

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pain is one of the most common complaints that patients present with at hospital [1]. Pain has several definitions that depend on the aim or scope. Mersky et al. [2] defined pain as “an unpleasant sensory and emotional experience with actual or potential tissue damage or described in terms of such damage.”. McAloon et al. [3] described pain as a subjective feeling or experience interpreted by oneself, while Gloss et al. [4] reported that pain is a complex and private experience. Briggs and Closs [5] highlighted that pain was also influenced by numerous intrinsic and extrinsic factors, and that multiple aspects of pain was assessed in different ways. Although no one interprets pain in exactly the same way, the intensity of pain depending on the patients' perception, should be assessed for effective pain management [3]. Pain perception depends on the pain threshold of each person, which might be used as a baseline to compare pain intensity.
The assessment of the intensity of pain and locating it is a routine procedure in clinical practice. Various tools have been developed for different types and subtypes of chronic pain conditions so that the effect of chronic pain on quality of life and the patient's function can be gaged [6]. The accuracy of pain assessment is very important to evaluate the appropriate treatment.
Pain intensity is the initial factor that point to its sensation and function. Therefore, pain measurement tools are used to help assess pain intensity, and monitor the effectiveness of and response to treatment decisions [7].
Multidimensional pain scales assess the following:
The aim of the current article was to provide an overview of pain measurements that are commonly used in OMFS research.
Go to : 
TYPES OF PAIN INTENSITY SCALES (Table 1)
There are multidimensional and unidimensional scales of pain. The following are multidimensional scales:
Unidimensional scales to assess pain are as follows:
1. Multidimensional pain scales
The intensity, nature, and location of pain can demonstrate its impact on the patient's activity or mood, and is useful to assess complex or persistent acute or chronic pain.
1.1. MPQ [8]
The MPQ, which was formulated in 1971 by Melzack and Torgerson., was first published in its complete form in 1975. As seen in Fig. 1 it measures several dimensions of the experience and intensity of pain experience and pain intensity [9]. The advantages of the MPQ are its reliability, validity, and its access to the multidimensionality of pain [9].
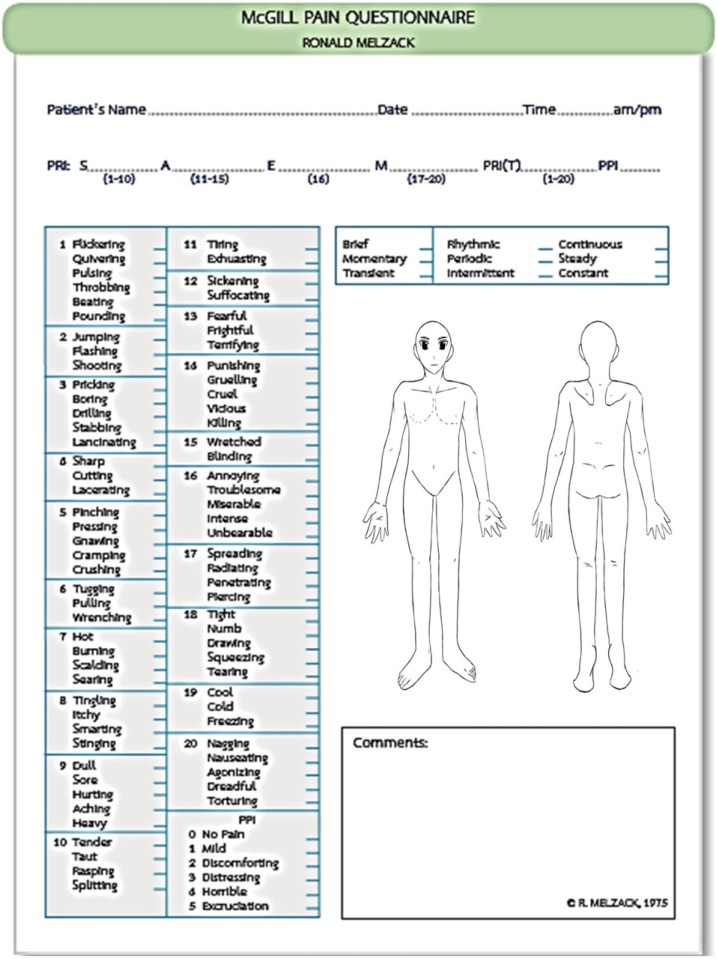 | Fig. 1Modified of McGill Pain Questionnaire. The McGill Pain Questionnaire. The descriptors fall into four major groups: sensory (S), 1–10; affective (A), 11–15; evaluative (E), 16; and miscellaneous (M), 17–20. The rank value for each descriptor is based on its position in the word set. The sum of the rank values is the pain rating index (PRI). The present pain intensity (PPI) is based on a scale of 0–5.
|
The major disadvantages of the MPQ include the following: very complex, requires tremendous patient compliance and endurance to fill the form, and takes up to 30 min, which can be tedious and time-consuming [3].
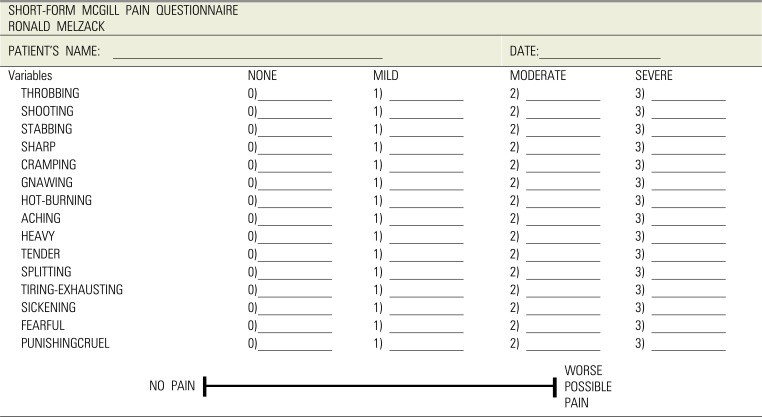
1.2. SF-MPQ (Table 2)
SF-MPQ is the alternative scale of the Present Pain Intensity (PPI) tool (Table 3). This scale only assesses the intensity of pain, and not its other qualities [10]. It was developed in 1980, when Melzack realized that the MPQ was too long [10]. This pain assessment scale turned out to be relatively easy, since it consisted of choosing the most commonly used sensory and affective descriptors in all clinical studies. Given its simplicity, it can be applied to assess mild, moderate, and severe cases. The SF-MPQ incorporates both the PPI and VAS, and thus, has the following five sub-scores: sensory, affective, total scores from the MPQ descriptors, overall intensity scores from the PPI, and the VAS [8]. The scales were ranked as follows:
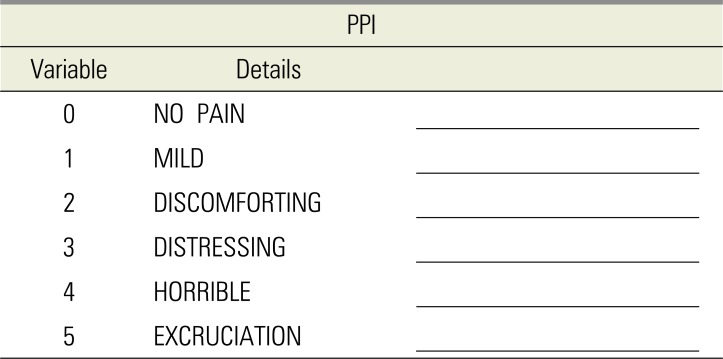
The PPI of the standard LF-MPQ and the VAS are also included to provide overall intensity scores.
Table 2
The short-form McGill pain questionnaire of Ronald Melzack [10]

![]()
1.3. BPQ (Table 4)
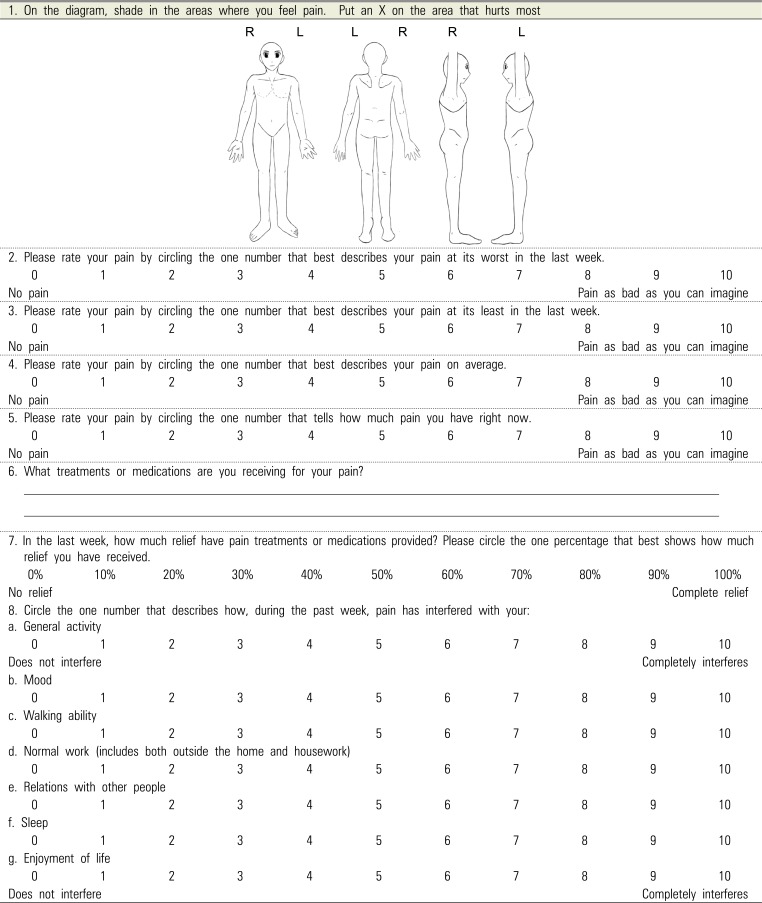
The BPQ is used to estimate the prevalence and severity of pain. It is easy to administer to a large numbers of patients, since it brief, can be self-administered, and easily determines the history, intensity, location, cause, quality, and interference with activities. However, the disadvantage is that given its brevity, it does not allow a comprehensive assessment of the pain course [11].
Table 4
The Wisconsin Brief Pain Questionnaire (modified of Wisconsin Brief Pain Questionnaire) [11]
Detail:
Brief Pain Inventory Scoring Instructions
1. Pain Severity Score: This is calculated by adding the scores for questions 2, 3, 4 and 5 and then dividing by 4.This gives a severity score out of 10.
2. Pain Interference Score: This is calculated by adding the scores for questions 8a, b, c, d, e, f and g and then dividing by 7. This gives an interference score out of 10.
Brief Pain Inventory from Hunter Integrated Pain Service Dec 2006
Reproduced with acknowledgement of the Pain Research Group the University of Texas MD Anderson Cancer Center, USA
![]()
2. Unidimensional scales
Most previous acute pain researches [5] used these pain measurement tool for only the sensory pain experience.
2.1. VAS
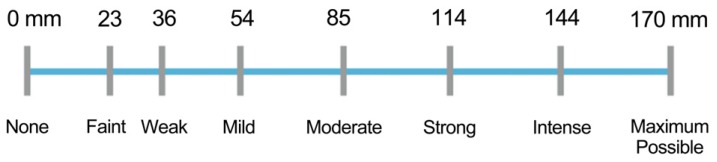
In OMFS research the VAS is commonly used to investigate many kinds of subjective experience, including pain [5]. The VAS (Fig. 2) is a straight, 100-mm line (10 cm), which can either be vertical or horizontal. It represents continuous pain intensity, where the left end of the line indicates “no pain,” while the other end denotes “pain as bad as it could possibly be.” A patients indicates their level of pain (in mm), by marking a single point on the line [9].

2.2. HPS
2.3. VRS or VDS
The VRS or VDS was created by Keele [13]. It was developed to assess patient responses to analgesics [9], with statistical validity and reliability. The VRS lists adjectives describing different levels of pain intensity [5], which consists of five numerically ranked words representing intensity of pain including the following [9]:
2.4. NRS (Fig. 4)
The NRS, which was developed by Downie [14] in 1978, consists of a vertical or horizontal line, with a total of 11 numbers, ranging from 0 to 10, denoting no pain to the worst possible pain, respectively [7]. Previous studies using the NRS offer great accuracy [9]. The NRS is a simple assessment tool that is easy to score. It can be administered in either the written or verbal form [9], but is not suitable for the elderly or very young child as it does not differentiate words and numbers [9].
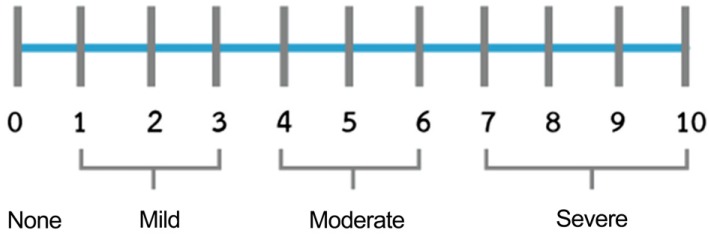 | Fig. 4Numerical rating Scale (NRS) [14].
|
2.5. FPS (Fig. 5)
The original FPS was a 7-point number scales, which was more difficult to complete since it did not follow the usual 0-5 or 0-10 metric [15]. Thus, Hicks et al. revised the FPS scale, changing it to a more suitable 0-10 scale. Bieri et al. however, developed this measurement as seven line-drawn faces in a horizontal format, ranging from no pain to worst pain [15]. Instead of a happy face, a neutral face, with the absence of smiles and tears, was used to depict no pain [7], with increasing levels of pain intensity along the remaining six-face continuum. Patients were asked to point to the face that best represented the intensity of their pain. The scores 0, 2, 4, 6, 8, and 10 were assigned to each face consecutively from no pain to more painful faces [7].
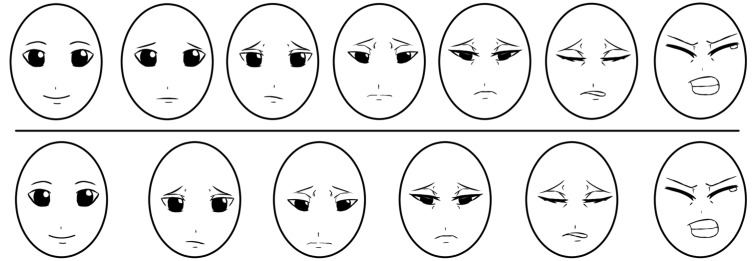 | Fig. 5Faces Pain Scale (FPS) (modified of Faces Pain Scale) [15].Top: Faces Pain Scale scored 0 to 6. Bottom: Faces Pain Scale-Revised, scored 0-2-4-6-8-10 (or 0-1-2-3-4-5).
|
2.6. WBS
Wong and Baker [16] created the WBS (Fig. 6), which shows faces ranging from a happy face at 0 (“no pain”) to a crying face at 10 (“worst pain”). Since patients are required to point to the face that best describes their feelings of pain, it is a popular method of pediatric pain assessment [17].
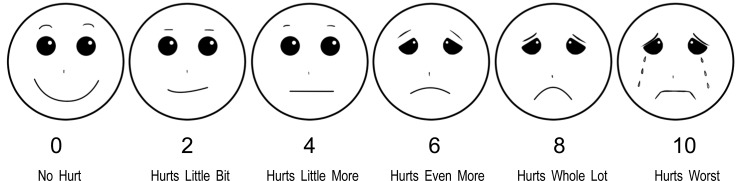 | Fig. 6Wong-Baker Faces Pain Rating Scale (WBS) (modified Wong-Baker Faces Pain Rating Scale) [16].
|
2.7. FCT
Ergun et al. [18] described the FCT a simple “cup” drawing. Patients are required to draw a completely full cup for the most severe pain, an empty cup for no pain at all, and a horizontal line in the cup to represent pain levels between [18]. The FCT score is calculated as a percentage (Fig. 7).
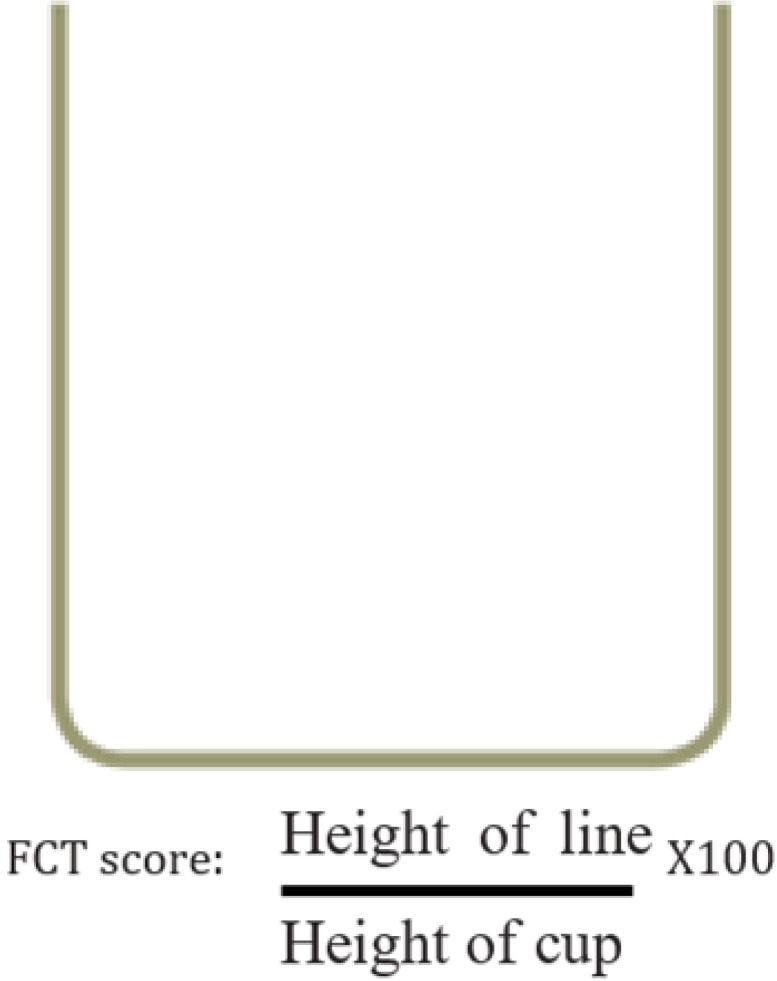 | Fig. 7Full Cup Test [18].
|
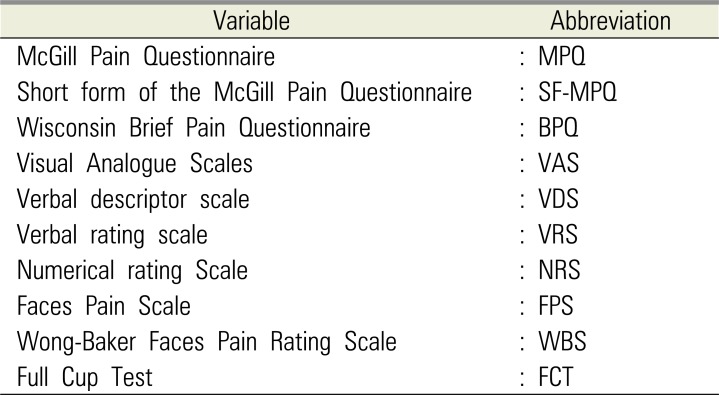
Table 1
Pain intensity scale abbreviations
![]()
Go to :
DISCUSSION
Pain that occurs during or post-OMFS can be difficult to assess. Since patient self-reports are accepted as the gold standard for pain assessment [19], pain assessment tools should be simple and straight-forward to use [6]. These tools should ideally measure baseline discomfort and the response to remedy [17].
Several previous articles in biomedical studies suggested the use of multidimensional scales to assess chronic pain, such as in cancer and lower back pain [681011], since it can be more difficult to assess than acute pain [6].
Sensory and affective pain can be relatively easily described using the simple intensity sub-scales of the SF-MPQ, which includes the PPI and VAS. The SF-MPQ is more commonly used instead of the MPQ because the latter measures several dimensions of the experience and intensity of pain, making it more complicated to use [9]. The BPQ for estimating the prevalence and severity of pain can be easily administered to a large number of patients. The BPQ can be a quantitative or qualitative measure of pain, and is thus, the best clinical pain measurement tool.
Several previous articles suggested the use of unidimensional scales to measure acute pain [56202122232425], caused by trauma, surgery, childbirth, or an acute medical disease. Previous OMFS articles mostly used the VAS for pain assessment in acute pain. Bijur et al. [26] found that the VAS was a highly reliable tool for assessing acute pain in adults. Garra et al. [17] demonstrated that the VAS was also more informative and relatively sensitive to changes in pain, compare to other ordinal scales. The VAS tool is recommended for measuring pre- and post-operative pain. Additionally, although the VAS is similar to the NRS, it is more sensitive. Although the NRS can both underestimate and overestimate scores than the VAS, however, it is easy to administer verbally in a clinical unit and is familiar as a clinical tool [27]. Polly et al. [27] suggested that the verbally administered the NRS can be related to the VAS in acute pain measurement. Unfortunately, the VAS has also been mentioned to have more practical difficulties than the VRS and the NRS [20].
The VRS can be applied by mail or telephone [21] and it separates the pain experience into distinct categories. However, since the intervals of the VRS are not equally spaced, it cannot be assumed to be equal to ordinal data. Another weak point of the VRS scale is that application of statistical analysis to nonparametric scales is limited [5].
Previous studies suggest the use of FPS for children and older people [691516172829], since children find it easier to comprehend than non-graphics-based pain assessment scales [20]. The larger number of faces and consequent finer distinctions, however, pose difficulty for children aged 3–5 years [29].
Stanford et al. [17] demonstrated that age is a significant predictor of a child's ability to accurately apply the FPS. The WBS is one of several faces scales that has been used in multiple pediatric pain assessment settings [17]. Given the lack of tools for older people, some researchers have also suggested the use of the WBS for this population. The FPS is self-reporting scale that uses facial expressions to assess pain intensity [30]. This has appropriate psychometric properties when used with the elderly [30]. The FPS-R, however, also has strong validity and reliability properties, and has been recommended to measure pain intensity in elderly adults [30].
The full cup test is useful for pain assessment of patients with low-education patients because it does not need any numerical or verbal skills and is easy to understand and complete the scale [20].
The common intervention sequelae in lower third molar intervention (LTMI) is associated with post-operative pain, swelling, infection, and limited mouth opening. All of these may be decreased with antibiotic regimens and anti-inflammatory drugs. Previous reviews of analgesic efficacy for control pain after all types of third molar surgery contain a significant number of clinical trials of the third molar intervention study [31], and several contain pain assessment after analgesic drug usage following LTMI. The studies were shown less analgesic drug usage relate to less post-operative pain or more analgesic drug usage correlate with more painful after surgery [32].
The VAS is the most common scale to evaluate postoperative pain (especially after LTMI) [33]. Apart from due to the surgery itself, post-operative acute pain can occur due to insufficient administration of local anesthesia. In 2005, Babatunde et al. [34] compared the effect of co-administered dexamethasone and diclofenac potassium (diclofenac K) with diclofenac K alone, on postoperative pain, swelling, and limited mouth opening following LTMI. They evaluated the pain score through a four-point Category Rating Scale as follows:
In 2013, Marko et al. [35] also assessed the intensity postoperative pain during the first seven days after LTMI using the VAS. Fenlon et al. [36] determined the effect of pre-operative paracetamol administration on pain following LTMI, using the VAS, 1 hour after the intervention [36]. In 2017, Raiesian et al. [37] assessed the effect of low-level laser therapy (LLLT) on pain in LTMI, by complete a questionnaire with the VAS for pain intensity measurement. Further, Nicoli et al. [38] studied the efficacy of two different anti-inflammatory agents, i.e., Diclofenac (Deltaflogin) and Lumiracoxib (Prexige), in postoperative pain control resulting from LTMI, and also assessed pain using the VAS, as did Huskisson in 1983 [39]. The pain measurement scale also consists of a 100-mm straight line, which allows quantification of the post-operative pain.
In 2016, de Oliveira et al. [40] compared the efficacy of ibuprofen and etodolac for controlling pain after extraction of lower third molars and assessed pain using an 11-point VAS scale. They used a line with 11 identical boxes, where the extremes represented the pain limitation of patients, from absent to severe, respectively. At 6, 12, and 24 h after the LTMI, patients were instructed to mark an X in the box on the scale to indicate their pain intensity. This study demonstrated that successful use of this tool, which was adapted so that the patient had an increased understanding of the scale. Baxendale et al. in 1993 [41] evaluated the effect of a single prophylactic dose of oral dexamethasone 8 mg on these complications, in a randomized double-blind study of 50 adult patients. They also used the VAS for post-operative pain assessment in all patients of this study. In 2017, Boonsiriseth et al. [42] showed the effects of 8 mg dexamethasone injection into the pterygomandibular space on the postoperative sequelae of lower third molar surgery. They analyzed the consumption of analgesics and assesses pain using the VAS.
In 2012, Aznar-Arasa et al. [43] performed the comparative study of the analgesic and anti-inflammatory effects of preoperative and postoperative administration of ibuprofen following LTMI. They measured the intensity of postoperative pain using a 100-mm VAS scale. The intensity of pain was assessed every 2–4 h for the first 14 h, and then every 8 h between, 24 and 64 h post-surgery.
In 2012, de Santana-Santos et al. [44] investigated the relationship between preoperative findings and short-term outcome following LTMI. In this study, pain intensity was evaluated using a 10-level VAS scale. In 2010, Barreiro-Torres et al. [45] studied the difficulty and technique LTMI, assessing the ability level of fourteen dental practitioners with varying levels of experience. They also used a 100-mm VAS scale and a modified version of a surgical difficulty scale.
A study conducted by Ozveri Koyuncu et al. [46], in 2013, on postoperative pain, also used a 10-cm VAS scale. In 2015, Nedal et al. [47] studied the effects of primary versus secondary wound closure on postoperative pain, swelling, and acute alveolar osteitis after surgical extraction of partially LTMI. They also used the VAS for pain intensity assessment in all volunteers.
In contrast, in 2013, Anighoro et al. [48] assessed baseline and postoperative pain (following LTMI), using a four-point VRS verbal rating scale from 0 to 3. In 2017, Gulüen et al. [49] evaluated the efficacy of platelet-rich fibrin (PRF) on postoperative edema and pain after impacted mandibular third molar surgery using both the VAS and VRS. All patients completed the VAS and VRS to assess their pain, and there was no significant differences between the two pain scores. It must be noted, however, that the NRS is easier to use to evaluate pain in adults [33]. Further, the WBS is widely applied to assess pain in children and older adults.
In conclusion, multidimensional scales such as MPQ, SF-MPQ, and BPQ are suitable to assess chronic pain, while unidimensional scales, like the VAS, VDS, VRS, NRS, FPS, WBS, and FCT are more suitable for acute pain evaluation occurring after LTMI.
Go to :
 XML Download
XML Download