

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma, the most common chronic disease of childhood,1 is characterized by the presence of reversible airway obstruction. Compared to asthma in children and young adults, asthma in the elderly (EA; ≥65 years old) is more complex due to comorbidities and aging-related changes, and this ambivalence has often led to the heterogeneous clinical phenotypes. EA is increasing with an aging society, adding a heavy socioeconomic burden to the healthcare system.2 EA patients have higher medical demands and poorer outcomes than younger patients due to frequent exacerbation and hospitalization.34 With the recent paradigm shift based on health behavior, population-tailored treatment options for asthma are recommended to achieve optimal control of the disease symptoms.5 However, there are virtually no large-scale cohort studies on the diagnosis, pathophysiology, and treatment of the EA group.6
There are even more critical issues associated with asthma exacerbation of EA. A nationwide study showed that patients with asthma aged 55 years or older have a mortality rate approximately 5 times higher than that in patients under 55 years.4 We previously identified control of depression, improvement of compliance, and education related inhaler technique as significant predictors of future asthma exacerbation in the elderly.7 Many studies have reported that EA is phenotypically different from non-EA (NEA).891011 However, there is a paucity of evidence regarding the risk factors contributing to exacerbation in the elderly vs. non-elderly populations.
The Bayesian network (BN), a statistical model that has been applied to machine learning, expresses the relationship among a set of variables visually through a probabilistic graphical model. Its mathematical solidity has been demonstrated in medical science.1213 Compared to conventional regression-based model, BN could provide causal structure between individual nodes that could easily be transformed into decision models.14 In this cohort study, we investigated the risk factors associated with asthma exacerbation in elderly and non-elderly patients using the BN and confirmed the results using a regression-based model.
Go to : 
MATERIALS AND METHODS
Design of the EA and NEA cohort
Our cohort combined patients from 3 existing adult asthma cohorts, the elderly asthma cohort,7 Korean asthma cohort15 and Cohort for Reality and Evolution of Adult Asthma in Korea (COREA) cohort in 2015.16 First, the EA prospective cohort in Seoul National University Hospital, was founded in 2009 (follow-up rate in 2015, 62.5%) and asthmatic patients were recruited from 9 centers. Second, Soonchunhyang University Asthma Genome Research Center, was comprised of adult asthma patients registered at the Korea Genome Research Centre for Allergy and Respiratory Diseases. Koreans aged ≥65 years and were regularly followed in stable state at enrollment. Last cohort of adult asthma patients were from the COREA. These patients were recruited by allergists or pulmonologists from 11 referral centers.
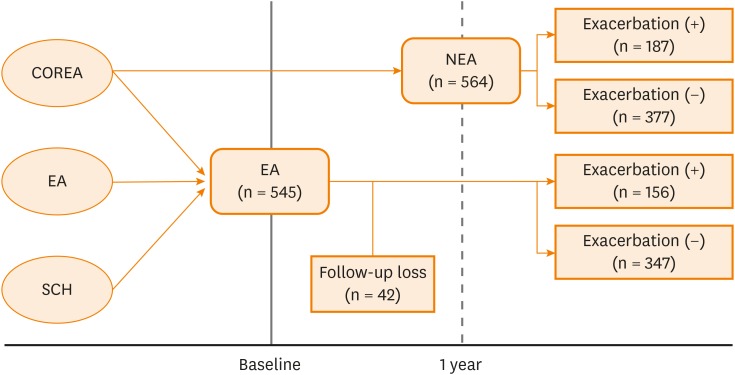
Combined patients from 3 cohorts of previously registered patients with regular outpatient follow-up were enrolled. We prospectively analyzed the baseline data of this newly established EA cohort and patients with EA from June 2015 to May 2016 (Fig. 1).
We identified patients who 1) were 65 years or older and 2) presented for follow-up observation every 3 months until May 2016. We established a unified web-based database by refining clinical information that could be merged. All predictable variables—sex, age, asthma control status, body mass index (BMI), smoking status, atopy, medication adherence, and dose of inhaled steroid—used in each analysis were collected at baseline. We investigated factors that could predict asthma exacerbation in the elderly by conducting a prospective cohort analysis during a 1-year follow-up period.
The NEA cohort was utilized as the control group from the COREA cohort. Patients aged 20 to 55 years who had at least 2 regular outpatient visits per year during the analysis period were extracted, and the occurrence of asthma exacerbations a year prior to registration were analyzed.
Institutional Review Board (IRB) approval was obtained for this study (Seoul National University Hospital IRB No. 1301-118-461), and all patients provided written informed consent to participate in this research.
Definition of EA and fixed airway obstruction
In this study, the EA cohort included adults aged 65 years or older that experienced chronic airway symptoms (dyspnea, cough, wheezing and/or sputum) and reversible airflow limitation; forced expiratory volume in 1 second (FEV1) increased by ≥ 12% or 200 mL after using a bronchodilator; airway hyper responsiveness; or a methacholine provocation test result of PC20 ≤ 16 mg/mL. Fixed airway obstruction (FAO) as a marker of airway remodeling was defined as FEV1/forced vital capacity (FVC) of less than 70% at baseline after appropriate asthma treatment for 6 months.
All patients were divided into the exacerbation and non-exacerbation groups, depending on whether they experienced at least 1 episode of acute asthma exacerbation during the previous year. The groups were analyzed for differences in their underlying baseline characteristics (asthma onset age, atopy, smoking, lung function and chronic rhinosinusitis [CRS]). Atopy was defined as a positive skin prick test response (allergen/histamine ratio > 1.0 or a mean wheal size > 3 mm) to one or more aeroallergens. Smoking was defined as a current smoker or ex-smoker with a history of tobacco use of at least 10 pack-years. Asthma exacerbation was defined according to the official American Thoracic Society/European Respiratory Society Statement17 and included at least one of the following: 1) systemic use of corticosteroid for consecutive 3 days, 2) asthma-specific emergency department visits or hospitalization and, 3) change in FEV1 > 20% compared to a personal best baseline. Data on the doses of inhaled corticosteroids (ICS) used by each EA patient at 12 months was obtained. Additionally, the information on medication possession by patients' refill count and duration, i.e., the number of days the patient should be consuming the medication was obtained and analyzed. Severe asthmatics were defined as follows: patients who did not consistently reach a well-controlled state despite the global initiative for asthma (GINA) treatment step 4 or 5; patients with well-controlled asthma who required more than 1 urgent care visit a year, needed oral steroid pulse therapy more than 3 times a year, or experienced exacerbation when the doses of oral or ICS was reduced by 25%.
Statistical analysis
Elderly and non-elderly patients with asthma were compared using the unpaired t test, Mann–Whitney U test, and χ2 test as appropriate. Potential confounders were included in the multivariable analyses if the P values were < 0.1. We performed a clinical indicator network analysis using a BN model of the significant clinical variables. All clinical variables were converted to binary variables (yes as smoking ≥ 10 pack/year, blood eosinophilia ≥ 3% in peripheral eosinophil fraction, obese ≥ 25 in BMI, atopy as positive in skin prick test). The network was implemented using the Hill-climbing algorithm of R package bnlearn.
The calculation of the sample size was based on the pooled prevalence of exacerbation in the EA 22% obtained from previous pooled data.7 We calculated the sample size with the precision error of 5% and at type 1 error of 5% and had to take at least 263 patients.
All P values were 2-tailed and considered statistically significant with P values < 0.05. Statistical analyses were performed using SPSS software (version 23.0; SPSS, Inc., Chicago, IL, USA) and R studio (version 1.1.442).
Go to :
RESULTS
Baseline characteristics
During the observation period, 503 and 583 patients were assigned to the EA and NEA groups, respectively. The mean age of the EA and NEA groups was 78.24 ± 7.18 and 36.89 ± 10.28 years, respectively. The EA group had a longer symptom duration, a higher rate of smoking, a higher proportion of obese individuals, and more patients with fixed airway obstruction, whereas the NEA group had higher eosinophil counts and higher proportions of atopy (Table 1).
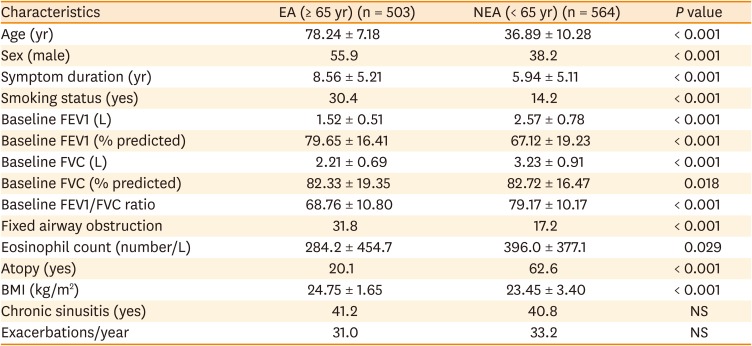
Table 1
Baseline characteristics of the EA and NEA groups
Data are shown as mean±standard deviation or number (%).
EA, elderly asthma; NEA, non-elderly asthma; BMI, body mass index; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; NS, not significant.
![]()
Clinical variables associated with asthma exacerbation in the EA and NEA groups
During the observation period, the exacerbation rate was 31.0% in the EA group and 33.2% in the NEA group (Table 2). In the EA group, patients with exacerbations were older, were of male sex, had longer symptom duration, and used a higher dose of inhaled steroid than the NEA group. In the NEA group, patients with exacerbation were older, but there were no differences in sex or symptom duration. In both the EA and NEA groups, FEV1, FVC, and FEV1/FVC were significantly lower in patients with a history of exacerbation as compared to controls. Within the EA group, fixed airway obstruction and chronic sinusitis were more frequent in patients with exacerbation, whereas within the NEA group, the eosinophil count was higher in patients with exacerbation. In elderly, 37 subjects (21.7%) were non-compliant to inhaled medications in exacerbation group while 52 (15.0%) were non-compliant in non-exacerbation group (P < 0.021). The rate of severe asthma was also higher in the exacerbation group in the both EA (64.1% vs. 29.7%, P < 0.001) and NEA (58.8% vs. 12.7%, P < 0.001).
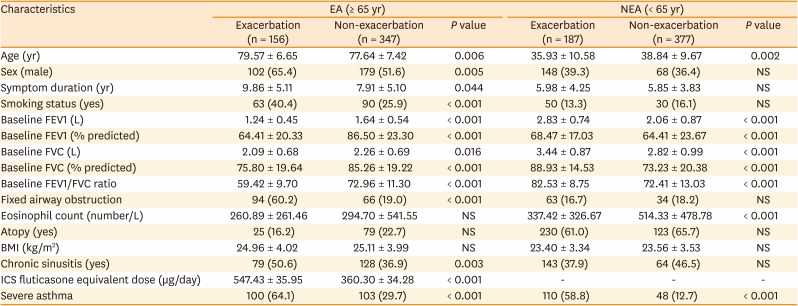
Table 2
Comparison of clinical variables between exacerbation and non-exacerbation groups among EA and NEA
Data are shown as mean ± standard deviation or number (%).
EA, elderly asthma; NEA, non-elderly asthma; BMI, body mass index; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; NS, not significant; ICS, inhaled corticosteroid.
![]()
BN analysis
BN analysis confirmed that the difference in distribution of the above-listed clinical variables between the EA and NEA groups was accurate (Fig. 2). In the EA group, the FEV1/FVC ratio and age were clinical variables directly connected to acute exacerbation events that occurred after 1 year of follow-up. In contrast, predicted FEV1% and blood eosinophil counts were clinical variables directly connected to acute exacerbations in the NEA group.
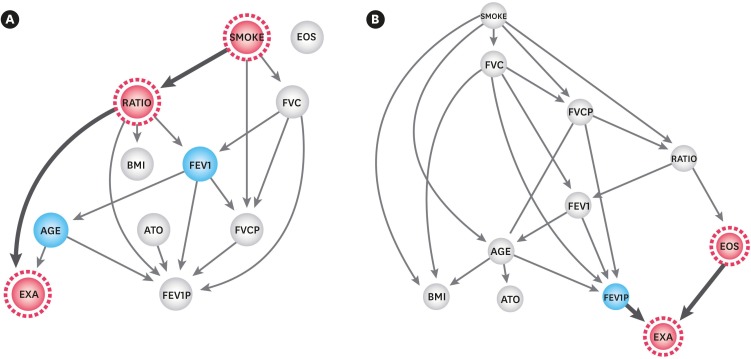 | Fig. 2Comparison of the Bayesian network analysis between (A) EA and (B) NEA.EA, elderly asthma; NEA, non-elderly asthma; EXA, exacerbation; ATO, atopy; BMI, body mass index; SMOKE, 10 pack year smoking; Ratio, forced expiratory volume in 1 second per forced vital capacity; EOS, eosinophil; FEV1, forced expiratory volume in 1 second; FEV1P, percentage of forced expiratory volume in 1 second; FVC, forced vital capacity; FVCP, percentage of forced vital capacity.
|
Multiple logistic regression for predicting exacerbation in the EA and NEA groups
To explore associations between asthma exacerbation and clinical variables in the EA and NEA groups, multiple logistic regression analyses were performed with adjustment for age, smoking status, BMI, atopy, and fixed airway obstruction (Table 3). In the EA group, the significance of the association was independent of fixed airway obstruction in multivariate logistic regression (relative risk [RR], 13.23; 95% confidence interval [CI], 5.96–31.61; P < 0.001). CRS was also significantly associated with exacerbation in the EA group (RR, 3.21; 95% CI, 1.11–4.54; P = 0.027); however, in the NEA group, eosinophil count was the only statistically significant clinical variable (RR, 1.02; 95% CI, 1.01–1.21; P = 0.019).
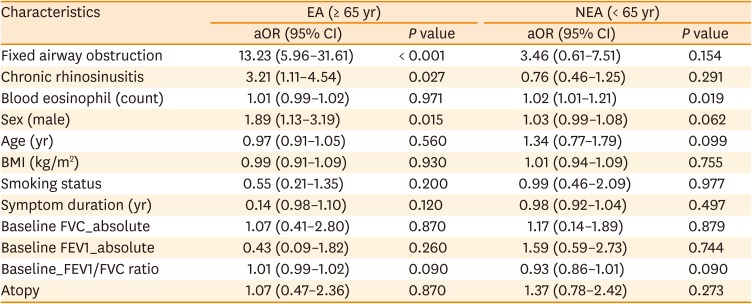
Table 3
Multiple logistic regression analysis of predictors of exacerbation in EA and NEA
EA, elderly asthma; NEA, non-elderly asthma; aOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
![]()
Go to :
DISCUSSION
In this pooled analysis of EA patients from 3 adult asthma cohorts, fixed airway obstruction and CRS were significant clinical factors associated with acute exacerbations in the EA, whereas blood eosinophil count was connected to acute exacerbations in the NEA group. This suggests that asthma may have different pathophysiological mechanisms for acute exacerbation in the EA vs. NEA groups. To the best of our knowledge, this study is the first to identify risk factors in terms of acute asthma exacerbations in elderly compared to non-elderly.
Asthma, a representative ambulatory care sensitive condition, is a disease where appropriate prevention strategies are the key challenge from the perspective of public health.18 Acute asthma exacerbations can initiate potentially preventable hospitalization, thus risk factors should be proactively identified and addressed with appropriate treatment. The present study revealed that fixed airway obstruction and CRS are important predictive factors for acute exacerbation in the EA. Our finding is significant in the following 3 domains: 1) From the perspective of public health, pulmonary function tests should be performed regularly in the EA and exacerbations should be responded to by more actively and comprehensively managing CRS associated risk groups—e.g., shorter follow-up intervals, regularly checked drug compliance. 2) From the perspective of pathophysiology, as the exacerbation mechanisms varies between the EA and the NEA, the possibility of new diagnosis and therapeutic target should be verified through future in vivo studies or omics studies. 3) Lastly, from the clinical view, ICS are the mainstay of asthma treatment in the GINA guidelines, but its effectiveness in airway remodeling remains controversial.1920 As an alternative to treatment based on existing asthma guidelines,21 drugs that affect airway remodeling—e.g., long-acting muscarinic antagonists,22 and roflumilast23—should be tested in a prospective clinical trial and an asthma guideline specialized for elderly patients may be required. Therefore, these findings suggest that current guidelines should be modified to consider fixed airway remodeling and CRS status in this vulnerable population group.
In the present study, 31.0% of the patients experienced asthma exacerbation, which was slightly higher than the 21.6% in our previous EA cohort.724 The present study mimics the real-world setting closely as compared to the previous study because the study design was advanced to a multicenter study by combining 3 asthma cohorts. Factors associated with exacerbations of the EA include smoking,25 chronic obstructive pulmonary disease (COPD),26 obesity,27 depression,7 sinusitis,2829 staphylococcal enterotoxin immunoglobulin E,3031 adherence and poor inhaler technique.7 In our study, the dose of ICS used by patients was higher, whereas the drug compliance was lower in patients with EA who experienced exacerbation than in those who did not. Additionally, education on proper use of inhalers and regular follow-up to ensure adherence to medications are necessary to prevent asthma exacerbation in patients with EA. Interestingly, we found CRS is a modifiable risk factor which is critical to prevent the exacerbation of EA. Recent findings suggest that unlike young patients, the elderly patients with CRS have neutrophilic inflammation and poor response to intranasal steroid.32 Therefore, a new therapeutic approach which targets the innate immune response should be developed for the at-risk population.
Asthma has been considered a reversible airway obstruction associated with variable levels of inflammation. However, we found that fixed airway obstruction was the most potent predictor of future acute asthma exacerbations in the elderly. Fixed airway obstruction in asthma could also called as asthma-COPD overlap (ACO). The frequency of fixed airway obstruction in adult patients with asthma is largely unknown, but it has been reported to be about 20%-49%.3334 According to a multicenter observational study, ACO in elderly patients with asthma is approximately 29%-78.2%.353637 In this study, 31.8% of the elderly patients with asthma had fixed airway obstruction, which represents small airway remodeling. We could not investigate FEF 25%-75% in this cohort; however, a previous study reported that post-bronchodilator FEV1/FVC, obtained through computed tomography measurements, can be used as surrogate markers of airway remodeling.38 Persistent airway obstruction makes it difficult to distinguish between asthma and COPD, especially when the elderly patients with asthma is a heavy smoker or a ‘super-old (≥90 years-of-age)’ individual. As is widely known, older patients with asthma that experience fixed airway obstruction and concurrent atopy may have the so-called ACO.39 However, though smoking node is associated with the FEV1/FVC in BN, fixed airway obstruction is most significant risk factor independently of smoking in multiple regression analysis. These findings indicate that airway remodeling is independent risk factor for exacerbation in the EA group. We suggest that fixed airway obstruction is sufficient to be recognized as a distinct phenotype from asthma or COPD. Additional multidisciplinary approaches are required to manage the airway remodeling in the elderly.
Our study had several limitations when interpreting our findings. First, the smoking rate was 30% in the EA group. Thus, the possibility of ACO cannot be eliminated. However, there is no gold standard for the diagnosis of ACO in the EA patients. This is the rationale for searching and validating diagnostic criteria for ACO in actual practice. Second, as our analysis is based on a 1-year follow up study, any alteration in disease progression including mortality was not investigated. Third, although this study is based on a prospective design, the omission of randomization in the process of merging 3 cohorts may have introduced unknown bias. However, there was no intentional bias in the selection of patients to merge from the previous cohorts, this was similar to random assignment. Fourth, NEA patients were not originally designed to compare the risk factors in asthma exacerbation to EA patients. Therefore, this group analysis had to be retrospective in nature. Finally, the number of comorbidities is an important factor which could affect the outcomes of EA. We assessed comorbidities in the elderly patients with questionnaires; however, the incidence of comorbidities in patients with EA may be extremely low because of recall bias (e.g., overall hypertension incidence in the EA cohort, 1.6%). Therefore, further studies are required to directly examine the effects of comorbidity control on EA. However, this study provides valuable information regarding the role of FAO and CRS in the exacerbations of the EA by longitudinal observation.
In summary, we confirmed that the asthma exacerbation rate was not different between elderly and non-elderly patients, but the predicting risk factors were distinctive in this study. The present study suggests that asthma exacerbation in elderly patients is associated with fixed airway obstruction and CRS, whereas eosinophil count was the most significant risk factor for asthma exacerbation in non-elderly patients. Based on multiple regression analysis, we confirmed that fixed airway obstruction was the most important predictor for asthma exacerbation in the elderly. Thus, particularly, when fixed airway obstruction and CRS are found in elderly patients with asthma, clinicians should consider the potential risk of asthma exacerbation. Long-term prospective studies correlating physiological variables are necessary to further explore EA versus NEA.
Go to :
 XML Download
XML Download