

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Local anesthesia is one of the most delicate and difficult procedures in pediatric dental treatment. The injection of the anesthetic solution produces the greatest negative response in children [1]. Several research studies support the proposition that pain or the fear of pain is a primary source of dental anxiety and a major obstacle for seeking dental care [23]. Some children find it difficult to cope with the stimuli and behavioral demands associated with dental experience. This could be due to fear of the needle, bodily harm, or a general fear of the unknown. Successful treatment of pediatric patients, in terms of allaying their anxiety and discomfort during restorative and surgical procedures, is facilitated by profound local anesthesia [4].
During the administration of a local anesthetic injection, an anxious patient might perceive more severe pain of longer duration than would a less anxious patients [5]. Visually and psychologically, the dental syringe is perceived as a threatening instrument, especially by children. Camouflaging the syringe can be an effective distraction tool and can allay dental fear and anxiety.
To the best our knowledge there are very limited studies where syringes have been camouflaged resulting in the entire injection apparatus being hidden from the sight of children. The Syringe Sleeve by Angelus™ makes it possible to camouflage the threatening metal dental syringe using an autoclavable plastic in the shape of a toy alligator.
The aims of this study were to determine whether camouflaging dental syringes has a positive influence on the behavior of children and causes less anxiety, based on changes in pulse rate, and to compare patient and operator preferences between camouflaged and conventional syringes.
METHODS
This randomized, crossover clinical pilot study was conducted in the Department of Pediatric and Preventive Dentistry, M.R Ambedkar Dental College and Hospital, after obtaining approval from the institutional review board and ethics committee (IRB Number: MRADC&H/ECIRB/2017-18) and after obtaining written informed consent from the parents of children involved in the study.
Based on previously published literature, after setting the level of significance at P < 0.05 and power of study as 80%, the required sample size was estimated as 29. This was rounded off to 30 in order to have equal groups of 15.
The study included 30 children aged 6 to 11 years (15 boys and 15 girls). Children were distributed equally into two groups according to age (group 1: 6–8 years and group 2: 9–11 years).
Only patients who required infiltration anesthesia in at least two quadrants, who had never experienced dental injection, and who belonged to the Frankl's positive and definitely positive behavior (Frankl behavior rating scale) [6] were included in the study. All patients with acute signs and symptoms which required emergency treatment, patients with painful dental experiences in the past, and medically compromised patients were excluded from the study.
The armamentarium of the study is shown in Fig. 1.
Children in each age group were treated in two separate appointments where they were further randomly distributed. Fifteen children from the total sample were treated with camouflaged syringes (Fig. 2) in the first appointment and conventional syringes (Fig. 3) in the next appointment, while the remaining fifteen children were treated with conventional and camouflaged syringes during the first and second appointments, respectively, to avoid preference bias.
All the treatment procedures were carried out by one pediatric dentist who used euphemisms and the tell-showdo technique to convince patients for treatment. In both appointments, prior to injection of local anesthetic, topical anesthetic spray was administered at the injection site and baseline pulse rate was noted using a finger pulse oximeter. Afterwards, the injection was administered using a pre-determined syringe type, either a conventional or camouflaged syringe, during which a third person noted the pulse rate. After the injection, the operator graded the child's behavior using the Faces, Legs, Arms, Crying, Consolability (FLACC) behavior pain scale [7]. On the second appointment, all the children were subjected to the same procedure, but a different syringe type was used. After both appointments, the children were asked to state their syringe preference. The syringe preference of the operator was inferred from the FLACC score. The lower score, i.e., the better behavior, was recorded as the operator preference. The operator was assumed to have no preference if FLACC scores were equal for both appointments.
The data collected was tabulated and subjected to statistical analyses. Statistical analyses including the Fisher's exact test and unpaired t- test were performed using the SPSS statistical software package version 20.0. Results for the same have been mentioned below.
RESULTS
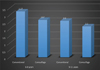
The mean FLACC scores in both groups were lower when camouflaged syringes were used indicating a better behavior. In group 1, the mean FLACC scores when conventional and camouflaged syringes were used were 3.27 ± 1.94 and 2.67 ± 1.59, respectively while that for group 2 were 2.60 ± 2.03 and 2.20 ± 1.70, respectively. The P values after comparison of the FLACC scores when conventional and camouflaged syringes were used in groups 1 and 2 were 0.363 and 0.563, respectively. This is shown in Fig. 4. The FLACC scores were not significantly different between both groups when conventional and camouflaged syringes were used.
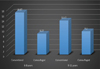
The mean increase in pulse rate was lower in both groups when camouflage syringe was used indicating lower anxiety levels. In group 1, the pulse rate when conventional and camouflaged syringes were used were 16.67 ± 15.77 bpm and 8.27 ± 12.69 bpm, respectively while that for group 2 were used were 13.47 ± 9.06 bpm and 9.20 ± 9.96 bpm, respectively. The P values after comparison of the pulse rate when conventional and camouflaged syringes were used in groups 1 and 2 were 0.119 and 0.230, respectively. The pulse rates were not significantly different between both groups when conventional and camouflaged syringes were used. This is shown in Fig. 5.
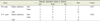
12 out of 15 (80%) patients in group 1 preferred the camouflaged syringe whereas only 8 out of 15 (53%) patients in group 2 preferred it. However, the operator preferred the camouflaged syringe for 8 patients in group 1 and 7 patients in group 2. A statistically significant correlation was noted between patient and operator preferences in group 2 (P = 0.044) as shown in Table 1.
DISCUSSION
Fear of dentists and dental procedures, and the associated anxiety are common among patients of pediatric age [8]. Middle childhood, i.e., 6–11 years was selected for the study because the children in this age group have good cognitive skills.
A number of recent studies used the pulse oximeter [910] as an objective measure of anxiety. In the present study, a small increase in pulse rate was noted when camouflage syringes were used, in both groups suggestive of lower anxiety.
The FLACC Behavioral Scale comprises behavioral categories and a variety of descriptors that are reliably associated with pain in children, adults with cognitive impairment, and critically ill adults, supporting the content validity of this tool in these groups of people.
Recent studies have also used the FLACC scale [1112] to rate behavior in children during dental treatment. In the present study, lower FLACC scores were noted when camouflaged syringes were used indicating better behavior during the injection administration.
There is very limited literature on camouflaging syringes to positively influence behavior and decrease anxiety. A clinical trial was conducted to evaluate the efficacy of a camouflage sleeve created using cold cure acrylic [8]. The results of that study also strongly favor the use of camouflaged syringes to reduce dental fear and anxiety in children, which is in accordance with the present study.
Two studies [1314] were conducted to evaluate the reaction of children to dental injection after viewing the needle. In these studies, showing or hiding the needle had no influence on the reaction of children, which is contradictory to the present study as the needle hidden in the camouflaged syringe had a positive influence on behavior and anxiety.
In the present study most children, especially younger children, preferred the camouflaged alternative possibly because they are more easily distracted and the toy-like appearance of the camouflaged syringe takes away the fear-provoking stimuli of a conventional syringe. An older child would probably be less easily distracted with a camouflaged syringe as compared to a younger child. This could explain the lower preference rate of camouflaged syringe in group 2 than group 1. The operator preference was inferred from the FLACC scores. Syringes with lower FLACC scores were noted as the operator preference. If both the scores were equal, then the operator was said to have no preference. In our study, we found that even the operators preferred the camouflaged syringe in about half of the cases. They had no preference in about one-third of the cases and preferred the conventional syringe in only about one-sixth of the cases among patients in all age groups. This therefore shows that even operators preferred using camouflaged syringes possibly because they were more likely to induce positive behavior in children.
In the present study a novel, simple and child-friendly sleeve for the metal dental syringe developed by Angelus™ was used. The main aim was to conceal the needle from the child's sight while still keeping the syringe functional in order to deliver the intended drug.
The advantages of using this sleeve by Angelus™ is that it is playful, it conceals the needle, it acts as a distraction tool, it is autoclavable, and it is commercially available.
The sample size in our study is too small to make accurate conclusions regarding the product. In addition, due to its large size, it is not currently known whether the Angelus™ sleeve is acceptable to dental practitioners since its maneuverability may be somewhat restricted compared to conventional syringes. The sleeve is presently only compatible with the metal aspirating dental syringe which uses local anesthesia cartridges and disposable needles. Before generalizing the results of this study, it should be noted that only children under the age of 11 years were included in the study and the toy-like appearance of the syringes may not impress or distract older children or adults.
It is the responsibility of pedodontists to make dentistry as child-friendly and pain-free as possible to bring about positive change in the behavior of children during dental treatment.
There are no previously published studies which used this camouflaged sleeve by Angelus™. Hence, we decided to conduct a pilot study using the product. More extensive research with larger sample sizes should be conducted with the product for more statistically significant results.
In this study, we showed that a simple and novel innovation to camouflage conventional syringes can result in improved outcomes related to dental fear and anxiety.



 XML Download
XML Download