

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Generally, oral intubation is performed to secure the airway during general anesthesia; however, because oral cavity is operation field during oral and maxillofacial surgery and dental treatment, nasotracheal intubation is performed to maintain the airway [1]. For nasotracheal intubation, generally, a laryngoscope and Magill forceps are used; however, if any difficulty in securing the airway is expected, for example, cervical fracture and dislocation or airway tumor and abscess, fiberoptic nasotracheal intubation (FNI) is performed. Depending on the situation, if risks, such as difficult facial mask ventilation, restricted mouth opening, or pulmonary aspiration are present, then awake fiberoptic intubation is performed [2]. An anesthesiology resident should be able to perform FNI for the management of difficult airways.
Because of the complex anatomical structure of the nasal cavity, performing nasotracheal intubation can cause complications such as nasal cavity damage, dental injuries, airway bleeding and bronchospasm. Thus, securing the airway during FNI can be difficult due to increased risk for bleeding and discharge during emergency situations such as damage to the oral cavity, edema, or hematoma after surgery [3]. Therefore, training is required to perform proficient awake fiberoptic intubation.
FNI can be performed in two ways: inserting the tube into the nasal cavity first, then finding the vocal cord using a fiberscope; or inserting the fiberscope first into trachea through the nasal cavity, then inserting the tube into the trachea through the nostril. Although the former method was introduced earlier, and requires fiberscope insertion when it is difficult to secure the airway [4] and the risk for nasal bleeding may increase, the tube can be used as a guide to easily insert a flexible endoscope into the oral cavity. The latter method is generally performed if any difficulty in securing the airway is initially expected when performing FNI. Although interference of the visual field due to bleeding in the nasal cavity can be prevented, damage to the nasal cavity can be more severe when inserting the tube following the fiberscope.
To train intubation using a fiberscope in case of difficulty in securing the airway during nasotracheal intubation, the method of inserting the tube first into the nasal cavity was taught. Furthermore, awake intubation training was also conducted for the same method.
For every nasotracheal intubation using a fiberscope that was performed, success status was evaluated to plot a learning curve and the time it takes to train individuals to perform awake FNI. In addition, factors that influence the level of difficulty in FNI were also investigated.
Go to : 
METHODS
1. Study subjects
Operators: For this study, Institutional Review Board approval was obtained from Seoul National University Dental Hospital (SNUDH, No. L0605-12). Second-year anesthesiology residents of Seoul National University Hospital who were on 1-month rotation from August 2005 to April 2007 were included. Although the operators had at least 1 year of experience with oral intubation, they had virtually no experience with nasotracheal intubation and FNI.
Patients: All patients who were undergoing surgery at SNUDH during the residents' rotation period and receiving nasotracheal intubation were considered. However, only those who were educated about the possible complications of general anesthesia and nasotracheal intubation and provided informed written consent were included in the study. Patients with American Society of Anesthesiologists physical class III or lower, children < 8 years of age, and patients with lung or heart disease were excluded. Patients in whom a difficulty with nasotracheal intubation was anticipated due to nasal cavity obstruction, mass or deformity, and those undergoing emergency surgery were also excluded. If the use of mask ventilation was expected to be difficult, due to reasons such as severe maxillofacial deformities or mass in the oral cavity, or the visual field with laryngoscope was not satisfactory due to trismus, awake FNI was performed.
Study subjects only included individuals for whom intubation was performed by residents. Each resident performed FNI in at least 40 patients.
2. Protocol
2.1. Resident training
All residents who participated received more than 1 h of FNI practice using an airway management trainer (Laerdal Co., Stavanger, Norway) before performing nasotracheal intubation. Up to the third time performing FNI on patients, specialists provided training using videos, and these attempts were not included in the study analysis.
2.2. Preparation of general anesthesia and nasotracheal intubation
When a patient was transferred to the operating room, the anatomical condition of the nasal cavity was assessed, and the appropriate nostril was chosen for intubation. An RAE endotracheal tube with internal diameter (ID) 6.5 mm was used in women, while ID 7.0 mm was used in men. For children between 8 and 15 years of age, the (age/4 +3) mm equation was used to select the appropriate RAE tube ID with cuff.
Anticholinergics were not administered as pretreatment for anesthesia. The tube was softened by immersion in water heated to a temperature of approximately 40℃, and then coated with surgical gel for insertion into the nasal cavity. While performing intubation, an assistant held the patient's chin upward.
A flexible endoscope with a diameter of 4.2 mm (LF2, Olympus Co., Japan) was used and if the tube ID was < 5.5 mm, then a 2.8 mm tube (LF-DP, Olympus Co., Japan) was used. The ocular of the endoscope was equipped with a camera (AR-TF08E; Olympus Co., Japan) that enables viewing through a video system. While performing FNI, the operator viewed through the ocular, and the observer viewed the monitor. The fiberscope was cleaned with antiseptic solution before and after use to minimize infection risk. Before intubation, the flexible endoscope was coated with surgical lubricant and the lens was wiped with a cotton ball soaked in alcohol to secure the view.
Before injecting the anesthetic, 100% oxygen ventilation was administered. Intravenous anesthetic (thiopental or propofol) was injected and the inhalation anesthetic or propofol was continuously administered until complete loss of consciousness. Vecuronium 0.15 mg/kg was injected to induce complete muscle relaxation, then nasotracheal intubation was performed.
If awake intubation was required, the patient was nebulized with 4% lidocaine for 20 min, then fentanyl 25–50 mcg and midazolam 1–2 mg were administered by intravenous injection before performing FNI.
2.3. Evaluation of FNI success
FNI success was evaluated as the time required for intubation. The endotracheal tube was inserted into the nasal cavity and tip of the tube was positioned at the nasopharynx. Next, the fiberscope was inserted into the endotracheal tube to find the vocal cord, and then the tip of the fiberscope was inserted through the trachea until the carina was seen. An RAE tube was inserted into the trachea following the fiberscope. An assistant held the patient's chin upward with one hand to facilitate intubation. Another assistant measured the time from the moment the tip of the fiberscope was inserted into the endotracheal tube until the carina was seen on the monitor.
2.4. Time measurement interval and safety maintenance
Before inserting the endotracheal tube into the nostril, 100% oxygen saturation level was maintained by manual ventilation of oxygen and inhalation anesthetics. Tracheal intubation time was restricted to 2 min 30 s. Once 2 min 30 s passed, the endotracheal tube was removed from the nasal cavity, and 100% oxygen was provided via mask ventilation for 1 min. If significant bleeding and discharge were occurred, suction was performed. Even if the time was within 2 min 30 s, if the oxygen saturation level dropped below 95%, then 100% oxygen manual ventilation was performed. The first two attempts were performed by the same operator. After two failed attempts, a specialist intervened and performed the intubation. If bleeding was severe or too much time had passed, then nasotracheal intubation was performed using laryngoscope and Magill forceps. The resident's failure after two attempts was evaluated as a failed case [5].
2.5. Measurement of nasal bleeding
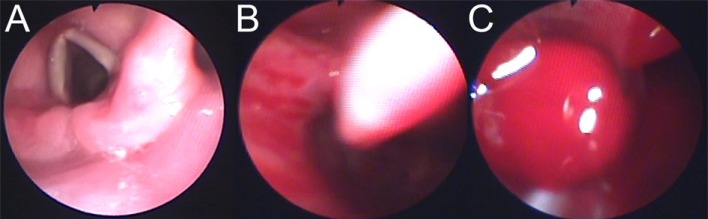
The degree of nasal bleeding during nasotracheal intubation with fiberscope was measured by the degree of visibility: grade 1 no bleeding (no interference with securing the visual field); grade 2 mild bleeding (the degree of bleeding that did not influence the visual field); and grade 3 massive bleeding (the degree of bleeding that influenced the visual field) (Fig. 1). If too much bleeding and discharge were occurred, suction was performed by the assistant.
2.6. Learning curve analysis method
Patient sex, age, weight, height, and the size of the tube were recorded. For each patient, the time required for FNI by the resident and the degree of bleeding observed with endoscope were also recorded.
The times recorded as required time for FNI were depicted as a learning curve, and the ratio of FNI success and failure cases were evaluated. For awake FNI, success was evaluated separately. The success rate was analyzed by dividing into several intervals based on the sum of 5 trials. The effect of nasal bleeding on the degree of difficulty was determined, and logistic regression analysis was used for comparative analysis of the influence of awake status, degree of nasal bleeding, and increased FNI trials on the success rate of intubation.
Depending on the situation, the chi-squared test, Student's t-test, and logistic regression analysis were performed for analysis, and a P < 0.05 was considered to be statistically significant.
Go to :
RESULTS
A total of 18 second-year anesthesiology residents (11 men, 7 women) were included in the present study. The age of the residents were 27 (n = 10), 28 (n = 4), 29 (n = 1), 30 (n = 2), and 31 (n = 1) years.
All residents performed a total of 716 FNIs, in which 15 residents performed the procedure 40 times, 2 performed it 39 times, and 1 performed it 38 times. Awake FNI was performed a total of 44 times (mean 2.4 times), in which 2 residents performed it 5 times, 3 residents performed it 4 times, 3 residents performed it 3 times, 6 residents performed it 2 times twice, 1 resident performed it once; 3 residents were not able to perform the maneuver at all (Table 1).

Table 1
Patient characteristics
![]()
The success rate was 88.3% for the first attempt and 94.6% for the second attempt. The failure rate was 4.9% in anesthetized patients and 13.6% in awake patients (Table 2).

Table 2
Success rate of fiberoptic nasotracheal intubation (divided by awake intubation and postanesthesia intubation)
![]()
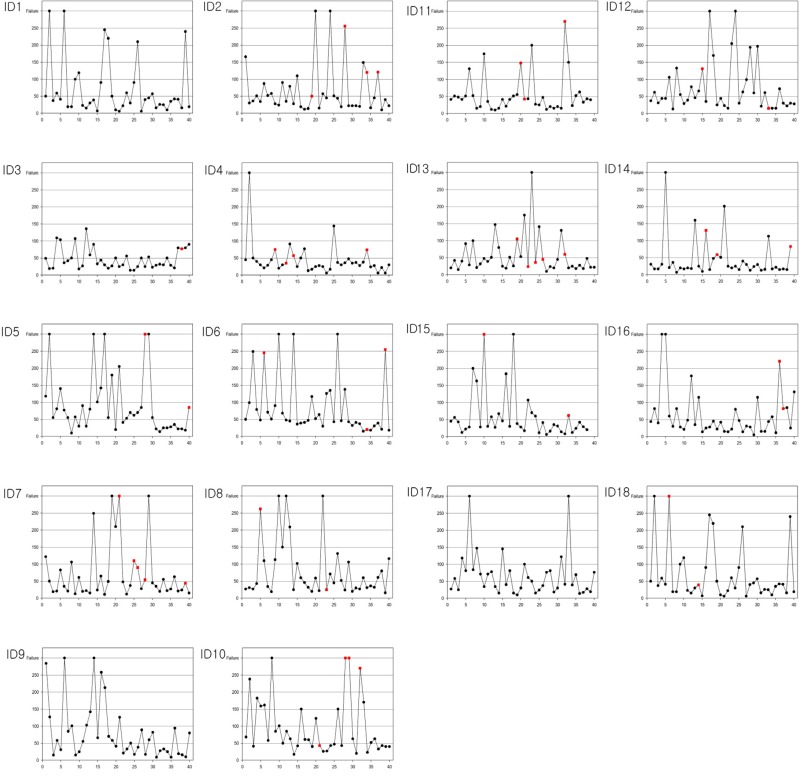
Time for each successful intubation for each resident was represented as a learning curve (Fig. 2). Analysis of the learning curves revealed that improvement was observed as the number of attempts increased. The learning curves exhibited diverse patterns, in which some showed frequent failures in the beginning, interim and end, some had a high interim failure rate, and some had a steady success rate from beginning to end.
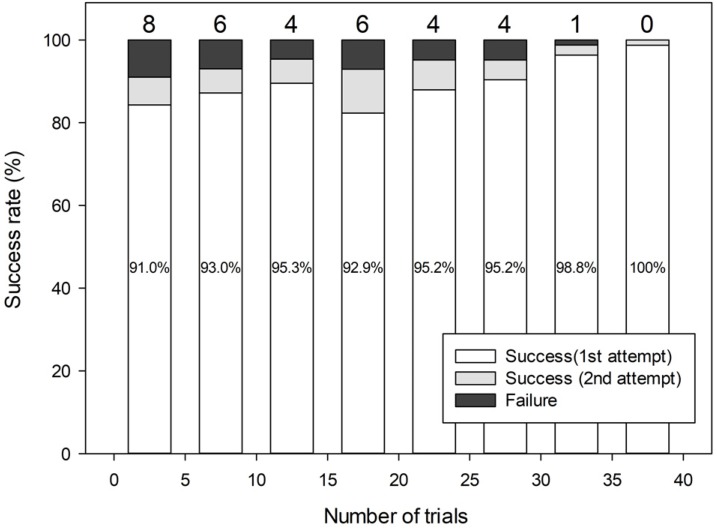
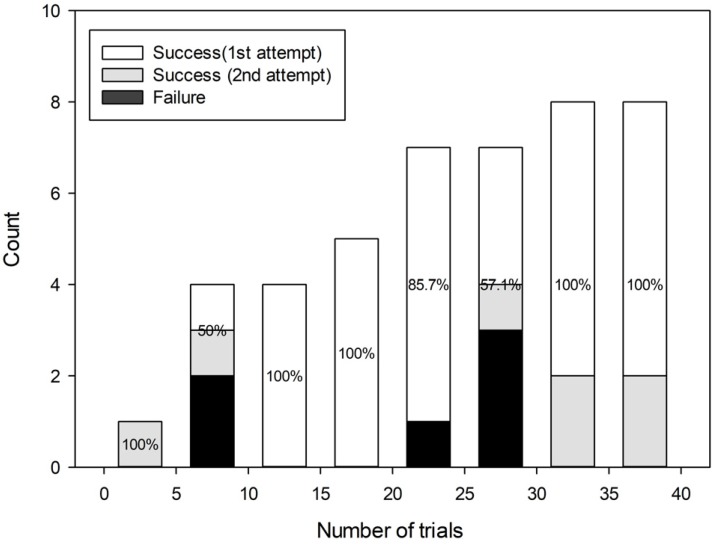
In terms of the mean time to successful performance, the mean time was 53.8 ± 47.4 s for anesthetized intubation and 103.2 ± 79.8 s for awake intubation, demonstrating a difference in time to successful intubation depending on awake status (P = 0.001) (Fig. 3). When analyzing the cumulative success rate by dividing by 5 trial intervals, the failure rate up to the first fifth post-anesthesia intubation was 9.0%, and the failure rate decreased to 0.7 % when the total performance number was > 30 (Fig. 4). Even for awake intubation, the failure rate was 0% when performed > 30 times (Fig. 5).
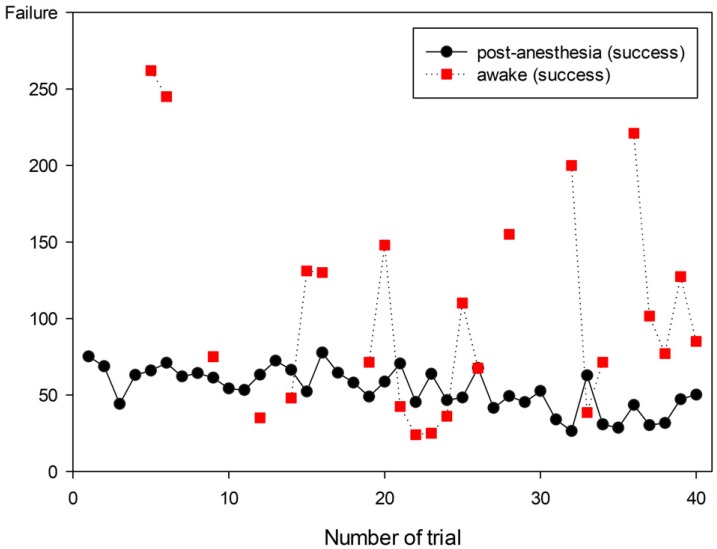 | Fig. 3Plot of average time in cumulative trials in successful cases (divided by awake intubation and post-anesthesia intubation).
|
When nasal bleeding was severe, the failure rate increased to 30% when FNI was performed while awake (Table 3) (P < 0.001 chi-squared test). According to logistic regression analysis, awake status, degree of nasal bleeding, and the number of attempts for nasotracheal intubation had an influence on the intubation success rate and, among them, nasal bleeding was the factor with the most influence (Table 4).

Table 3
Influence of nasal bleeding on the success rate of flexible endoscopy
![]()

Go to :
DISCUSSION
The results of this study demonstrated that the success rate of intubation and awake FNI increased as the number of attempts increased. However, when bleeding occurred as the endotracheal tube was inserted, the difficulty of FNI increased.
In patients for whom endotracheal intubation is expected to be difficult, awake intubation using fiberscope has been presented as the standard method of airway management [2]. However, to proficiently perform intubation using fiberscope without complications, significant training and performance experience are needed [6].
For new residents, the FNI learning curve for a normal airway simulator showed that it converged to 51 seconds to reach the carnia from the nostril and that the number of trials required for proficient intubation performance varied from 27 to 58 [7]. For oral intubation, the first attempt required 4 minutes, but it fell to 1.53 minutes after 10 trials, with a success rate > 95% [8]. Another study reported that when fiberscope was first inserted to nasal cavity, followed by nasotracheal intubation, the intubation time was approximately 50 seconds in 12 residents who performed intubation 20 times [5]. In the present study, the mean performance time for anesthetized FNI was 53.8 ± 47.4 seconds and that of awake FNI was 103.2 ± 79.8 seconds, yielding similar results.
An American Society Anesthesiologists Closed Claims Study collected data on adverse respiratory events from the 1980s and found that improper ventilation accounted for 38%, esophageal intubation for 18%, and difficult endotracheal intubation for 17% of the adverse respiratory events [9]. According to data collected after the 1990s, esophageal intubation has decreased significantly to less than 5%; however, difficult endotracheal intubation remains an important issue, at 27% [10].
Adverse respiratory events mainly occur during anesthesia induction, [11] and two failed attempts at intubation into the airway has been associated with hypoxia, arrhythmia, cardiac arrest, brain damage and death. Therefore, the competence of the operator is related to the incidence of adverse respiratory events [12].
The use of a fiberscope is a highly successful method in patients for whom securing the airway is difficult. Even if the laryngeal view of laryngoscope is poor, a fiberscope inserted up to the carina can be a guide for the endotracheal tube to appropriately position within the trachea, and the position can be confirmed while the fiberscope is removed. A previous study reported that among patients for whom intubation was impossible with the usual method, more than 90% showed success with fiberscope [13].
Many methods of local anesthesia for the airway are available for awake FNI, and the authors have chosen a highly stable and noninvasive lidocaine nebulizer [1415]. In addition, an appropriate amount of midazolam and fentanyl were administered when inserting the fiberscope to reduce airway reflexes and to safely maintain natural ventilation [16].
Endotracheal intubation generally uses a laryngoscope, and the degree of difficulty is evaluated based on the laryngeal view grade established by Cormack and Lehane [17]. In addition to cases with a high Cormack and Lehane's laryngeal view grade, a flexible endoscope can be useful in cases with difficulty in securing the airway due to poor cervical extension, short thyromental distance, and modified Mallampati test [1819].
The correlation analysis between the degree of difficulty of flexible laryngoscope intubation and the laryngeal view grade revealed that laryngeal view grade had no effect on the degree of difficulty [20]. Results of this study demonstrate that excessive bleeding and discharge are the most significant disadvantages interfering with the visual field of laryngoscope, making intubation difficult [21]. Therefore, to increase residents' success rate in FNI, reducing intra-oral bleeding and discharge are important.
Intra-oral and nasal cavity discharge can be reduced using antisialagogues such as glycopyrrolate [22]. Nasal bleeding occurs commonly during nasotracheal intubation when endotracheal tubes with large diameters are used, when too much force is applied during tube insertion, or when multiple attempts at intubation are made [23]. Many studies have investigated methods to reduce nasal bleeding, such as using a siphon as a guide at the tip of the tube [2425], softening of the tube by immersing it in warm water [25], and applying epinephrine [26]. In addition, the presence of systemic diseases associated with major bleeding disorders should be screened through patient history taking, and the appropriate nostril for intubation should be selected through physical examination [121]. Insertion of a flexible laryngoscope into the nasal cavity first was one method to reduce the frequency of nasal bleeding when performing FNI [27]. In this study, however, the purpose was to train residents for FNI in cases of unexpected difficult airway during nasotracheal intubation. Thus, methods of inserting the tube into the nasal cavity first were pursued.
In conclusion, even with some nasal bleeding, the success rate of FNI was found to increase with residents' FNI proficiency.
Go to :
 XML Download
XML Download