

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dementia, which is one of major neurocognitive disorders (MNCD), is a non-congenital cognitive disorder characterized by speaking difficulty and reduced memory, problem-solving ability, and ability to carry on with daily living, as well as loss of socio-occupational functions over time [12]. The most common cause of dementia is Alzheimer's disease (AD) (60-80%), and other causes include vascular (10%) and traumatic brain damage as well as systemic diseases, such as Parkinson's disease [2].
The level of disability for dementia patients increases with increasing duration of disease, and patients with severe disease eventually lose the ability to adequately perform oral hygiene on their own, which increases the risk for caries or periodontal diseases [3]. Furthermore, these patients have difficulty in describing their symptoms after developing oral problems, and even if they visit a dentist, the difficulty in communication hinders effective treatment [45]. As patients with MNCD are largely uncooperative, performing appropriate oral examination is challenging, and due to the risks and difficulty of local anesthesia, intravenous sedation (IVS) or general anesthesia (GA) are generally needed [6].
Dental treatment under GA enables dentists to effectively treat patients because they are immobile. Furthermore, safety may be improved by using appropriate doses and treatment based on a pre-procedural assessment of patient's systemic disease status and dental treatment-related risks [7]. In addition, dental treatment usually involves outpatient general anesthesia, which allows patients to receive all necessary dental treatments under GA in one day and return home on the same day, thus avoiding any inconveniences and saving costs and time involved in visiting the clinic multiple times [8].
However, this group of patients is older in age and has multiple comorbidities, which increases the risk of complications of GA, including reduced cardiopulmonary functions [9]. Furthermore, preoperative tests cannot be adequately performed because patients tend to be uncooperative. Anesthetic management for patients with AD is not familiar with the anesthesiologist due to the scant number of reports on outpatient anesthesia [10]. In this article, this study aims to analyze data on dental care under outpatient GA or IVS for AD patients at the Seoul National University Dental Hospital (SNUDH), in an attempt to contribute to effective outpatient anesthesia management for severe AD patients.
METHOD
This study was approved by the Institutional Review Board (IRB-No S-D20170049). Medical records of AD patients who were treated under outpatient GA or IVS at the Special Care Clinic of the SNUDH between January 1, 2012 and November 30, 2017 were obtained and analyzed.
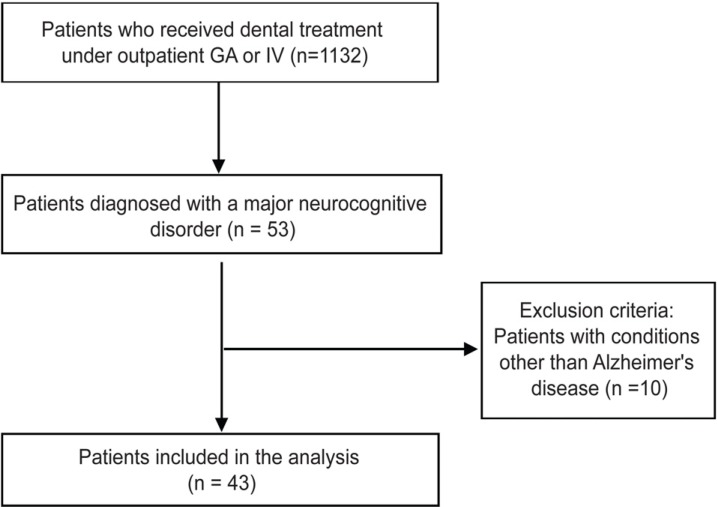
After analyzing the outpatient anesthesia list, we excluded patients with MNCD caused by cerebrovascular dysfunction, such as cerebral infarction, hemorrhage, patients with brain tumor, and searched for patients who were only diagnosed with AD at neurology. Patients with incomplete medical records were excluded from the analysis (Fig. 1).
In the hospital's electronic medical record database, we also analyzed each patient's dental treatment record, pre-anesthesia assessment record (sex, age, duration of Alzheimer's disease or dementia, current stage, and type of comorbidity), anesthesia and recovery room records (drug used for anesthesia induction, cooperation, airway management, total duration of anesthesia, duration of stay in the recovery room, and side effects and complications observed in the recovery room), next-day follow-up record data by phone (presence of complications after returning home), dental treatment details and duration of dental care. In addition, we investigated any differences in relation to the type of anesthetic used as well as between GA and IVS.
Vital sign data(blood pressure (BP), ECG, oxygen saturation, and capnography) during anesthesia that were monitored at five-minute intervals (Sola 8000M, GE, USA) and relayed to the hospital's server were used for analysis. Bispectral index (BIS, USA) and target-controlled infusion (TCI) data were obtained from electronic medical records, which were manually written based on the number shown on the infusion pump (Fresenius Orchestra, Fresenius Kabi, Germany).
For data analysis, each category was presented as the number of patients or procedures, and where necessary, as mean and standard deviation or number with percentage. With regard to medical history records, missing records or incomplete records were excluded, and only well-recorded data were included in the analysis.
RESULTS
1. Pre-anesthesia evaluation
Of 1,132 adult patients who received dental treatment under GA or IVS at the Special Care Clinic of the SNUDH during a period of six years from January 2012 to November 2017, 43 (3.8%) were AD patients. GA for dental treatment was performed in 32 of these AD patients, while IVS was performed 11 patients. One patient received four rounds of dental treatment, and six patients received two rounds of treatment; all the remaining patients received only one dental treatment. The mean age of the patients was about 70 years, and the mean duration of AD was 6.3 years. It took about 70 days from the first examination at our hospital to dental treatment under outpatient anesthesia (Table 1).
The severity of disease in the patients who underwent GA or IVS was assessed using the global deterioration scale (GDS) [11] based on the patients' attitudes and caregivers' statements on the day of the first examination. Twenty-seven patients had a moderately severe dementia (level 6) or higher, accounting for 62.8%. Ten out of a total of 43 patients were taking anti-hypertensive drugs, and there were three patients with diabetes, eight patients with Parkinson's disease, and two patients with a respiratory disorder. None of the patients had a severe disease that would contraindicate GA. A total of 38 out of 43 patients were classified as American Society of Anesthesiologists (ASA) physical class 2 (81.8%), and five patients were classified as ASA class 3 (18.2%).
Thirty patients underwent blood laboratory tests, electrocardiogram (ECG), and chest X-ray prior to surgery. However, three patients, who displayed needle phobia who had no notable findings in past health examinations or neurological tests, underwent blood tests on the same day after induction of anesthesia.
The method of anesthesia was usually determined based on the patient's state and treatment plan. The Alzheimer GDS level and the proportion of comorbidities were greater in patients who we determined should undergo treatment under IVS than those undergoing GA (Table 2).
2. Anesthesia induction and maintenance
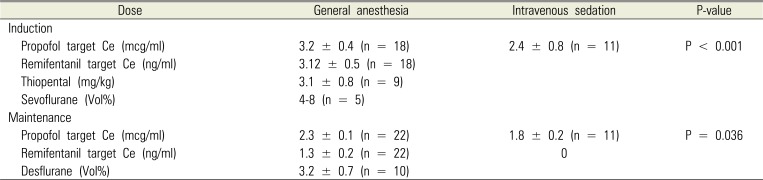
Cooperation during induction was assessed by the anesthesiologist on the day of the treatment. In most cases, the anesthesiologist was able to start an intravenous (IV) catheterization without coercive physical restraints (cooperative grade 1, and 2, 81.3%). However, 14 patients who were assessed to be cooperative had severe dementia (Alzheimer GDS level 7) and were incapable of resisting or responding to the attempted treatment (Table 3) [12]. For five patients for whom IV catheter insertion was difficult due to poor cooperation, anesthesia was induced via inhalation of sevoflurane. For all the patients who underwent IVS, sedation was induced and maintained via target-controlled infusion (TCI) with propofol. For 18 of the patients who underwent GA, anesthesia was induced via TCI with propofol and remifentanil, and maintained via total intravenous anesthesia (TIVA). For four patients who received sevoflurane for induction of anesthesia, anesthesia was maintained with TIVA, and for ten patients, including nine patients for whom thiopental was used for induction, anesthesia was maintained with desflurane. When propofol was used, the induction dose was significantly different between those who underwent GA and those who underwent IVS, where the induction dose was significantly higher for patients who underwent GA (P < 0.001) (Table 4).
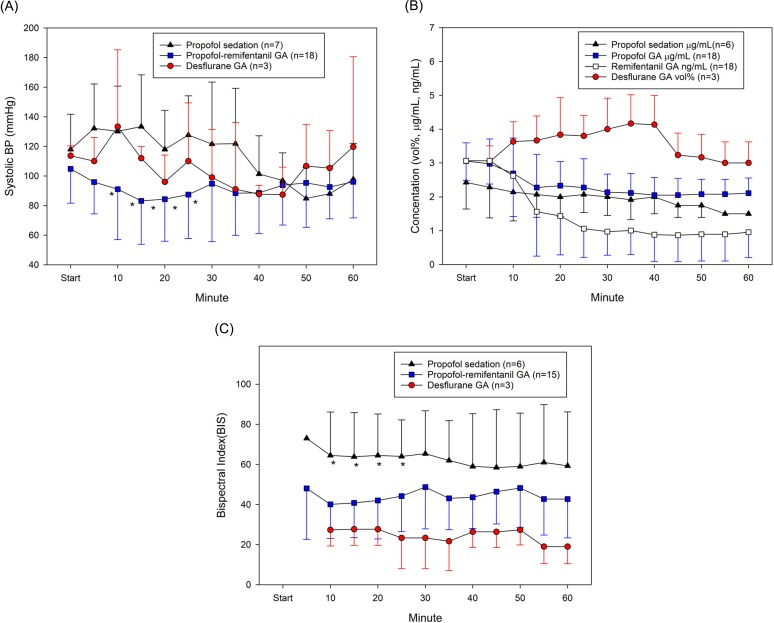
With GA, the airway was maintained through nasotracheal intubation. One patient had a difficult airway, for whom a fiberscopic intubation was performed. For a patient with IVS, O2 was administered via a nasal cannula at 2 L/min. The degree of sedation was confirmed with BIS, and propofol concentration was adjusted accordingly. Treatment was performed in a deep sedative state where the patient is unconscious. Among patients who underwent GA, inotropic agents (e.g., ephedrine) were administered due to a severe drop of BP in eight patients, and four patients needed anti-arrhythmics due to severe bradycardia or tachycardia. BP and pulse rate were relatively stable in patients who underwent IVS. BIS was maintained below 60 for patients undergoing GA and between 60-80 for patients undergoing IVS (Fig. 2).
3. Anesthesia Recovery
The duration of anesthesia with GA was twice that of IVS. After the completion of surgery, administration of the anesthetics was stopped, and recovery of consciousness and spontaneous breathing were confirmed before extubation, after which the patients were transferred to the recovery room. This took about an average of 18 min, whereas it took about 13 min for patients who underwent IVS to recover consciousness. In the recovery room, the patients were confirmed to have recovered to their pre-anesthesia states and to have stable vital signs before discharge. The duration of stay in the recovery room differed by about 20 min between the GA and IVS groups (Table 5). During recovery, postoperative delirium (POD) was not observed, and there were no complications requiring hospitalization. Fifty percent of the patients returned to a long-term care hospital, while the remaining 50% of the patients returned to their homes. When returning home, 75% of the patients used their own cars, 15.7% used an ambulance, and 9.3% used a taxi. At the time of returning home, 11.6% were in a drowsy state; however, the remaining patients had recovered their pre-anesthesia states. About 5% of the patients stated that they slept longer than usual on the first day after returning home, and there were no cases of nausea or vomiting. During an over-the-phone check-up the next day, five patients complained a mild fever and three had persistent oozing at the extraction site; however, none of the patients developed complications requiring a hospital visit.
4. Dental Treatment
The most commonly performed dental treatment for AD patients was tooth extraction (92.7%) and caries treatment (43.9%). The mean number of extracted teeth among the patients who received tooth extraction was 5.9 ± 4.9. The mean number of dental caries among the patients who underwent caries treatment was 3.4 ± 2.1.
DISCUSSION
The worldwide prevalence of dementia is about 5–7% of the elderly population aged 60 years or older, and at the current growth rate, the prevalence is estimated to double every 20 years [13]. In South Korea, about 9.2% of the elderly population aged 65 years or older have dementia, and the prevalence rises with advancing age [14].
Although the exact cause of Alzheimer's AD has not yet been elucidated, a mutation of the amyloid precursor protein gene located in chromosome 21 is known as the cause of early-onset familial Alzheimer's disease, in which dementia develops before the age of 65 years. A mutation of the presenilin 1 gene in chromosome 14 as well as a mutation of the presenilin 2 gene in chromosome 1 are also known as some causes of AD [15]. With regard to dementia that sporadically appears after the age of 65, the apolipoprotein E4 allele in chromosome 19 is known to be a risk factor. AD is a syndrome caused by an interaction of progressive neurological degeneration, genetic risk factors, and environmental risk factors, as opposed to a disease caused by a single specific cause. AD patients demonstrate behavioral changes, including disordered cognitive functions and irreversible memory disturbance, delusion, reduced social adjustment, verbal disability, walking difficulty, and reduced motor coordination similar to that of Parkinson's disease [16].
The treatment trends at our hospital show that the annual number of cases receiving treatment is rising; however, the treatment is generally focused on tooth extraction and caries treatment. As AD progresses, oral health is exacerbated, particularly, the prevalence of periodontal diseases is reported to be higher among AD patients compared to the healthy population, and dental caries is known to proportionately rise with the degree of exacerbation of dementia symptoms [17]. Furthermore, drugs that are taken to mitigate neurological symptoms not only increase dental caries but also may cause mucositis, gingival hypertrophy, and intraoral ulcer [18]. Such poor oral health and increase in oral diseases induce pain and discomfort, and changes of swallowing habits may have a toll on self-esteem. Therefore, appropriate dental intervention is essential for AD patients to lower pain and oral diseases and maintain adequate oral health. This would in turn improve quality of life and hinder worsening of oral states in the later stages of dementia [19].
However, dental treatment for moderately to severe AD patients must be performed under IVS or GA because these patients have no insight into their dental diseases and demonstrate poor cooperation [6]. Treatment under IVS or GA is performed while the patient's movements are reduced or eliminated, so quality dental care can be provided irrespective of the patient's cooperation. Furthermore, the amount of treatment that can be performed in one session as well as the time of one session of treatment can be increased, resulting in fewer hospital visits. In addition, patients do not have to undergo a painful or bad experience, as the treatment is performed while the patient is unconscious, which helps patients maintain a positive attitude toward future dental treatments [8].
Anesthesia for AD patients must be performed in adherence to the geriatric standards and with extra precaution, as most AD patients are older adults. The most well-known and confirmed risk involved with GA in relation to AD is age and not AD per se [20]. Patient safety can be enhanced by using appropriate doses and providing appropriate treatment based on a preanesthesia risk assessment by the anesthesiologist. Ten out of the 43 AD patients referred to our hospital (23%) had hypertension, which was in line with the hypertension prevalence in South Korea (22.9%) [21].
The anesthesia method was determined based on the patient's general condition and comorbidity, amount of time needed for dental procedure, and type of techniques used. The durations of anesthesia and procedure were significantly shorter for IVS in our hospital, and this may be attributable to the following factors. First, even though there is no underlying disease, a reduction of functional capacity is a predictor of postoperative pulmonary complications [22], and patients with Alzheimer GDS level 7 fall under this category. Second, aspiration pneumonia is one of the most common causes of mortality among patients with late stage AD, primarily because of reduced consciousness, dysphagia, loss of the gag reflex, and periodontal disease [23]. Prolonging IVS for dental treatment for patients with reduced Gag reflex has no benefits for the patients. When one IVS session was insufficient to complete treatment, we had the patients visit the hospital several times to complete the treatment. GA was performed for patients who could not visit the hospital several times, who were scheduled to undergo a large number of dental extractions, who were in needed of adequate muscle blockade to be treated in the molar region, or who required an analgesic other than propofol due to a temporomandibular joint disease.
Overall, vital signs were maintained at a stable level. but vital sign changes were observed in the 1 hour interval after induction. This was not related to the presence or absence of underlying disease in the patients and occurred in general anesthesia using TIVA (6 out of 8 cases). In GA, propofol requires a higher induction dose than IVS, which can cause a drop in blood pressure and tachycardia. Autonomic dysfunction is accompanied in patients with AD or dementia [24], implying the possibility of excessive hemodynamic change due to drug response. With regard to the correlation between the chosen drug and SBP in TIVA, there is a possibility that the drop in SBP may be inversely proportional to the concentration of remifentanil. Remifentanil is quickly degraded by esterase in blood and tissues; however, the level of esterase declines with aging, with a decrease of about 30% at the age of 80. The volume of distribution also decreases by about 20%, which leads to a higher peak concentration compared to that in younger adults. Further, extra precaution is demanded when bolus-injecting remifentanil, as it may induce severe hypotension and bradycardia [25]. During TIVA, a high-dose drug is injected at the early stage to achieve the initial effect-site concentration, after which the dose is reduced, and this may cause side effects. In fact, when remifentanil is used, reduced blood pressure is maintained for a while even after adjusting the dose after the stimulus is lost. This may explain why inotropics were usually used during TIVA. Atropine, a medication for bradycardia, was also used only in TIVA cases, and patients in these cases are speculated to have developed opioid-induced bradycardia caused by remifentanil.
Inhalation or intravenous agents used for GA are predicted to be associated with AD at the tissue level in animal models [26]. However, there were no differences in maze-solving abilities or motor capacities from those of animal models without exposure [27].
Minimum alveolar concentration (MAC) is defined as “the minimum alveolar concentration of anesthetic at 1 atmosphere that produces immobility in 50 per cent of those patients or animals exposed to a noxious stimulus,” and surgical incision is generally the stimulus in humans. Human studies have reported that aging is associated with a reduction in the MAC. Patients with reduced consciousness due to a brain injury require a lower amount of inhalation anesthetics [28]. However, in animal studies, the presence of pathological changes, that is, neuropathology such as AD, was predicted to induce resistance to hypnotic action caused by inhalation anesthetics [26].
The MAC in the 40-yr-old of sevoflurane and desflurane is 2 and 6 vol%, respectively. According to the formula suggested by Nickealls et al., the The MAC in the 70-yr-old (average age of our patients) of desflurane is 4.98 vol% [29]. The average amount of desflurane used in our hospital was 3.2 vol% ± 0.7. This is a markedly lower concentration than those reported in previous studies, and additional studies are needed to substantiate whether AD patients demonstrate resistance to inhalation anesthetics.
According to the study by Schultz, electroencephalogram (EEG) during total intravenous anesthesia (TIVA) seems to be affected by age. The amount of propofol required while anesthesia is stably maintained is also smaller than that in younger patients, and recovery was also slower [30]. This is correlated with our finding that while the maintenance dose for propofol and desflurane was lower than the generally known maintenance dose, BIS was maintained at 40–60, which is the level for maintaining GA.
When using GA for treatment purposes in AD patients, the benefits of GA must be prioritized over the risks that have not been established. However, it is necessary to avoid low body temperature and isoflurane, which were confirmed by many studies to have an impact [31].
None of our patients showed postoperative delirium (POD) during recovery. Delirium was defined as an acute change in cognition characterized by inattention, fluctuating levels of consciousness, and/or disorganized thinking. In non-cardiac surgeries, the predictors of POD include cognitive disorder, age of 70 years or older, reduced physical capacity, alcoholism, and abnormal blood test results such as electrolyte abnormality [32]. These risk factors are in common with AD patients' conditions, so AD patients are predicted to have a high risk for POD. Intravenous or inhalation anesthetics must be used carefully because mental confusion may be exacerbated in AD patients after administering sedatives or anesthetics [33]. However, this was not the case at our hospital, presumably because of our aggressive nondrug prevention strategies [32]. The primary caregiver was told to stay with the patient from the first recovery room, and a warm environment with appropriate lighting was provided. Hearing aids were provided when necessary. For patients who had their teeth extracted, non-opioid analgesics were provided to control pain if not particularly prohibited. We believe that these factors contributed to the prevention of POD at our institution.
One limitation of this study is that although we collected data from dementia patients for five years, our sample size was below 50. However, we expect to gain more experience in several years based on the current rate of new dementia patients. Furthermore, as with other retrospective studies, our analyses may not be strict due to missing values caused by incomplete medical records data.
Outpatient anesthesia care for AD patients has rarely been studied in the literature. Moreover, this was a great challenge for anesthesiologists, as AD patients are known to have a high risk for POD. There may also be a vague fear of encountering multiple underlying diseases due to the old age of patients. However, based on our experience of performing outpatient anesthesia, patients with AD-type dementia did not particularly have a greater number of comorbidities compared to the general population and also did not develop POD.
In conclusion, this study finds that using smaller drug doses and providing adequate anesthetic management would prevent hazards to AD patients undergoing IVS or GA. Although oral health examination is difficult for AD patients, we believe that their oral health has improved with anesthesia consultation.




 XML Download
XML Download