

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Local anesthesia is applied topically or administered by injection to control pain in the body. Unlike general anesthesia, local anesthetics do not cause loss of consciousness. Topical anesthetics are used to numb mucosa of the nose, ear and throat, anus, and genital area. It is used adjunctively to relieve pain and to help patients feel more comfortable before surgery. In addition to their anesthetic properties, local anesthetics also possess antimicrobial effects. They have been shown to inhibit and kill a wide spectrum of bacteria and fungus [1]. In dentistry, topical anesthetics are typically used to anesthetize the mucosal surface area of the oral cavity prior to local anesthetic injection [2].
When administering local dental anesthesia, bacteria in the normal oral flora can pass into the tissue by needle injection through the mucous membrane. These bacteria can cause suppurated local infections or odontogenic bacteremia after dental interventions [345]. Therefore, it is possible that the antimicrobial properties of topical anesthetics may provide an additional benefit as an antiseptic to prevent post-operative infections.
We reviewed the effect of local anesthetics on antimicrobial activity with a focus on dentistry. These anesthetics were tested against a broad spectrum of microorganisms, including oral and skin microflora, opportunistic pathogenic bacteria, and fungi. The collective results of in vitro and in vivo studies conducted over many years have substantiated a supplemental role for local anesthetics in the probable prevention and treatment of interventional site infections.
CLASSIFICATION OF ANESTHETICS AND THEIR EFFECTIVENESS IN DENTAL ANESTHESIA
The structure of an anesthetic molecule consists of three components: 1) the lipophilic aromatic ring, 2) an intermediate ester or amide linkage, and 3) the tertiary amine, which influences the clinical properties. The potency of a local anesthetic depends on lipid solubility of the aromatic rings and its substitute compound along with the tertiary amine [67]. For example, bupivacaine is more potent than articaine due to its greater lipid solubility. Lipid solubility also affects the onset of the anesthetic as it enables rapid diffusion of the drug through cell membranes. Thus, the potency of 0.5% bupivacaine is comparable to 4% articaine [8]. Conversely, concentration or the presence of other factors may have a greater effect on onset [7]. Epinephrine in the solution of the local anesthetic decreased its vascular absorption rate, thereby enhancing the deep numbness and long duration of local action [8].
Local anesthetics can be classified as ester-type or amide-type based on its intermediate chain. Drug metabolism is different for each type; esters are hydrolyzed in blood plasma by plasma esterases, whereas amides are metabolized in the liver. The incidence of allergic reaction, from skin rash to anaphylaxis, is highly associated with ester anesthetics due to the formation of p-aminobenzoic acid (PABA) [6], which may cross-react with similar compounds such as sulfa antibiotics or metabisulfite [9].
1. Ester-type anesthetics
Cocaine was the first local anesthetic drug, introduced by Koller in 1884 [10]. For oral use, cocaine is available in liquid form mixed with adrenaline for topical anesthesia. It has a reported high risk of addiction and toxicity.
Topical benzocaine is an ester-type anesthetic agent composed of p-aminobenzoic acid (PABA) that can induce allergic reactions. Benzocaine is available in various preparations, such as gel, gel patch, spray, ointment, or solution. Concentrations used range from 6% to 20%, and has multiple uses. Topical use of 20% benzocaine provides anesthetic effect within 30 seconds but requires approximately 2 – 3 minutes to reach adequate depth. It effectively reduces pain caused by injection into the alveolar mucosa and tongue, but only slightly affects the palatal mucosa because of the tissue thickness and dense nerve supply [11]. The duration of action is approximately 5 – 15 minutes after onset. Benzocaine-associated methemoglobinemia has been regularly reported [12].
Tetracaine, also an ester derivative of PABA, is more effective than cocaine [13]. Tetracaine is available in spray and ointment forms of 0.2% to 2.0% concentration. It produces rapid onset within 10 – 20 seconds, with a short duration of action of 10 – 15 minutes. Tetracaine is quickly absorbed into the mucous membrane. Limiting use to 20 mg per session to reduce the risk of adverse reactions has been recommended [14].
2. Amide-type anesthetics
Lidocaine is the only amide-type anesthetic that is available in both topical and injectable forms. In dentistry, many forms and concentrations of lidocaine are used, from 2 – 5% gel and solution, 5% ointment, 10% spray, and 20% lidocaine patch [15]. Lidocaine has a potency comparable to benzocaine. It requires three minutes after application to reach adequate anesthesia [16]. Lidocaine is highly effective on alveolar mucous but is less effective on palatal mucous membrane. It is used as an analgesic ingredient in Magic Mouth Wash and mouth rinse products for oral mucositis in patients receiving radiation and chemotherapy [17].
Prilocaine is also used in combination with other topical anesthetics, such as in Eutectic mixture of local anesthetics (EMLA) and Oraqix [18]. The maximum dose is 6 mg/kg in adults and should not exceed 400 mg. Prilocaine has low cardiac toxicity and is relatively safe in pregnant women [19].
EMLA, which contains 2.5% lidocaine and 2.5% prilocaine, is used in procedures or surgeries that cause minimal to considerable pain. EMLA is also commonly used as a topical skin analgesic cream to reduce pain, anxiety, and discomfort associated with venous cannulation in adults and children [20].
ADVERSE EFFECTS OF LOCAL ANESTHETICS
Common adverse effects of topical anesthetics are temporary altered sense of taste and allergy. The signs and symptoms of allergic reactions are itching, edema, nasal discharge, shortness of breath, wheezing, and headache [2324].
Allergic reactions are infrequent in amide-type anesthetics [25]. Methemoglobinemia is another adverse reaction caused by anesthetics that can lead to severe or fatal cyanosis and additional adverse effects [12]. Adverse effects from using prilocaine and EMLA creams have been reported [26]. More severe complications can occur, including central nervous system toxicity, cardiovascular toxicity, and methemoglobinemia [2728].
MECHANISM OF ACTION OF LOCAL ANESTHETICS
Topical anesthetics eliminate pain by inhibiting signal transmission of tiny nerve endings at the surface [29]. Local anesthetics interrupt neural conduction by inhibiting sodium ion influx through sodium channels within neuronal membranes during their activated and inactivated states. Sensitivity to anesthetics depends on the diameter of neural fibers. Differential sensitivity consequently affects the recovery of neural fibers in first the motor, then the sensory, and finally the autonomic fibers [30].
TOPICAL ANESTHETIC AGENTS USED IN DENTISTRY
Various forms of topical anesthetics, such as sprays, solutions, gels, and ointments, and indicated uses have been developed to facilitate clinical use by dentists [213]. The effective duration of a topical anesthetic is 10 – 50 minutes depending on anesthetic usage. When used prior to local anesthetics injection, at least two minutes is required after application for significant anesthetic effect [25].
ANTIMICROBIAL EFFECT OF LOCAL ANESTHESIA
1. Antimicrobial properties of local anesthesia
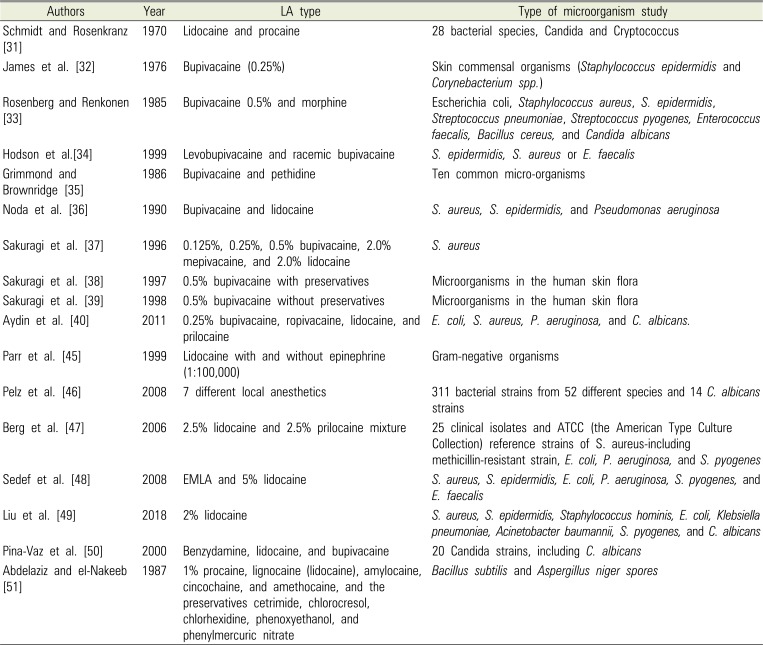
Numerous previous studies have reported antimicrobial activity of several local anesthetics since their first observations in 1909 (Table 1) [3132333435363738394045464748495051]. The bacteria investigated were all common pathogens. Noda et al. [36] indicated that bupivacaine had greater antibacterial activity than lidocaine. At equal concentrations, greater antibacterial activity was found when preservatives were added to the anesthetics, and the authors observed that while the preservatives alone were weakly bacteriostatic, they were not bactericidal. This points to the significance of bactericidal activity in the anesthetics.
From 1996 to 1998, publications by Sakuragi and colleagues [373839] also indicated that the rate and potency of antimicrobial activity were dose-dependent, time-dependent, and temperature-dependent. They also reported that 0.5% bupivacaine showed the greatest bactericidal activity on methicillin-resistant Staphylococcus aureus.
Aydin et al. [40] showed that a concentration of 1% prilocaine inhibited the growth of Escherichia coli, S. aureus, and Pseudomonas aeruginosa, whereas lidocaine inhibited only P. aeruginosa. While 0.25% bupivacaine was found to inhibit only P. aeruginosa, ropivacaine failed to inhibit the growth of any pathogens [40]. These findings were confirmed by many other studies [41424344]. In vitro, epinephrine appearing in clinical doses of local anesthetic agents has shown no antimicrobial effect. In 1999, Parr et al. [45] demonstrated this in Enterococcus faecalis and vancomycin-resistant enterococci, E. coli, P. aeruginosa, and S. aureus and methicillin-resistant S. aureus. Gram-negative organisms showed the highest sensitivity to lidocaine whereas S. aureus was the least sensitive. Time-kill studies were carried out on bacteria exposed to various clinical concentrations of lidocaine with and without epinephrine. Lidocaine demonstrated a dose-dependent inhibition of growth for all strains of bacteria tested. The addition of epinephrine to the local anesthetic did not affect the susceptibility of bacteria to lidocaine [45]. These results also suggested that lidocaine may have a role in the prophylaxis and treatment of surgical wound infections, particularly in methicillin- and vancomycin-resistant bacterial infections.
A comparison study of antimicrobial effects [46] of 1) articaine, 2) bupivacaine, 3) mepivacaine, 4) prilocaine, 5) lidocaine, 6) butanilicaine, and 7) procaine in combination with four preservatives and vasoconstrictive components showed different minimal inhibitory concentrations (MIC) and minimal bactericidal concentrations (MBC). Antimicrobial activity was proven to come from the anesthetic component, and not from the preservative or vasoconstrictor components. An in vitro study of 25 clinical isolates and ATCC (American Type Culture Collection) reference strains showed powerful antibacterial effects of EMLA [47]. Subsequently, Sedef et al. [48] showed dose-dependent antibacterial activity of EMLA and 5% lidocaine. Recently, Liu et al. [49] reported that 2% lidocaine shows strong antimicrobial activity against eight isolates of commonly encountered bacterial strains in periprosthetic joint infection.
In the case of Candida albicans, Rodrigues et al. [43] suggested that local anesthetics inhibited fungal germ tube formation secondary to a blockade of ionic channels. Pina-Vaz et al. [50] also found fungistatic activity at lower concentrations secondary to yeast metabolic impairment, and fungicidal activity at higher concentrations secondary to cytoplasmic membrane damage. Clinical doses of lidocaine and procaine have demonstrated inhibitory effects on growth of various species of bacteria and fungi.
Sporicidal activity of local anesthetics and their preservatives were tested by Abdelaziz and el-Nakeeb [51]. Inhibition of growth proved to be temperature-dependent for all agents. Higher temperatures were required to elicit sporicidal activity against Bacillus subtilis, compared to Aspergillus niger. Among the preservatives, chlorocresol/local anesthetic combinations also exhibited the highest sporicidal activity [51].
2. Antimicrobial mechanism of action of local anesthetics
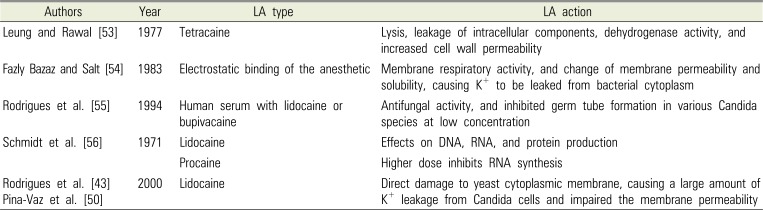
It has been suggested that the inhibitory effect of local anesthetics on bacterial growth results from the disruption of the bacterial cell wall or cytoplasmic membrane, leading to leakage of cellular components and subsequent cell lysis [52]. Table 2 [435053545556] summarizes the results of studies on local anesthetic action and antimicrobial mechanism. It has been reported that penetration of bacterial membranes results from the electrostatic binding of anesthetic molecules to polar groups relating to the hydrophobic character of the anesthetic on the surface of the membrane [54]. Anesthetic molecules inhibit membrane respiratory activity, and change membrane permeability and solubility, causing K+ to be leaked from the bacterial cytoplasm. Including anesthetic agents at high concentrations has shown antifungal activity, and at low concentrations has shown inhibition of germ tube formation in various Candida species [55]. Conversely, there are limited studies that attribute the mechanism of action of antimicrobial activity of local anesthetics.
3. Antimicrobial effects of local anesthetics on infection control
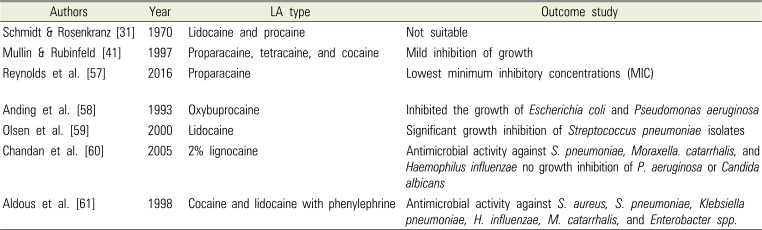
This paper first reported that isolating and culturing pathogenic microorganisms in samples collected from an area that might be contaminated with the anesthetics can be problematic to the microbiological laboratory [47]. The antibacterial effect of topical anesthetics may lead to false-negative cultures from the specimens. Numerous studies have recommended using a low concentration of anesthetic to decrease the possibility of obtaining false-negative cultures. Table 3 lists the studies on antimicrobial effects in local anesthetics for infection control [31415758596061].
Reynolds et al. [57] found that proparacaine had the lowest MICs, lower than that of povidone-iodine. All tested anesthetics and povidone-iodine inhibited bacterial growth at commercially available concentrations. For the diagnosis of pneumonia, Anding et al. [58] found significant bactericidal activity of the local anesthetic oxybuprocaine against Streptococcus pneumoniae and Haemophilus influenzae, even at the lowest concentration of 0.01%. At 1%, oxybuprocaine inhibited the growth of E. coli and P. aeruginosa. Collectively, growth inhibition by local anesthetics is likely a reason behind low sensitivity observed in microbiological culture. Therefore, it is recommended that clinicians use a low concentration of minimally inhibitory local anesthetics to optimize culture yields.
4. Antimicrobial effects of local anesthetics in dentistry
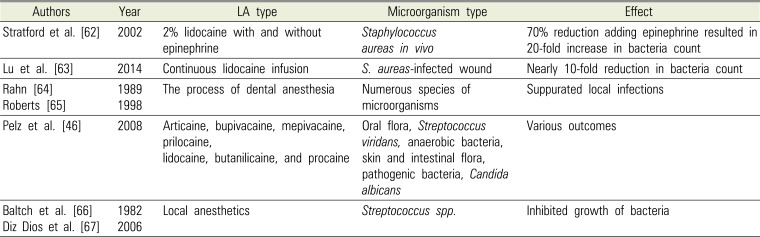
Antibacterial activity demonstrated over the past several decades indicates that local anesthetics might help eradicate microorganisms that are introduced into the tissues or blood vessels. In the case of methicillin and vancomycin-resistant bacteria, treatment of surgical wound infection has mandated a broader application for local anesthetics [45]. This suggests that the surgical benefit of local anesthesia may extend beyond its analgesic properties, as shown in Table 4 [46626364656667].
Stratford et al. [62] reported that lidocaine produced a 70% reduction in bacterial count in vivo, however adding epinephrine resulted in a 20-fold increase in bacterial count compared to controls. This suggested that hypoxia resulting from vasoconstriction may directly increase the risk of surgical site infection [62]. Lu et al. [63] used a mouse model to demonstrate that infusion of 2% lidocaine in a S. aureus-infected wound showed a nearly 10-fold reduction in bacteria count.
In the process of dental anesthetic injection, oral bacteria can enter the tissue following perforation of the mucous membrane. Dental local anesthesia in compromised patients may, therefore, lead to suppurate local infections or odontogenic bacteremia, as has been shown to occur in other dental surgery interventions. These circumstances have raised the issue of routine antibiotic prophylaxis in oral surgery [6465].
Pelz et al. [46] studied antimicrobial activity of commonly used local anesthetics in dentistry, occurring at the concentrations of the seven commercially available local anesthetics. The tested microorganisms were oral flora, including Streptococcus viridans and anaerobic bacteria, skin and intestinal flora, opportunistic pathogenic bacteria, and C. albicans strains.
The antimicrobial activity of methyl-4-hydroxybenzoate, sodium bisulfite, adrenaline hydrogen tartrate, and adrenaline (preservative and vasoconstrictive components in anesthetics) were tested. Ultracaine D-S and its active substance, articaine hydrochloride, similarly showed the most prominent antimicrobial activity with regards to both MIC and MBC. The routinely applied concentration of Ultracaine D-S and Hostacaine was roughly four-times higher and two-times higher, respectively, than the MBC values for the tested bacteria, whereas MBC values were not reached or exceeded with the concentrations of other anesthetics used. Novocaine showed the lowest antimicrobial activity and did not inhibit 35 species tested. Due to the results obtained with nosocomial strains of E. coli, S. aureus, and P. aeruginosa, disinfection of the mucous membranes should be performed routinely in immunocompromised patients, regardless of the anesthetic used.
A solution of 1:100,000 epinephrine and 2% Xylocaine®, was shown to inhibit the growth of specific organisms and to be bactericidal to others. Its bactericidal activity was significantly less than 2% Xylocaine® without epinephrine.
Therefore, dentists can apply the potential use of local anesthetics as antiseptics in a variety of dental procedures to eliminate bacteria on the surface areas of treatment. During dental treatment, local anesthetic injection techniques, such as buccal infiltration and conventional and modified intraligamental injection, have been found to significantly increase the rate of bacteremia [4]. It was shown that elevated levels of bacteria in the bloodstream that increased immediately after local anesthetic injection returned to normal within one hour [5].
Local anesthetics can inhibit the growth of bacteria that have inoculated into the soft tissue during the injection process. For dental treatments such as tooth extraction and root scaling, antibiotic prophylaxis is recommended prior to the dental procedure to decrease bacteremia rates, especially in immune-compromised patients or patients under immunosuppressive drugs [36667].
Alternatively, infection may occur after dentoalveolar surgery such as third molar removal and dental implant placement [6869]. This can occur from contamination during the surgical process, in suturing, in the environment, as well as from patient hygiene [70]. Prophylaxis antibiotics should be prescribed prior to the operation to reduce the rate of postoperative infection [6871].
For dental implant surgery, the use of chlorhexidine mouth rinse significantly reduces plaque collection and the microorganisms that relate to postoperative infection. Among several antibacterial agents, chlorhexidine is recommended as the gold standard for surgical site infection control due to its broad spectrum and antiseptic efficacy [72].
In patients with oral mucositis who have received radiotherapy, symptoms can arise from acute inflammation of oral mucosa, tongue, and pharynx. Agents are required to reduce pain and prevent infection. In general, the local anesthetics diphenhydramine, xylocaine, and lidocaine are the drugs of choice to relieve the pain, and non-alcohol-containing chlorhexidine is recommended to prevent the infection [7374].
CONCLUSION
Local anesthetics not only serve as agents for pain control but possess antimicrobial activity as well. Caution should be exercised when administering local anesthetics prior to diagnostic procedures in which culture specimens are to be obtained, as the antimicrobial activity of the local anesthetic could lead to false-negative results. In such cases, it is recommended that the lowest concentration possible of a mildly antimicrobial agent be used to optimize culture yields.
However, local anesthetics can be considered as an adjunct to traditional antimicrobial use in the clinical or laboratory setting. Greater concentration, longer exposure, and higher temperature each correlate with a proportional increase in microbial growth inhibition. Multiple local anesthetics at concentrations typically used in the clinical setting, such as 0.125% – 0.75% bupivacaine and 1% – 3% lidocaine, inhibit the growth of numerous bacteria and fungi. Bupivacaine and lidocaine inhibit growth to a significantly higher degree than ropivacaine.
Minimal information is available on the antimicrobial efficacy of anesthetic agents in dental clinical settings. The rate of onset of antimicrobial activity of local anesthetics as well as whether the activity is bactericidal or bacteriostatic is still unknown. Similarly, antimicrobial activity of local anesthetics with preservatives has not been studied. A statement on the possible prophylaxis use of topical anesthetics in dentistry cannot currently be made unless more clinical studies have confirmed.
 XML Download
XML Download