis of anaphylaxis.4 Tryptase, which is released from activated mast cells in severe anaphylaxis, is the most reliable biomarker of anaphylaxis.4 Tryptase has been shown to stimulate monocytes and eosinophils to produce interlukin (IL)-6, tumor necrosis factor (TNF)-α, and IL-1β.12 Among these, IL-6 is known to augment the acute phase response in inflammatory diseases, resulting in increasing C-reactive protein (CRP) levels.1314 Another study described increased platelet-activating factor (PAF) levels in patients with anaphylaxis.15 Interestingly, several studies have suggested that elevated levels of these inflammatory mediators are associated with PTSD.161718 Accordingly, we hypothesized that assessment of these mediators in patients with anaphylaxis would reveal links between them and psychiatric disorders, such as PTSD, anxiety, and depression.
In this study, we evaluated psychological distress (PTSD, anxiety, and depression) in patients with anaphylaxis using validated versions of related questionnaires translated in Korean and investigated relationships among inflammatory markers and distress severity.
Go to : 
MATERIALS AND METHODS
Subjects and data collection
A total of 203 adult patients with anaphylaxis (83 males and 120 females, mean age of 44 years) participated in this study. Patients who had been diagnosed with anaphylaxis in an emergency department or in an inpatient or outpatient setting were recruited. It was confirmed that all the patients in this study met the diagnostic criteria of anaphylaxis proposed by National Institute of Allergy and Infectious Diseases/Food Allergy and Anaphylaxis Network.19 For the follow-up, all patients visited an allergy outpatient clinic for 10 to 102 days after anaphylaxis, at which time blood sampling and psychiatric questionnaires were administered. No control subject was included in this study. Informed consent was obtained from each patient. This study received Institutional Review Board approval (MED-SUR-16-012).
Demographic characteristics, including age, sex, atopy, underlying diseases (allergic, psychological, or other medical diseases), prior anaphylaxis, causes of anaphylaxis, and the severity of anaphylaxis, were collected. Severe anaphylaxis was defined as the presence of hypotension, hypoxemia, collapse, loss of consciousness, or incontinence.2021 Information on the presence of any underlying psychiatric diseases was also acquired. Atopy was defined as at least 1 positive reaction to a skin prick test for 55 common inhalant allergens (Bencard Co., Brentford, UK), in which a positive reaction was defined as a ratio of the mean diameter of an allergen wheal greater than or equal to that of a histamine wheal. Administration of a systemic steroid or epinephrine was also recorded.
Korean versions of the Impact of Event Scale (IES-R-K)-Revised and other questionnaires
The IES-R-K, which is a modified Korean version of the IES-R, was used to detect PTSD.22 It is a self-rating questionnaire consisting of 22 questions designed to evaluate PTSD features, such as hyperarousal (feeling watchful and on guard), avoidance (an effort to avoid reminders of the trauma), and intrusion (dreams about the trauma). We categorized IES-R-K scores among the patients into three groups: normal (IES-R-K ≤ 24), wherein the risk of PTSD was low; mild-to-moderate (25 < IES-R-K ≤ 39); and severe (IES-R-K ≥ 40). The original cutoff points for the categorization of IES-R-K scores were 24, 39, and 60, allowing researchers to categorize subjects into one of four groups (≤ 24 = normal, 25-39 = mild/moderate, 40-59 = severe, ≥ 60 = very severe). However, as there were only 16 patients with an IES-R-K score over 60, we integrated the severe and very severe groups to maintain balance among groups.
For anxiety and depression, the Korean version of the Beck Anxiety Inventory (K-BAI) and the Beck Depression Inventory (K-BDI) were adopted. The K-BAI and K-BDI are self-rated questionnaires designed to evaluate anxiety and depression, respectively, both of which consist of 21 questions. Each of the questions is scaled from 0 to 3. Generally, a score of 22 or greater on K-BAI is considered to reflect the presence of anxiety symptoms, while a score of 17 or more on K-BDI is indicative of the presence of depressive symptoms.2324
Measurement of serum inflammatory markers in the recovery phase
Sera from all patients were collected at each participating hospital and sent to Ajou University Medical Center for the assessment of inflammatory markers. Serum tryptase (ThermoFisher Scientific, Uppsala, Sweden), IL-6 (R&D Systems, Minneapolis, MN, USA), TNF-α (Thermo Fisher Scientific), CRP (R&D Systems), and PAF (LifeSpan BioSciences, Seattle, WA, USA) levels were determined by enzyme-linked immunosorbent assay. All experiments were conducted in accordance with manufacturer guidelines for each product.
Statistical analysis
Statistical analyses were performed using SPSS 22.0. Student's t test or the Mann-Whitney U test was applied for the analysis of continuous variables. Discrete variables were analyzed by the χ2 test or Fischer's exact test. For comparisons among 3 groups, an analysis of variance test or Kruskal-Wallis test was adopted according to the normality of the data. The Wilcoxon signed rank test was performed to evaluate quantitative changes in variables at different time points. Simple correlation analysis was used for the determination of correlation between continuous variables. To identify factors predictive of PTSD, single and multiple logistic regression analyses were conducted. All P values less than 0.05 were considered statistically significant.
Go to :
RESULTS
Clinical characteristics of the study population
The study subjects comprised 83 (40.7%) males and 120 (59.3%) females (Table 1). Atopy was present in 69 (33.9%) patients. Among 88 (43.3%) patients with other allergic diseases, allergic rhinitis (80 patients, 39.6%) was the most common comorbid allergic condition, followed by food allergy (66 patients, 32.6%), atopic dermatitis (17 patients, 8.4%), asthma (13 patients, 6.4%), and chronic urticaria (11 patients, 5.4%). Underlying psychiatric diseases were noted in 6 (2.9%) patients. Drugs were the most common cause of anaphylaxis (114 patients, 56.1%), followed by food (52 patients, 25.6%), food-dependent exercise-induced anaphylaxis (16 patients, 7.8%), and bee stings (11 patients, 5.4%). Fifty-three patients (26.1%) had prior anaphylaxis events. More than half of the patients (110 patients, 54.2%) had severe anaphylaxis. Epinephrine and systemic steroids were administered in 61 (30.0%) and 63 (31.0%) patients, respectively. The mean time interval between an anaphylaxis event and administration of the questionnaires was 33.4 ± 19.6 days (range, 10-102 days).
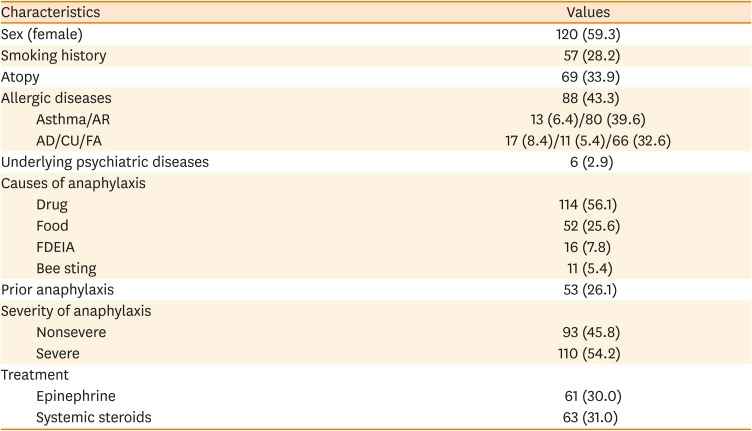
Table 1
Demographic, clinical, and psychiatric characteristics of the patients with anaphylaxis
Data are shown as number (%).
AR, allergic rhinitis; AD, atopic dermatitis; CU, chronic urticarial; FA, food allergy; FDEIA, food-dependent exercise-induced anaphylaxis.
![]()
Psychological burden posed by anaphylaxis
The mean IES-R-K score was 25.0 ± 20.5, and 84 (41.4%) patients had PTSD (IES-R-K ≥ 25). The mean K-BAI score was 13.1 ± 13.1, and 47 (23.2%) patients had anxiety (K-BAI ≥ 22). The average K-BDI score was 11.9 ± 9.7, and 57 (28.1%) patients had depression (K-BDI ≥ 17) (Fig. 1).
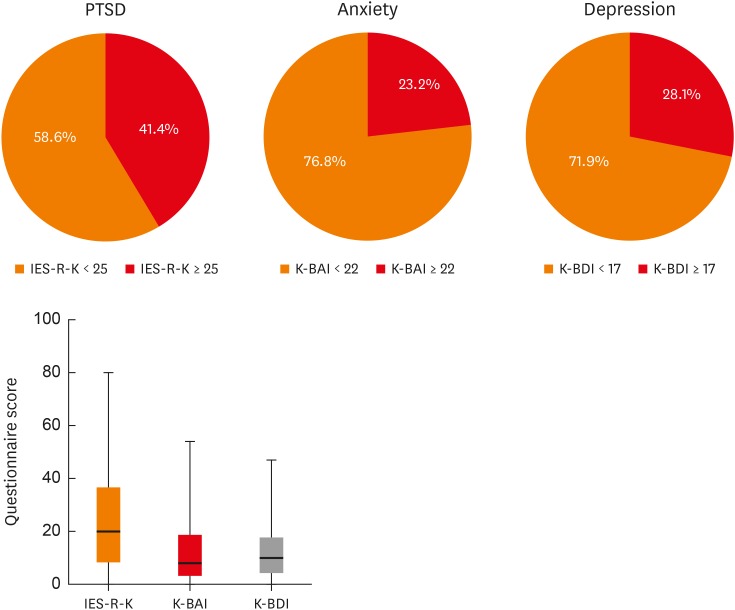 | Fig. 1Measurements of IES-R-K, K-BAI, and K-BDI and the proportion of patients who scored over the cut-off point of each questionnaire.PTSD, posttraumatic stress disorder; IES-R-K, the Impact of Event Scale-Revised-Korean version; K-BAI, Korean version of the Beck Anxiety Inventory; K-BDI, Korean version of the Beck Depression Inventory.
|
Defined according to IES-R-K scores, the normal, mild-to-moderate, and severe PTSD groups comprised 119, 37, and 47 patients, respectively (Table 2). The proportion of female patients was highest in the severe PTSD group, although the difference was not statistically significant (56.3%, normal; 51.4%, mild-to-moderate; 72.3%, severe; P = 0.095). The mean ages of each group were similar (43.2 ± 14.5 year-old, normal; 46.2 ± 14.1 year-old, mild-to-moderate; 44.3 ± 14.9 year-old, severe; P = 0.409). There were 1 (0.8%) and 5 (10.7%) patients who had psychological diseases in the normal and severe groups, respectively, whereas no patient had a psychological disease in the mild-to-moderate group (P = 0.009). A history of prior anaphylaxis showed no statistical significance among the three PTSD groups (27/93 patients, 29.0%, normal; 8/29 patients, 27.6%, mild-to-moderate; 18/36 patients, 50.0%, severe; P = 0.058), nor did the severity of anaphylaxis (P = 0.484).
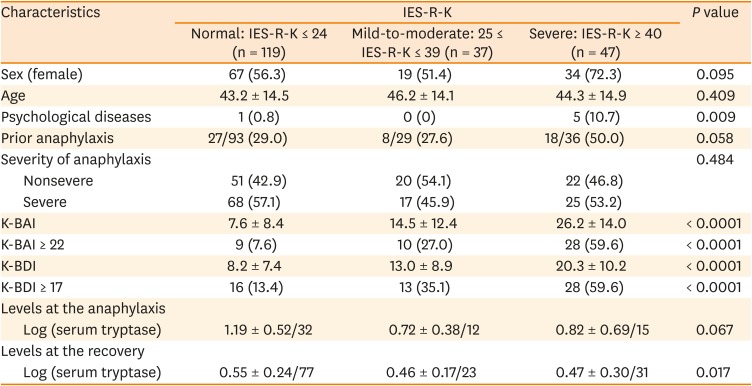
Table 2
Demographic, clinical, and psychiatric characteristics and serum tryptase levels of the patients with anaphylaxis according to IES-R-K
Data are shown as mean ± standard deviation or number (%).
IES-R-K, the Impact of Event Scale-Revised-Korean version; K-BAI, Korean version of the Beck Anxiety Inventory; K-BDI, Korean version of the Beck Depression Inventory.
![]()
K-BAI scores increased with more severe PTSD (7.6 ± 8.4, normal; 14.5 ± 12.4, mild-to-moderate; 26.2 ± 14.0, severe; P < 0.0001), as did K-BDI scores (8.2 ± 7.4, normal; 13.0 ± 8.9, mild-to-moderate; 20.3 ± 10.2, severe; P < 0.0001). Also increasing with more severe PTSD were the proportions of patients with anxiety (K-BAI ≥ 22) (9 patients, 7.6%, normal; 10 patients, 27.0%, mild-to-moderate; 28 patients, 59.6%, severe; P < 0.0001) and the proportions of patients with depression (K-BDI ≥ 17) (16 patients, 13.4%, normal; 13 patients, 35.1%, mild-to-moderate; 28 patients, 59.6%, severe; P < 0.0001).
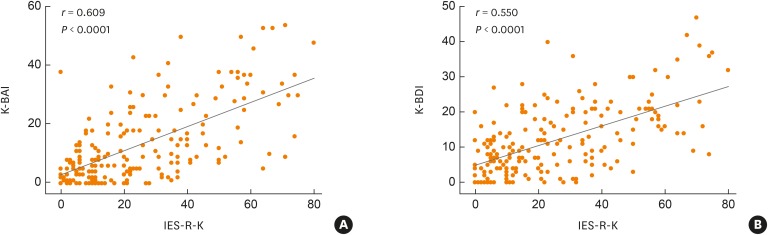
While log-transformed serum tryptase levels at the anaphylactic event were similar (1.19 ± 0.52, normal; 0.72 ± 0.38, mild-to-moderate; 0.82 ± 0.69, severe; P = 0.067), those after recovery from anaphylaxis were significantly higher in the normal group than in mild-to-moderate and severe groups (0.55 ± 0.24, normal; 0.46 ± 0.17, mild-to-moderate; 0.47 ± 0.30, severe; P = 0.017). Wilcoxon signed rank test indicated that serum tryptase levels significantly decreased during recovery, irrespective of IES-R-K score (P < 0.001). Meanwhile, IES-R-K scores in patients with anaphylaxis showed significant correlations with both K-BAI and K-BDI scores (r = 0.609, P < 0.0001 and r = 0.550, P < 0.0001, respectively) (Fig. 2).
Differences in serum inflammatory markers according to anaphylaxis severity and IES-R-K, K-BAI, and K-BDI scores
Various serum inflammatory markers were compared in the present study (Table 3). None of the inflammatory markers, including serum tryptase, IL-6, TNF-α, CRP, and PAF, differed between the mild-to-moderate and severe anaphylaxis groups (tryptase, 3.6 ± 2.1 ng/mL vs. 3.5 ± 2.7 ng/mL, P = 0.741; IL-6, 5.3 ± 11.0 pg/mL vs. 9.3 ± 25.2 pg/mL, P = 0.223; TNF-α, 0.8 ± 4.1 pg/mL vs. 1.4 ± 7.7 pg/mL, P = 0.594; CRP, 1.1 ± 0.8 µg/mL vs. 1.2 ± 0.9 µg/mL, P = 0.636; PAF, 4.5 ± 3.2 ng/mL vs. 4.4 ± 3.2 ng/mL, P = 0.868). None of these markers, except for serum tryptase, showed significant differences when dichotomized according to an IES-R-K score < or ≥ 25 (tryptase, 3.2 ± 2.5 ng/mL vs. 3.8 ± 2.4 ng/mL, respectively, P = 0.050; serum IL-6, 8.2 ± 20.8 pg/mL vs. 6.9 ± 19.2 pg/mL, P = 0.434; serum TNF-α, 1.1 ± 4.8 pg/mL vs. 1.1 ± 7.1 pg/mL, P = 0.797; serum CRP, 1.0 ± 0.8 µg/mL vs. 1.2 ± 0.9 µg/mL, P = 0.338; serum PAF, 4.0 ± 3.0 ng/mL vs. 4.8 ± 3.3 ng/mL, P = 0.156). Only serum PAF levels exhibited significant differences between patients grouped according to K-BAI scores ≥ 22 or < 22 (3.6 ± 3.0 ng/mL vs. 4.8 ± 3.2 ng/mL, respectively, P = 0.045) and between those grouped according to K-BDI scores ≥ 17 or < 17 (PAF, 3.5 ± 2.8 ng/mL vs. 4.9 ± 3.3 ng/mL, respectively, P = 0.028).

Table 3
Differences of serum inflammatory mediators measured at the recovery phase according to the severity of anaphylaxis and the cut-off values of psychiatric questionnaires (IES-R-K, K-BAI, and K-BDI)
IES-R-K, the Impact of Event Scale-Revised-Korean version; K-BAI, Korean version of the Beck Anxiety Inventory; K-BDI, Korean version of the Beck Depression Inventory; IL-6, interlukin-6; TNF-α, tumor necrosis factor-α; CRP, C-reactive protein; PAF, platelet-activating factor.
![]()
Predictors of PTSD severity
Univariate and multivariate logistic regression analyses were performed to identify predictors for PTSD (Table 4). The variables included demographic and clinical characteristics (female sex, prior anaphylaxis, causes of anaphylaxis, and severe anaphylaxis), as well as K-BAI and K-BDI scores (K-BAI ≥ 22 and K-BDI ≥ 17). In the univariate analysis, only K-BAI and K-BDI scores were predictors for PTSD (odds ration [OR], 10.10; 95% confidence interval [CI], 4.52-22.56; P < 0.0001, K-BAI ≥ 22; OR, 6.14; 95% CI, 3.11-12.10; P < 0.001, K-BDI ≥ 17). Multivariate analysis showed a K-BAI score of 22 or more as the most significant variable (OR, 6.15; 95% CI, 2.37–15.95; P < 0.0001), followed by a K-BDI score of 17 or more (OR, 2.63; 95% CI, 1.09–6.38; P = 0.032).
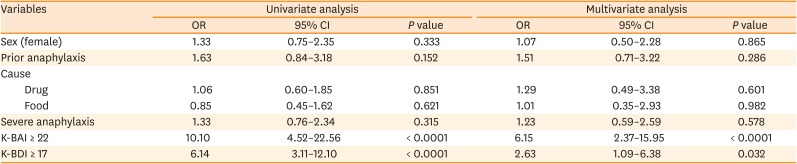
Table 4
Results of the univariate and multivariate logistic regression analyses for the presence of posttraumatic stress disorder
OR, odds ratio; CI, confidence interval; K-BAI, Korean version of the Beck Anxiety Inventory; K-BDI, Korean version of the Beck Depression Inventory.
![]()
Go to :
DISCUSSION
This is the first multicenter study to investigate the relationships between anaphylaxis and psychological distress in Korea. Our results indicated that patients who experienced anaphylaxis were likely to develop psychiatric disorders, such as PTSD, anxiety, and depression. Among all 203 patients with anaphylaxis in this study, 84 (41.4%) had PTSD, and the development of PTSD did not appear to depend on the severity of anaphylaxis, although patients with higher IES-R-K scores had more severe anxiety and depression. While serum tryptase levels during anaphylaxis did not differ according to PTSD status, serum PAF levels were lower in patients with anxiety and depression during recovery from anaphylaxis. Anxiety and depression were identified as predictors of PTSD in patients who had recently experienced anaphylaxis.
Generally, the diagnosis of psychiatric diseases is established by psychiatrists using the Diagnostic and Statistical Manual of Mental Disorders. However, IES-R-K is commonly used by researchers to evaluate the presence of PTSD in Korea, since not all patients with possible PTSD visit a psychiatric specialist. In a previous study, the reliability and validity of the IES-R-K were deemed satisfactory as an instrument for PTSD assessment in Korea.25
Serum tryptase is considered a reliable marker of anaphylaxis and is widely used for the diagnosis of anaphylaxis.26 In the current study, the mean serum tryptase level during anaphylaxis was 24.7 ng/mL, and serum tryptase levels during anaphylaxis above the known cutoff value of anaphylaxis (11.4 ng/mL) were only present in 44.1% of patients.27 Also, we discovered that serum tryptase levels neither during anaphylaxis nor during recovery were correlated with the severity of anaphylaxis (P = 0.827 and P = 0.973, respectively). While baseline serum tryptase levels have been proposed as a possible biomarker for risk prediction of anaphylaxis,27 their ability to reflect the severity of anaphylaxis appears to be limited.
In this study, we found serum PAF levels to be lower in patients with anxiety and depression than in those without these conditions after an anaphylactic event. Secreted by multiple sources, including mast cells, monocytes, and macrophages, PAF is a proinflammatory phospholipid important in platelet activation, and more than 99% of serotonin, which plays an important role in mediating positive affect and mood, is found among dense platelet granules.28 Nevertheless, while there are numerous studies on the relationship between platelet activation and depression, it remains unclear whether the development of depression is attributable to increased or decreased platelet activation.293031 Moreover, many factors other than PAF are thought to affect platelet activation. As the contributions of PAF to anxiety and depression in relation to platelet activation have undergone little research, further studies are warranted, employing tests of platelet aggregation or analyses of surface markers (P-selectin or activated glycoprotein IIb/IIIa) of and secreted chemicals (platelet factor 4 or β-thromboglobulin) from activated platelets.
Many psychiatric disorders are related to each other. In the present study, K-BAI and K-BDI showed incremental correlations with IES-R-K. Moreover, anxiety and depression were identified as the most reliable predictors for PTSD. Indeed, studies have shown PTSD to be accompanied by anxiety and depressive disorders after stressful events.3233 Some have attempted to document genetic features connecting PTSD to other stress-related psychiatric disorders.34 Nevertheless, it is still unclear how psychiatric disorders exactly affect one another, and robust studies of the relationships among stress-related psychiatric disorders are needed, particularly in adults with anaphylaxis; while there are studies regarding anxiety and depression in children, their parents, or young adults with anaphylaxis, research in these areas on adult patients with anaphylaxis is scarce.3536
There are several limitations in this study. First, clinical data on anaphylactic events were collected retrospectively. Since we planned to register the study participants when they visited for follow-up after anaphylaxis, we cannot exclude the possibility of selection bias. In addition, we were not able to compare our results with those in healthy controls. The second limitation is in relation to the timing of measurements of inflammatory markers. Except for serum tryptase, all inflammatory markers were measured only during the recovery phase of anaphylaxis, which was 102 days after the anaphylactic event at its latest. Moreover, the length of time until follow-up visit in each patient varied. As PAF has a very short half-life of 3 to 13 minutes,15 the results thereon as well as the other inflammatory markers might have differed if we had been able to measure it during the anaphylaxis. Despite these limitations, this study provides reliable information on psychological distress in patients with anaphylaxis. We prospectively evaluated the patients with questionnaires that were unified and reproducible, and the prevalence of psychiatric disorders in the anaphylaxis patients was remarkably higher than that reported in general populations.
In conclusion, we found that patients with anaphylaxis are prone to develop psychiatric disorders such as PTSD, anxiety, and depression. Accordingly, we suggest that the general management of anaphylaxis ought to include psychiatric evaluation.
Go to :
 XML Download
XML Download