

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bronchospasm is a rare but serious complication in patients undergoing endotracheal intubation for general anesthesia [12]. This response is likely due to a neural reflex constriction in the airway smooth muscle [3]. Bronchospasm causes an increase in lung resistance and a decrease in lung compliance [345], eventually making it difficult to provide effective mechanical ventilation.
Efforts to minimize the incidence of bronchospasm and peripheral airway constriction after endotracheal intubation are important, especially in patients with chronic airflow obstruction, including asthma and chronic obstructive pulmonary disease (COPD), because they are particularly at risk for bronchospasm under general anesthesia.
Tulobuterol patches (TPs) are transdermal β2-agonists useful for asthma and COPD patients [6789]. Although tulobuterol is a short acting β2-agonist, a TP exerts continuous bronchodilatory effects with a sustained serum concentration elevation for 24 h [1011].
We hypothesized that the use of a TP prior to general anesthesia would help to reduce the risk of bronchospasm after endotracheal tube placement in patients showing preoperative chronic airflow obstruction. The purpose of the present study was to determine the bronchodilatory effect of a TP for the prevention of bronchospasm during the induction of general anesthesia.
Go to : 
METHODS
This study was approved by the Institutional Review Board of the hospital and was registered with the Clinical Research Informational Service (KCT0001152, http://cris.nih.go.kr). Written informed consent was obtained from all patients.
Eighty-two American Society of Anesthesiologists (ASA) category I or II non-smoking adult patients undergoing minor elective surgery were enrolled in this prospective randomized study. They showed a forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) ratio < 70% in preoperative pulmonary function tests, suggesting chronic airflow obstruction [12]. Patients who used β-blockers, β2-agonists, steroids, and other bronchodilatory treatment, or who had a history of COPD exacerbation in the previous 4 weeks, were excluded. The sample size was estimated from preliminary data from ten patients. Power analysis suggested 34 patients per group with a power of 80% at α-error of 0.05 to detect a difference in airway resistance (Raw) at 5 min after endotracheal intubation for 2 cmH2O/L/sec. To compensate for potential dropout, we recruited 41 patients per group. Patients were randomly assigned to one of two groups using computer-generated random numbers. The tulobuterol patch group patients (TP group, n = 41) received a 2 mg tulobuterol patch applied to the skin of the chest on the night before surgery. The patients in the control group (n = 41) did not receive a drug-containing patch.
All patients were pre-medicated with midazolam 0.04 mg/kg intramuscularly 1 h before anesthesia induction. In the operating room, after confirming the TP attachment, standard monitors were attached. Anesthesia was induced and maintained using a target-controlled infusion device (Orchestra; Fresenius Kabi, Bad Homburg, Germany) with propofol (target effect site concentration, 4 µg/ml) and remifentanil (target effect site concentration, 2 ng/ml). Endotracheal intubation was performed using a 7.5–8 mm diameter cuffed tube with rocuronium 0.6 mg/kg for muscle relaxation. Mechanical ventilation was started as quickly as possible. The ventilator was set to maintain a tidal volume of 8 ml/kg, 10 breath/min, fresh gas flow 4 l/min, oxygen-air (fraction of inspired oxygen, 0.5), and an inspiratory to expiratory ratio of 1:2.
Mean arterial blood pressure (MAP), heart rate (HR), and SaO2 were recorded before induction and three times every 5 min after endotracheal intubation. Simultaneously, end-tidal carbon dioxide (EtCO2), airway resistance (Raw), and dynamic lung compliance (Cdyn) were determined 5, 10, and 15 min after intubation. These two respiratory variables were measured using a non-invasive cardiac output (NICO) monitor (Respironics-Novametrics, Wallingford, CT, USA) which was placed between the endotracheal tube and the corrugating tube. SPSS 17.0 (SPSS, Chicago, IL, USA) was used for statistical analyses. Data were expressed as the mean ± SD. The demographic data were compared using the student's t-test and the chi-square test. All continuous variables were checked for normal distribution with the Q-Q plot and the Kolmogorov-Smirnov test. Two-way analysis of variance (ANOVA) for repeated measures was used to analyze the effect of time and group. If significance was detected, multiple comparisons were evaluated using the Bonferroni correction. Statistical significance was set at 0.05.
Go to :
RESULTS
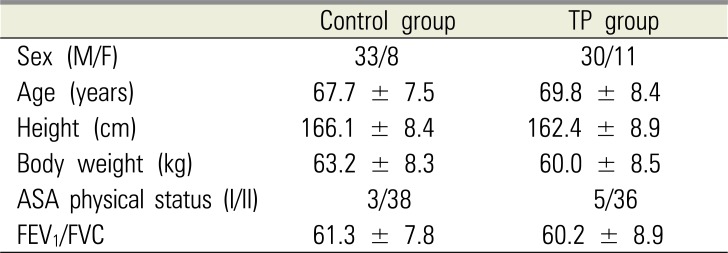
Throughout the study, neither group demonstrated any serious adverse cardiovascular side effects (palpitations or tachycardia), and all anesthetic inductions were performed safely, without any serious events. (Fig. 1) There were no differences in demographics, including sex, age, weight, height, and ASA physical status between the groups. No significant difference was observed between the groups in the preoperative pulmonary function tests (Table 1).
There was no difference in MAP, HR, SaO2, or EtCO2 between the two groups at any measurement points (Fig. 2). Within each group, the HR and SaO2 showed no significant change during the observational period. However, MAP was significantly different at 5, 10, and 15 min intervals after endotracheal intubation compared to before anesthesia induction (P < 0.01) in both groups (Fig. 2a). EtCO2 also showed a statistically significant difference at 10 min and 15 min, as compared to 5 min after endotracheal intubation (P < 0.01) in both groups (Fig. 2c).
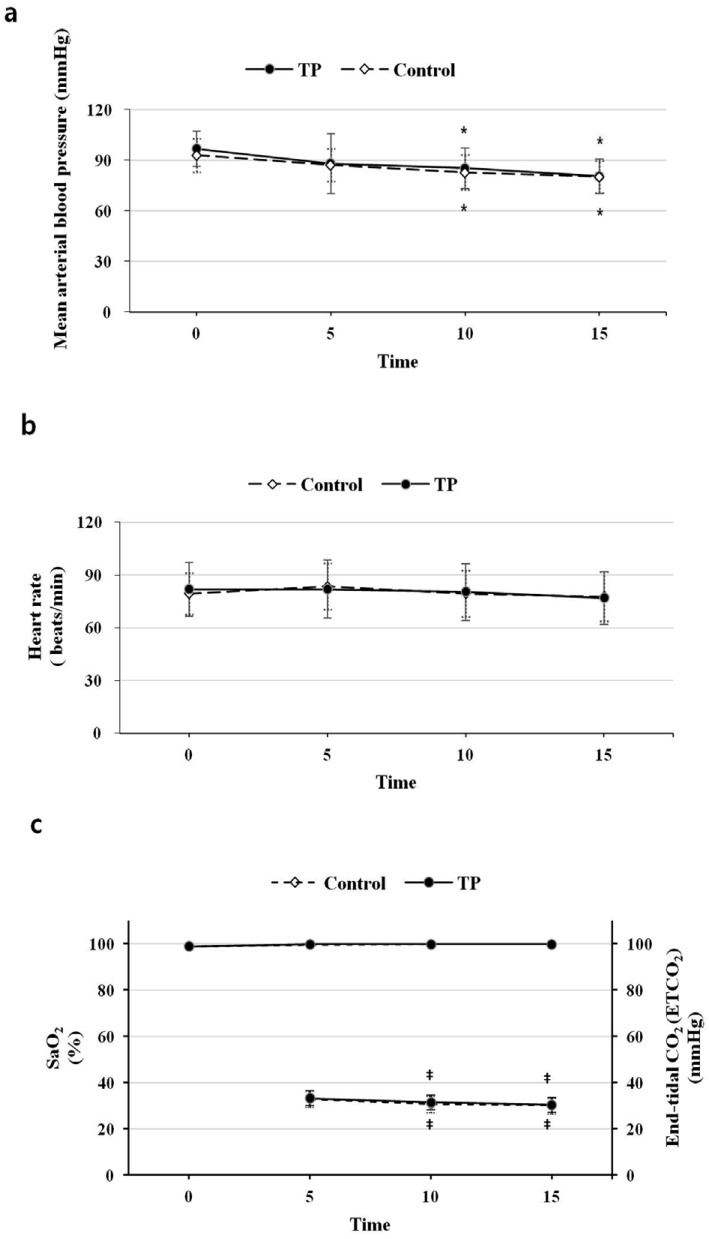 | Fig. 2Time numbers on the abscissas indicate the following: 0, before induction, and 5, 10, 15, 5 min, 10 min, 15 min after endotracheal intubation. Values are shown as the mean ± standard deviation. *P < 0.01 vs before induction within the group. ‡P < 0.01 vs 5 min after endotracheal intubation within the group.
|
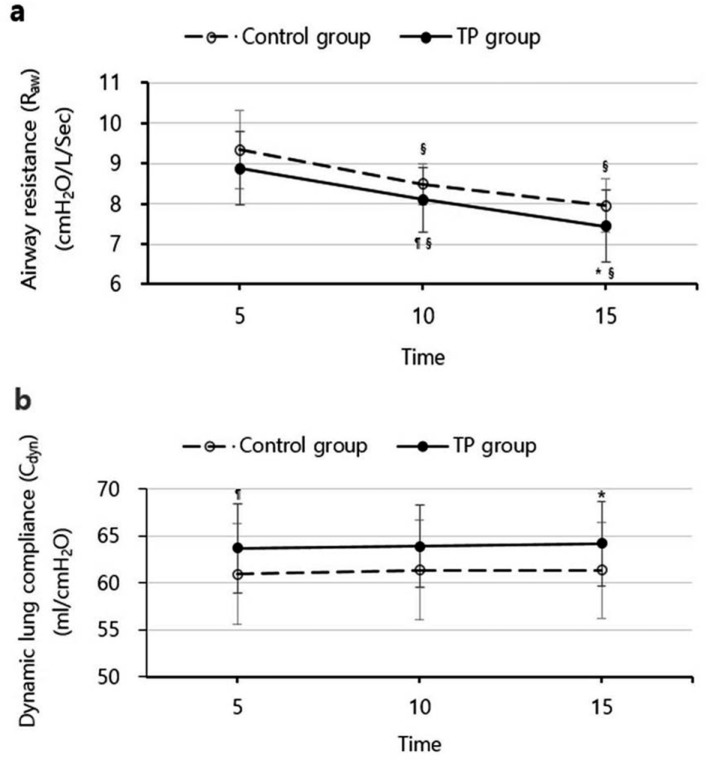
The TP group was associated with a lower Raw and a higher Cdyn, as compared to the control group. Raw was significantly lower at 10 min (P < 0.05) and 15 min (P < 0.01), and Cdyn was significantly higher at 5 min (P < 0.05) and at 15 min (P < 0.01) in the TP group (Fig. 3). A trend towards a lower Raw was observed and showed a statistically significant difference 5 min after endotracheal intubation (P < 0.01) in each group (Fig. 3a). In contrast, Cdyn showed no change 5 min after endotracheal intubation in either group (Fig. 3b).
Go to :
DISCUSSION
This study investigated the bronchodilatory effect of TPs for the prevention of bronchospasm after endotracheal intubation. Our hypothesis was that the bronchodilatory effect of a TP might affect airway resistance (Raw) and dynamic lung compliance (Cdyn), consequently reducing the risk of bronchospasm after anesthesia induction.
Numerous factors, including cold air, allergens, stress, and invasive ventilator devices, may cause bronchial smooth muscle contraction and eventually lead to bronchospasm [13]. In patients undergoing general anesthesia, cold inspired gases, laryngoscopy, and endotracheal intubation can provoke bronchospasm. Importantly, intraoperative bronchospasm is a rare but serious complication [12]. In this study, we enrolled patients showing an obstructive pattern in preoperative pulmonary function tests on the assumption that they had a bronchial hyperresponsiveness, such as asthma or COPD [14]. In these patients, the risk of bronchospasm increases with endotracheal intubation, as compared to normal patients. We measured two respiratory variables, Raw and Cdyn. An increase in Raw and a decrease in Cdyn could increase the possibility of bronchospasm and it has been reported that Raw is more sensitive than Cdyn to bronchospasm [15].
We used target-controlled infusion with propofol and remifentanil, instead of a volatile agent for anesthesia induction and maintenance, to minimize the influence of anesthetics on airway resistance. The bronchodilatory effect of a volatile agent, such as isoflurane or sevoflurane, may affect airway resistance [16], and there have been reports that desflurane may provoke bronchoconstriction in smokers [17]. For anesthesia induction, thiopental or etomidate may also be used. Although the possibility of bronchospasm cannot be precluded when using propofol, propofol is more effective in constraining increases in airway resistance [231819]. Simultaneously, we used rocuronium as a muscle relaxant, which is useful in asthma patients for rapid sequence induction, because some neuromuscular blocking agents, such as mivacurium and atracurium, have a histamine-releasing effect and may cause bronchospasm [20].
A TP is categorized as a long-acting β2-agonist and shows continuous bronchodilatory effects for 24 h with a low incidence of adverse effects [1011]. It has been used for the long-term treatment of asthma and COPD, and its benefits have been previously demonstrated [1121]. Compared to oral or inhaled tulobuterol, TPs maintain a stable serum tulobuterol concentration for a prolonged period [1022] and are simpler to administer. Nevertheless, transdermal absorption of the TP is slower than when tulobuterol is administered orally or inhaled. The time to maximum TP plasma concentration (Tmax) is between 9 h and 12 h, whereas the Tmax of inhaled tulobuterol is between 0.8 h and 1.5 h. At the dose used in our study (2 mg), Tmax was 11.8 h and the maximum plasma concentration (Cmax) was 1.4 ng/ml [10]. Considering the Tmax, we applied a TP on the night before surgery, because it was the optimal time to obtain a sufficient TP effect for all patients enrolled in the study. We hypothesized that a single TP application could attenuate the response to endotracheal intubation and improve airway obstruction in anesthetized patients, similar to other inhaled β2-agonists [4]. There are potential side-effects of β2-agonists, including hypokalemia, arrhythmia, and tachycardia, especially in elderly patients [232425]. However, at standard TP doses, such adverse effects are rare [821].
According to our results, Raw was lower at all measurement points in the TP group. However, Raw at 5 min after endotracheal intubation showed no statistically significant difference compared to the control group. It is possible that a 2 mg TP may not be sufficient to attenuate the response after endotracheal intubation completely. Alternatively, a TP may fail to reach Cmax in some patients. If we had applied a TP earlier, almost all patients would have been exposed for 12 h, reaching Cmax. However, earlier TP administration was not optimal in our hospital. In both groups, Raw at 10 min and 15 min was lower, as compared to 5 min after endotracheal intubation. This is likely due to the decrease in bronchial hyperresponsiveness rather than the TP. Overall, even though a high Cdyn value was recorded at all measurement points in the TP group, there was no statistically significant difference in Cdyn 10 min after endotracheal intubation. This may have been due to an unrecognized error.
In summary, our results suggest that a single TP application effectively suppressed the increase in Raw and the decrease in Cdyn without any severe adverse effects after anesthesia induction. The bronchodilatory effect of the TP may be helpful to reduce the risk of bronchospasm after endotracheal intubation.
Go to :
 XML Download
XML Download