

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of asthma in older adults ranges from 6% to 10%,1 but it is often difficult for them to achieve asthma control compared to younger asthmatics.2 With the increasing numbers of older people, proper management of older asthmatics has become an emerging concern. Aging is associated with decline in small airway diameters at the age of ≥ 40 years, contributing to a decrease in expiratory flow rate.3 Age-related structural changes of the respiratory system results in an increase in closing volume, subsequently increasing the risk for small airway dysfunction.45 It has been demonstrated that aging and asthma duration are risk factors for poorly controlled asthma, contributing to changes in small airways in older patients with asthma.6
The Global Initiative for Asthma (GINA) guidelines recommend a combination of inhaled corticosteroids (ICSs) and long-acting β2 agonists (LABAs) for the treatment of patients with moderate-to-severe asthma. Current inhaler devices available for ICS-LABA combination therapy include pressurized metered-dose inhalers (p-MDI) and dry powder inhalers (DPI). While p-MDI requires coordination between inhalation and device activation, DPI relies only on the subject's rapid and forcible inhalation.7 DPI is suitable for those who are able to generate sufficient inspiratory airflow in order to activate the medication; however, which makes this inhaler inappropriate for older patients and those with severe airflow limitation.8 The desirable aerosol size and spray impact force of p-MDI lead to increases in total lung deposition and peripheral airway penetration, which would be beneficial for older patients with longer duration of asthma, since small airways are important sites of inflammation.9101112
Previous studies have shown that improper inhaler technique is associated with poorly controlled asthma and frequent asthma exacerbation.1314 The effectiveness of inhaler devices is often compromised by incorrect inhaler technique and poor adherence that results in inadequate drug delivery to the lungs.1516 Both of the devices p-MDI and DPI, used in this study have been shown to be effective in a controlled setting with patients educated on how to correctly use them.17
There have been few studies investigating whether p-MDI treatment was effective in older patients with a longer duration of asthma. The aim of this study was to examine the efficacy and safety of 2 devices of combination inhalers, fluticasone propionate/formoterol fumarate (FP/FOR) treatment using a p-MDI (p-MDI group) and fluticasone propionate/salmeterol xinafoate (FP/SAL) treatment using a DPI (DPI group) in older asthmatics for 12 weeks after training the study subjects for the correct use of their study inhalers.
MATERIALS AND METHODS
Subjects
The subjects aged over 55 years, with a diagnosis of asthma more than 6 months before the enrollment in the study based on clinical symptoms (such as cough, dyspnea, chest tightness and wheezing), airway reversibility (an increase in forced expiratory volume in 1 second [FEV1] ≥ 12% and 200 mL from pre-bronchodilator use), and airway hyper-responsiveness (provocative concentration of methacholine that results in a 20% drop in FEV1 < 16 mg/mL of methacholine). Their current treatment was a combination therapy of inhaled ICS (budesonide 400 µg/day or equivalent) and LABA for over 30 days before participating in this study. Asthma symptom control was assessed according to the GINA guidelines.18
For this study, the patients were required to have normal results on complete blood count, routine chemistry, urinalysis, and electrocardiogram at screening. We recruited subjects who completely understood the purpose and content of the study, agreed to voluntarily participate in the study, and provided written consent. This study protocol was approved by the Institutional Review Board of our hospital (AJIRB-MED-CT4-15-420).
We excluded the patients who 1) had well-controlled asthma after a 4-week run-in period; 2) had other acute diseases within 30 days before administration of trial medications; 3) had a smoking history of more than 30 pack-years; 4) had a history of hypersensitivity to ICSs; and 5) were prescribed any medications influencing asthma control, such as immunomodulatory drugs (omalizumab, cyclosporine, etc.) or systemic steroids due to diseases other than asthma.
Study design
This was an open-labeled, randomized, prospective trial involving male and female outpatients over 55 years old. It aimed to establish the non-inferiority of the p-MDI group compared to the DPI group in terms of efficacy and safety in patients with uncontrolled asthma. Eligible subjects were recruited between March 2016 and February 2018 from Ajou University Hospital in Suwon, Korea. Before randomization, patients entered a 4-week run-in period and then they used a combination of inhaled ICS-LABA. At the end of the run-in period, subjects meeting the criteria GINA-defined “partly controlled asthma” or “uncontrolled asthma” were finally enrolled. The study subjects’ diaries to check for the administration of drugs, daytime and nighttime symptoms, and use of rescue medications were collected every 4 weeks during the study period.
The subjects were stratified according to the duration of asthma (longer [over 15 years] or shorter duration of asthma [less than 15 years]) (Fig. 1). They were randomly assigned to receive either FP/FOR-p-MDI or FP/SAL-DPI for a 12-week study period. Randomization was performed according to a balanced block design with a centrally generated randomization code.
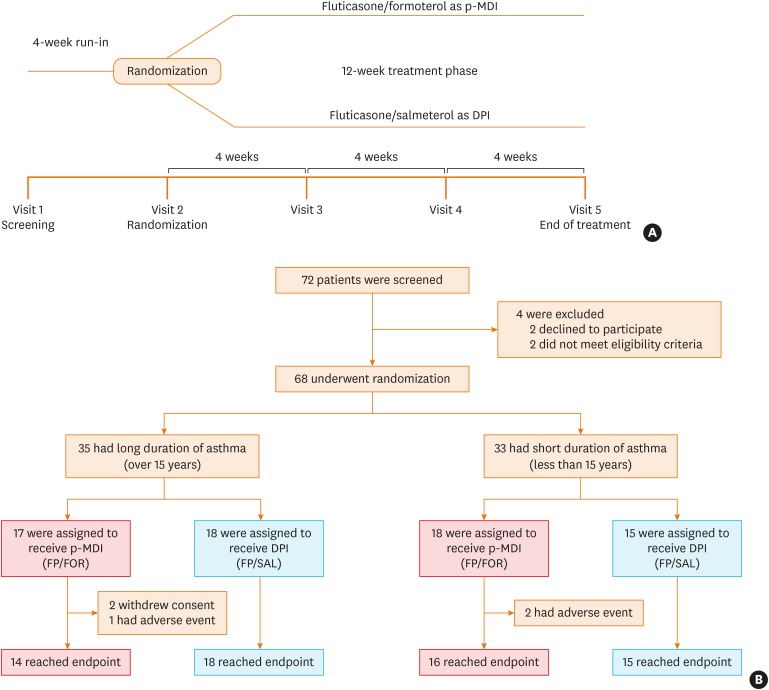
Fig. 1
Trial design and CONSORT flow.
(A) shows the design of the trial and (B) shows the screening, randomization, and treatment for patients stratified according to asthma duration (≥ 15 years or < 15 years). All patients who underwent randomization into the treatment method were included in the full analysis set population.
CONSORT, Consolidated Standards Of Reporting Trials; p-MDI, pressurized metered-dose inhalers; FP/FOR, fluticasone propionate/formoterol fumarate; DPI, dry powder inhalers; FP/SAL, fluticasone propionate/salmeterol xinafoate.
![]()
Endpoints and assessments
The primary endpoint was the proportion of subjects reaching well-controlled asthma after the 12-week study period based on the GINA guidelines. Primary endpoints were also assessed in pre-specified subgroups according to the duration of asthma (≥15 years or <15 years) and the residual volume (RV) to total lung capacity (TLC) ratio (≥ 45% or < 45%). Secondary endpoints included the changes in lung function parameters (airway obstruction evaluated by spirometry and air trapping evaluated by body plethysmography), fractional exhaled nitric oxide (FeNO) levels, asthma control test (ACT) scores, the proportion of subjects with exacerbation (worsening of asthma leading to systemic glucocorticoid treatment for ≥ 3 days, hospitalization, or an emergency department visit leading to systemic glucocorticoid treatment), inhalation technique, and adherence to the treatment. All the subjects were educated to properly use inhalers at each visit. Patients' inhaler technique was assessed by investigators using specific check lists for each type of study inhalers (Supplementary Table S1). The check list for each device consisted of 9 steps on a 0-to-3 score scale at each step. Total inhaler technique scores were calculated from the sum of the 9-step scores. Adherence was assessed from the dose counter values of each patient who returned their study devices based on the number of days. If the patients used the devices 2 times a day on average during the study period, which means 100% adherence. Adherence was assessed between baseline and week 12 visits.19
Safety was monitored at each visit by asking all the subjects whether they had had any adverse events during the study period. We obtained information on local adverse reactions including voice changes, oral thrush, sore throat, laryngeal discomfort and paroxysmal cough immediately after the inhalation, during the study period using patients’ questionnaires and clinical examinations at each visit.
Statistical analysis
The study was designed to evaluate the non-inferiority of the p-MDI group compared to the DPI group, and 63 patients were analyzed by the non-inferiority test. The difference in the proportion of reaching well-controlled asthma between the p-MDI group and the DPI group was examined as the primary endpoint at the end of the study period, and non-inferiority margin was set at 17.0%.202122 We applied the per-protocol principle to assess non-inferiority for the primary endpoint to reduce possible statistical biases caused by missing data imputation. Non-inferiority was concluded if the lower limit of the unilateral 95% confidence interval (CI) of the difference in the proportion of patients with well-controlled asthma between the p-MDI and DPI groups was greater than the non-inferiority margin (−17.0%).
Baseline characteristics were compared using the Mann-Whitney U test for continuous variables and the χ2 test for categorical variables. Secondary outcome analyses were performed in the full analysis set population, which included all the subjects who underwent randomization. Lung function parameters and ACT scores were analyzed with a linear mixed model. The t test or Mann-Whitney U test was used to analyze inhaler technique and adherence over the 12-week study period. The changes in lung parameters and inhaler technique scores from baseline at each time were compared using the paired t test or Wilcoxon-signed rank test. The categorical variables, such as FeNO and asthma exacerbation, were analyzed by the χ2 test. The number of adverse events were analyzed by Fisher's exact test.
RESULTS
Clinical characteristics of the study subjects
A total of 72 patients were recruited and entered the run-in period. Of these, 4 could not be randomized because they did not fulfill the eligibility criteria and declined to participate. The 68 eligible patients were randomized into the 2 treatment groups (35 into the p-MDI group and 33 into the DPI group). Of these, 5 were withdrawn after randomization (5 from the p-MDI group and 0 from the DPI group) because of adverse events occurred (n = 3) or consent was withdrawn (n = 2). Finally, 30 patients in the p-MDI group and 33 in the DPI group completed the study. The baseline demographics and clinical characteristics were not different between the 2 groups (Table 1).
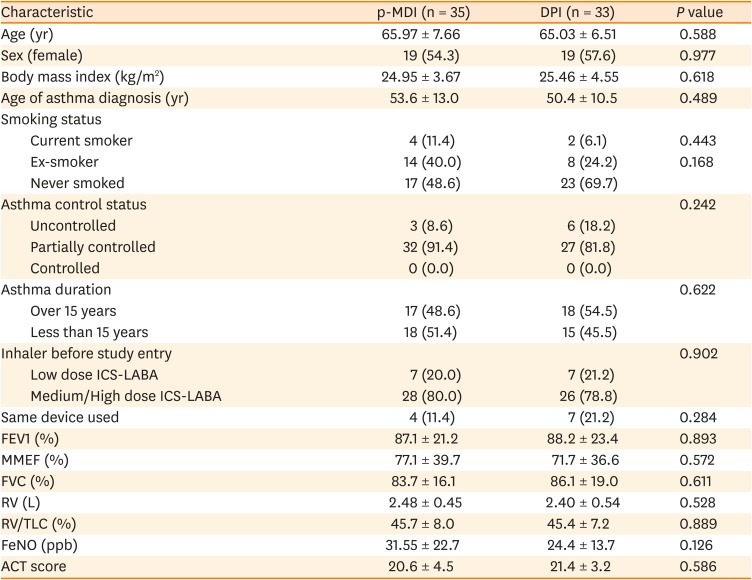
Table 1
Clinical demographic and clinical characteristics of the study subjects in the full analysis set population
The full analysis set population included all the patients who underwent randomization. P values were obtained from the Mann-Whitney U test for continuous variables and the χ2 test for categorical variables. Plus-minus values are mean ± standard deviation.
p-MDI, pressurized metered-dose inhalers; DPI, dry powder inhalers; ICS, inhaled corticosteroid; LABA, long-acting β2 agonist; FEV1, forced expiratory volume in 1 second; MMEF, maximal mid-expiratory flow; FVC, forced vital capacity; RV, residual volume; RV/TLC, residual volume/total lung capacity ratio; FeNO, fractional exhaled nitric oxide; ACT, asthma control test.
![]()
Primary efficacy endpoint
There were no significant differences in the rates of well-controlled asthma between the p-MDI and DPI groups in week 4 (40.0% vs. 33.3%), week 8 (56.7% vs. 36.4%) and week 12 (53.3% vs. 45.5%) (Fig. 2). Both groups reached a plateau in asthma symptom control compared to baseline after the first 4 weeks of treatment. Non-inferiority of the p-MDI group in reaching well-controlled asthma was met after 8 weeks of treatment (difference 18.2%; 95% CI −5.8% to 42.2% in week 8, difference 7.9%; 95% Cl −16.8% to 32.6% in week 12). The lower limit of 95% CI was above −17.0%, which was the predefined margin for the non-inferiority in weeks 8 and 12 (P = 0.002 and P = 0.024, respectively).
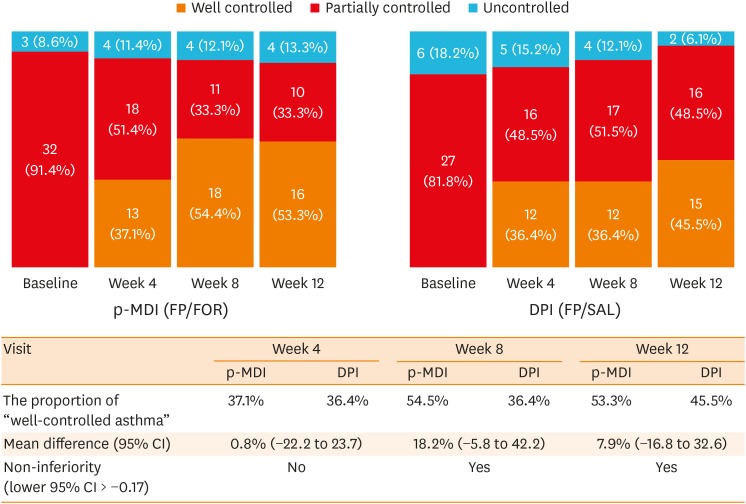
Fig. 2
The proportion of asthma control status in the p-MDI and DPI groups during the study period.
Asthma control status was assessed according to the GINA guidelines. The proportion test (one-sided) for proving non-inferiority of the FP/FOR group and the FP/SAL group in the PP population, with a predetermined non-inferiority margin of −17.0% for the difference in the rates of well-controlled asthma between the 2 groups. PP principle was applied to reduce possible statistical bias caused by missing data imputation.
p-MDI, pressurized metered-dose inhalers; FP/FOR, fluticasone propionate/formoterol fumarate; DPI, dry powder inhalers; FP/SAL, fluticasone propionate/salmeterol xinafoate; GINA, Global Initiative for Asthma; PP, per-protocol; CI, confidence interval.
![]()
Secondary efficacy endpoint
The relative risk (RR) of the proportion of not well-controlled asthma at the 12-week treatment was 0.86 (95% CI, 0.52–1.40) in the p-MDI group compared to the DPI group in the pre-protocol population (63 patients) (Fig. 3). Among patients with a longer duration of asthma (≥ 15 years), the rate of not well-controlled asthma was 0.43 in the p-MDI group and 0.56 in the DPI group (RR was 0.77 in the p-MDI group compared to the DPI group [95% CI, 0.37–1.61]). Among patients with a shorter duration of asthma (< 15 years), the rate of not well-controlled asthma was 0.50 in the p-MDI group and 0.53 in the DPI group (RR of the p-MDI group compared to the DPI group was 0.94 [95% CI, 0.47–1.85]). In addition, among patients with higher air trapping (RV/TLC ≥ 45%), the rate of not well-controlled asthma was 0.63 in the p-MDI group and 0.80 in the DPI group (RR of the p-MDI group compared to the DPI group was 0.78 [95% CI, 0.50–1.23]). Among patients with lower air trapping (RV/TLC < 45%), the rate of not well-controlled asthma was 0.29 in the p-MDI group and 0.33 in the DPI group (RR of the p-MDI group compared to the DPI group was 0.86 [95% CI, 0.30–2.46]). Lung physiology variables, including FEV1 (%), maximal mid-expiratory flow (MMEF) (%), forced vital capacity (FVC) (%), RV (L), RV/TLC (%), and FeNO (ppb), were not statistically different between the 2 treatment groups in week 12 (Table 2). The increases in predicted FEV1 (%) from baseline at the end of the study were 0.3% in the p-MDI group and 2.0% in the DPI group, although the difference was statistically insignificant. Mean baseline ACT scores were not significantly different between the 2 groups (20.6 vs. 21.4, P = 0.586). During the study period, there were no significant differences in mean ACT scores between the p-MDI and DPI groups (20.3 vs. 21.4 in week 4, 20.0 vs. 21.4 in week 8, and 20.7 vs. 22.0 in week 12, respectively). The proportion of patients without asthma exacerbations was 68.6% in the p-MDI group and 78.8% in the DPI group during the 12 weeks’ study period, with no significant differences (P = 0.340). The number of patients with asthma exacerbations resulting in hospitalization or an emergency department visit during the 12-week treatment was 1 (2.9%) in the p-MDI group and 1 (3.0%) in the DPI group.
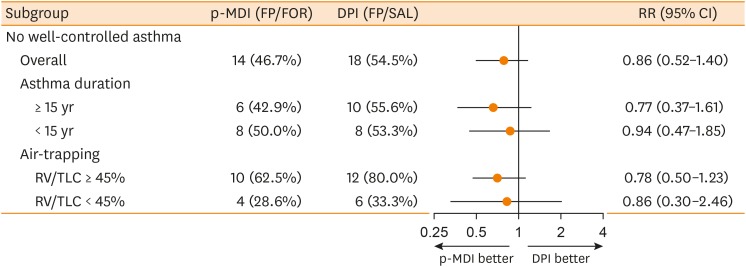
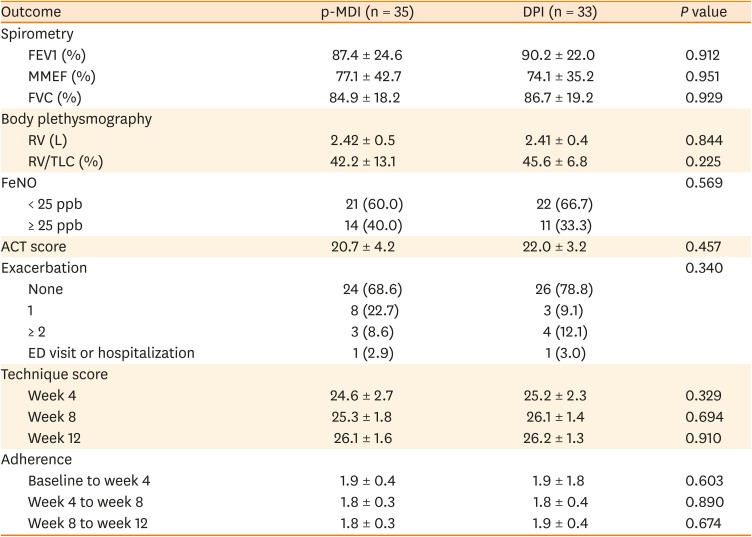
Fig. 3
Subgroup analyses of the risk of “partly controlled asthma” or “uncontrolled asthma” according to baseline asthma duration and baseline air trapping.
The subgroup analyses were evaluated in the per-protocol population to reduce possible statistical biases caused by missing data imputation.
p-MDI, pressurized metered dose inhalers; FP/FOR, fluticasone propionate/formoterol fumarate; DPI, dry powder inhalers; FP/SAL, fluticasone propionate/salmeterol xinafoate; RR, relative risk; CI, confidence interval; RV/TLC, residual volume/total lung capacity.
![]()
Table 2
Secondary outcome results in the full analysis set population
The full analysis set population included all randomized patients. Inhaler technique was calculated from the sum of checklist scores. Adherence was assessed from dose counter values of each patient who returned their study devices with taking into account the number of days. Lung function parameters and ACT score were analyzed with linear mixed model. P values were obtained from the Mann-Whitney U test for continuous variables and the χ2 test for categorical variables. Plus-minus values are mean ± standard deviation.
p-MDI, pressurized metered-dose inhalers; DPI, dry powder inhalers; FEV1, forced expiratory volume in 1 second; MMEF, maximal mid-expiratory flow; FVC, forced vital capacity; RV, residual volume; RV/TLC, residual volume/total lung capacity ratio; FeNO, fractional exhaled nitric oxide; ACT, asthma control test; ED, emergency department.
![]()
Inhaler technique and adherence
Inhaler technique scores at baseline before instruction were lower in both groups (18.43 in the p-MDI group and 20.3 in the DPI group). They significantly increased after inhaler use education during the 12-week study period in the p-MDI and DPI groups, although the difference was not significant (24.6 vs. 25.2 in week 4, 25.3 vs. 26.1 in week 8, and 26.1 vs. 26.2 in week 12, respectively) (Fig. 4). During the study period, no significant differences were observed in inhaler adherence between the p-MDI and DPI groups (1.9 vs. 1.9 in week 4, 1.8 vs. 1.8 in week 8, and 1.8 vs 1.9 in week 12, respectively). Both groups were found to have good inhaler adherence after instruction during the study period.
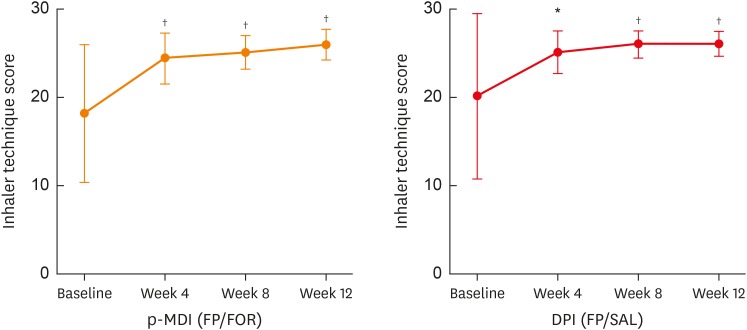
Fig. 4
Changes in total inhaler technique scores from baseline to week 12.
Inhaler technique scores were calculated from the sum of checklist scores. The P values shown refer to change from baseline using the paired t-test or Wilcoxon signed rank test.
p-MDI, pressurized metered-dose inhalers; FP/FOR, fluticasone propionate/formoterol fumarate; DPI, dry powder inhalers; FP/SAL, fluticasone propionate/salmeterol xinafoate.
*P < 0.01 and †P < 0.001. I bars represent 95% confidence intervals.
![]()
Safety
The number of patients who had experienced at least 1 adverse event during the 12-week study period was not different between the p-MDI and DPI groups (12 [34.3%] vs. 9 [27.3%]) (Table 3). The most frequently reported adverse events were nasopharyngitis (8.6% in the p-MDI group and 6.1% in the DPI group) and bronchitis (5.7% in the p-MDI group and 6.1% in the DPI group). Details of adverse events were similar in the 2 groups, and there were no clinically significant serious adverse events. However, cases of voice changes associated with inhalers were more frequently observed in the p-MDI group than in the DPI group (3 and 0 patients, respectively). In the p-MDI group, 3 patients discontinued the treatment because of adverse events; 2 patients had asthma exacerbation for more than 2 weeks and 1 had voice changes associated with inhaler use.
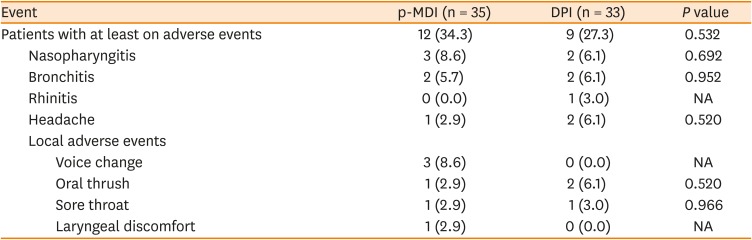
Table 3
Treatment-related adverse events reported during 12 weeks of treatment
Safety analyses included all the patients who underwent randomization. The number (%) of patients with treatment-related adverse events was reported during the study period. P values were obtained from Fisher's exact test.
p-MDI, pressurized metered-dose inhalers; DPI, dry powder inhalers; NA, not applicable.
![]()
DISCUSSION
To the best of our knowledge, this is the first randomized trial performed in older patients with moderate-to-severe asthma, in terms of the effects of ICS-LABA combination therapy using a p-MDI compared to that using a DPI. The present study showed that p-MDI was non-inferior to DPI with regard to the proportion of well-controlled asthma over a 12-week study period. Regardless of the type of inhaler devices, similar inhaler technique and inhaler adherence were observed; the efficacy and safety of p-MDI and DPI were not different in the management of older asthmatics. The results of the present study are consistent with those of previous studies demonstrating that p-MDI has comparable efficacy to DPI in patients with asthma, in which changes in FEV1 values from baseline and the risk of exacerbations were measured as primary endpoint.222324 However, most of these studies were performed on younger adults with asthma, while our trial was conducted on older asthmatics (over 55 years old).
The present study demonstrated that asthma control in older asthmatics was achieved in 53.3% of the p-MDI group patients and 45.5% of the DPI group patients over a 12-week study period, which was similar to the result of a previous study performed on patients at all ages including younger adults.21 In addition, when we educated the patients about inhaler technique to the study subjects at each visit, inhaler technique scores and adherence increased significantly in both treatment groups, which could improve clinical efficacy. These findings support that ICS-LABA maintenance therapy with proper use of inhaler devices can be expected to improve asthma symptoms in older asthmatics as well as in younger ones. On the other hand, significant improvements from baseline in lung function parameters were reported in most of the previous studies, which was not found in the present study, suggesting that decreased airway β2-adrenoceptor responsiveness and airway remodeling may occur in older asthmatics, especially in those with a longer duration.
It is known that elderly asthmatics have poorer clinical outcomes as they suffer from comorbid conditions and respond less to conventional anti-asthmatic medications including ICS-LABA1; therefore, older asthmatics with a longer duration tend to increase the severity of asthma, making the disease more difficult-to-treat.25 Several studies have shown that aging and asthma duration are related to small airway dysfunction.526272829 A recent study demonstrated that functional abnormalities in the small airways increase with age by about 2% per decade after the age of 50 years as assessed in computed tomography (CT) analysis even in never-smokers with normal lung function.30 In a cohort of elderly lifetime nonsmokers with asthma, subjects with a longer asthma duration displayed more severe airflow limitation as compared to those with a shorter duration, which suggested that long-standing asthma is also involved in small airway remodeling.31 In addition, recent studies combined 3-D radionuclide imaging with CT scanning to better interpret the deposition location of aerosol in the respiratory tract, showing that the total lung delivery by using a p-MDI is approximately twice that by using a DPI.911 Based on these findings, we hypothesized that use of p-MDI would be beneficial for older asthmatics, particularly in patients with small airway dysfunction, by increasing peripheral lung deposition. In the present study, there were no significant differences in primary and secondary outcomes between the 2 treatment groups and between the pre-specified subgroups. Our trial has limitations in evaluating the effects of p-MDI according to the presence of small airway dysfunction. However, there were trends toward a lower risk of not well-controlled asthma in older asthmatics with a longer asthma duration and higher air trapping levels in the p-MDI group compared to the DPI group. Further studies are required to demonstrate the potential advantages of p-MDI in older asthmatics affecting peripheral lung deposition.
In older patients with asthma, it has been shown that p-MDI is more difficult to maintain a good inhalation technique compared to DPI. Previous studies have shown that older asthmatics are at higher risk of improper use of p-MDI resulting in poor asthma control.3233 The present study demonstrated that older asthmatics in the p-MDI group have similar inhaler technique and adherence with a comparable effectiveness as compared to those in the DPI group. Also, this study evidenced that older asthmatics can be educated to achieve better inhaler technique using a p-MDI as well as DPI. The 2 most common types of inhalers, p-MDI and DPI, have distinct strengths and weaknesses. In choosing inhaler devices for asthmatics, the clinician must take into account several factors, including the cognitive and physical ability of the patients, ease of use, convenience, costs, and patient preference.34 Our findings suggest that p-MDI can be a good treatment option in older asthmatics. In a real-life clinical setting, improper inhaler technique and non-adherence to inhalers are common in older asthmatics. Specific factors for inappropriate inhaler use in older asthmatics are learning difficulties from impaired cognitive function as well as impaired vision and fine motor skills. Adherence is also an important issue in older asthmatics for achieving asthma control. Several factors, such as poor knowledge about the treatment, the disease or its consequences, can cause patients to intentionally decide not to maintain the treatment. Furthermore, patients with asthma may be prescribed various inhalers, which is associated with increased inhaler use errors and poor adherence. Thus, inhaler technique/adherence should be revised before making a change in the treatment plan of patients with uncontrolled asthma. Evaluating inhalation technique and repeated education about correct usage and good adherence to inhalers are essential for regular monitoring.
The regular use of ICSs raises concern about local adverse events such as oral thrush, sore throat, and voice changes. Many trials estimated adverse events at approximately 5% to 60% of treated patients, which may have a deleterious effect on compliance.35 In the present study, 6 patients in the p-MDI group and 3 patients in the DPI groups had local adverse events associated with ICSs, leading to discontinuation of the trial medications only in p-MDI group. Although these events occurred slightly more frequently in the p-MDI group, the overall number of patients with adverse events was not significantly different between the 2 treatment groups, suggesting that safety is not important for choosing inhaler types in older asthmatics.
There are several limitations to this study. First, the potential for investigator bias could not be completely excluded. Because evaluating asthma control status by the GINA guidelines depends on patients' recall of asthma symptoms, recall bias in older asthmatics may affect the results of this study. Secondly, the 12-week follow-up period might be insufficient to evaluate the effect of asthma control status and other outcome parameters. Longer follow-up studies are required to confirm our results. Thirdly, the present study was conducted at a single tertiary medical center in South Korea, and the number of subjects was relatively not large enough. Older patients are not willing to participate in clinical trials as compared to younger subjects. Moreover, it was difficult to recruit older patients because of coexistent chronic diseases, cognitive impairment, and polypharmacy. Future studies with a larger cohort of ethnically diverse populations of older asthmatics are needed to demonstrate the clinical importance of our findings.
In conclusion, the results of this study showed that p-MDI was non-inferior to DPI in GINA-guided asthma control over a 12-week treatment period, suggesting that p-MDI can be an effective treatment option for older patients with uncontrolled asthma, particularly in those with longer disease duration and higher air trapping.
 XML Download
XML Download