

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Various clinical procedures in dentistry carried out on adults and children require the use of palatal injections for obtaining local anesthesia. These palatal injections can be painful owing to the thick keratinized palatal mucosa, especially for pediatric patients whose cooperation is essential for treatment. Fear of the syringes and needle insertion is high among children [1]. This may complicate the procedure of local anesthesia prior to dental treatment, both for the child and the clinician. For this reason, topical anesthesia has been in use in order to reduce pain to the patient [2].
Reduction of pain during dental procedures can nurture the relationship of the child patient and dentist, building trust, allaying fear and anxiety, and promoting a positive behavioral attitude [34], as well as help to provide overall comfort and well-being during the entire dental experience. Researchers are constantly searching for tools which can enhance the comfort of dental procedures. The challenge is to find an effective method that can be utilized in the pediatric population [5].
Behavior management in pediatric dentistry encompasses various elements, ranging from creating a pain-free environment to acceptance of treatment by a child. A pain-free environment for the child typically is created by using psychological tactics and topical anesthetic agents prior to injection [6]. Topical anesthesia is a fundamental part of a local anesthesia administration as it has both psychological and pharmacological impact [7]. It is effective on surface tissues (2–3 mm in depth) to reduce painful needle penetration of the oral mucosa that act by blocking signal transmission in the terminal fibers of sensory nerves. The prior application of topical anesthesia helps to alleviate but does not eliminate, pain associated with needle insertion and anesthetic agent injection [8]. Their effects are limited to the control of painful stimuli occurring in or just beneath the mucosa [910]. The literature reports mixed results regarding the efficacy of topical anesthetics in reducing injection pain [10111213]. The application of topical anesthetic can reduce the discomfort of intraoral anesthetic injections, provide anesthesia for intraoral operative procedures, yield symptomatic relief of pain due to superficial mucosal lesions such as ulcers or even relieve a toothache and post-extraction pain [14].
Topical anesthetics are available in the form of ointments, gels, sprays, or as adhesive patches [15]. Cetacaine is a topical anesthetic with triple action formula, which is available in spray and liquid forms. Though its existence is from the 1960s, its use in the pediatric population has not been reported [16]. Mucopain (Benzocaine) 20% gel has been the most popular topical anesthetic among children due to its rapid onset of action and acceptable taste, whereas the use of Eutectic mixture of local anesthetic (EMLA) cream as a topical anesthetic in children has shown promising clinical results in dentistry [1718]. Studies comparing Mucopain (Benzocaine) gel and EMLA cream were not conclusive.
So far, to our knowledge, no study has evaluated the comparative efficacy of these three topical anesthetics to achieve palatal injection. Hence, the topical anesthetic efficacy of cetacaine liquid (Cetylite Industries, Inc, Pennsauken, NJ), EMLA cream (2% AstraZeneca UK Ltd, Luton, UK), and Mucopain (Benzocaine - 20% Jelly, ICPA health products Ltd, Ankleshwar, India) gel was evaluated among 7–11-year old children in the present study.
Go to : 
METHODS
Participants in the study included 90 healthy and positive (Frankl's rating 3 and 4) [19] subjects (45 boys, 45 girls) of age 7–14 years attending the Department of Pedodontics who required maxillary palatal injections for extractions of primary molars. Only those with no previous experience of local anesthetic injection were included in the present study. Subjects with special health care needs, systemic illness, abscesses, and space infections were excluded. After explaining the complete study design, possible risks, and discomforts of the procedure, written informed consent was obtained from the parents/guardians of all the subjects. The study protocol was approved by the institutional ethical committee and approval from Dr.NTR University of Health Sciences, AP. (NO. D148407052). The study was carried out from December 1, 2015 to June 1, 2016.
Power analysis yielded 28 subjects per group. A pilot study was conducted to determine the sample size prior to the main study. Sample size determination revealed that a minimum of 30 subjects in each group was required, thus giving a total sample of 90 for an ANOVA on four independent sample means (with an effect size of 0.34 measuring the changes in physiologic responses among three groups, α = 0.05, and a power of 0.8). Subjects were randomly assigned into three groups with 30 subjects in each group using computer-generated randomization. Groups A, B, and C received Mucopain gel, Cetacaine liquid, 2% EMLA, respectively, as a topical anesthetic prior to the local anesthetic injection prick. Direct self-report and physiological measures were ascertained using Faces pain scale– Revised (FPS-R) [20] and Pulse oximeter (Gibson, Fingertip Pulse Oximeter, MD300C29, Beijing Choice Electronic), respectively. Behavioral assessment was performed using the Modified Children hospital of the eastern Ontario Pain Scale (CPS)8 and Face Legs Activity Cry Consolability scale (FLACC) [21]. An investigator, not related to the study, recorded outcomes from the subjects. Scores of pulse oximeter were recorded preoperatively (i.e., before applying topical anesthetic) and postoperatively (after local anesthetic injection). Scores from CPS and FLACC were recorded peri-operatively (i.e., during the administration of local anesthesia). Scores from FPS-R were recorded when the child's pulse (heart) rate returned to normal.
The palatal mucosa was dried before the application of Benzocaine gel and EMLA cream, whereas no isolation was performed for Cetacaine liquid. Benzocaine gel and EMLA cream were applied with the help of the cotton applicator. The cetacaine liquid was dispensed using leur lock cup onto a cotton applicator and applied on the site of needle prick for 1 minute. Later 0.2 ml of anesthetic solution (2% Lidocaine with adrenaline 1:80,000) was administered palatally using a 27-gauge needle at the rate of 1 ml/min approximately. After behavioral and physiological assessments, the buccal injection was administered, and upon achieving profound anesthesia (i.e., after 5 minutes), a standard extraction procedure was performed. The patient was blinded to the topical anesthetic used. The statistical analyst was blinded regarding the three groups, and decoding was performed only after the analysis of results.
The data were entered using Microsoft Excel spreadsheet 2010. The statistical analysis was performed using SPSS (IBM Corp., Version 21.0. Armonk, NY: IBM Corp.). For categorical variables, the values were represented as numbers and percentages. For continuous variables, the values were represented as the mean and standard deviation. To test the mean difference among three or more groups, a one-way ANOVA with a post hoc (Tukey HSD) test was used. All the efficacy parameters were presented as an absolute change from baseline. All P values less than 0.05 were considered statistically significant (P < 0.05).
Go to :
RESULTS
A total of 90 children (45 boys and 45 girls), who required the extraction of maxillary primary molars were included in the study. The mean age of the children was 9.74 ± 1.9 years for boys and 8.32 ± 1.36 years for girls. There was no significant difference among the groups in terms of age (independent t-test, P = 0.88) or sex (independent t-test, P = 1). No adverse events were observed during the course of the study.
Statistical analysis
Shapiro-Wilk's normality test results showed that all physiologic responses followed a normal distribution. Therefore, parametric methods were applied for the analysis of the data. Mean responses among participants for all variables were assessed using analysis of variance (ANOVA) and post hoc Tukey HSD test. Other variables did not follow normal distribution (i.e., skewed). Therefore, non-parametric methods were applied for the analysis of the data. Overall comparisons of subjective and behavioral responses were analyzed using the Kruskal Wallis test. Further pairwise comparisons were analyzed using the Mann Whitney test. The level of significance was set at P < 0.05 for all tests.
Intergroup comparison between mean values of physiological parameters (heart rate) at baseline (P = 0.215), during extraction (P = 0.0001), and after extraction (P = 0.010) revealed statistically significant differences (Table 1, Fig. 1).

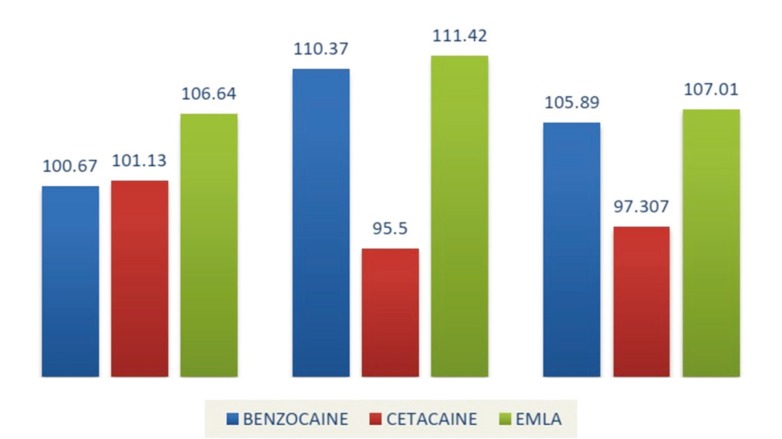
Table 1
Comparison of mean value of physiological responses between groups A, B and C
![]()
Pairwise comparison of Groups A and B showed a significant difference in physiological measures whereas no difference was observed between Groups A and C or between Groups B and C. During injection needle prick, physiological scores showed a significant difference between Groups A and B only. No difference was seen among the three groups with respect to physiological measures after the injection needle prick (Table 2).
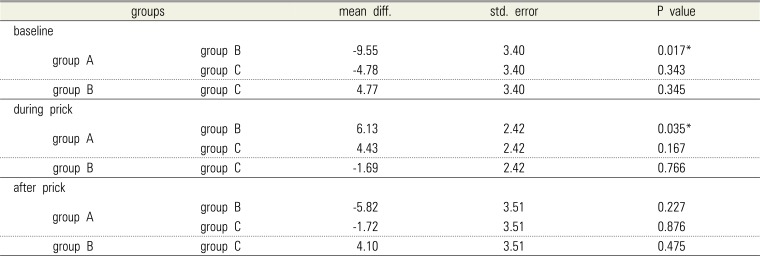
Table 2
Pairwise comparison of physiological responses between groups A, B and C
![]()
Intergroup comparison between the mean values of the self-report scale (FPS-R) after extraction revealed that there was a statistically significant difference among the three groups (P = 0.001). Furthermore, the intergroup comparison between the mean values of FLACC and CPS during extraction revealed that there was a statistically significant difference between the three groups for both the scores (P < 0.05).
The mean FPS-R, FLACC, and CPS scores were found to be higher in Group C when compared to Groups B and A, indicating greater pain experienced among the children in Group C compared to the children in Groups B and A (Table 3, Fig. 2 and 3). This difference in pain between Groups B and C was statistically significant (P < 0.05). Intergroup comparison between Groups A and B for FPS-R, CPS, and FLACC scores was found to be significant (P < 0.05). There was no statistical difference in mean pain scores between Groups A and C for FPS-R, FLACC, and CPS scores (P > 0.05) (Table 4).
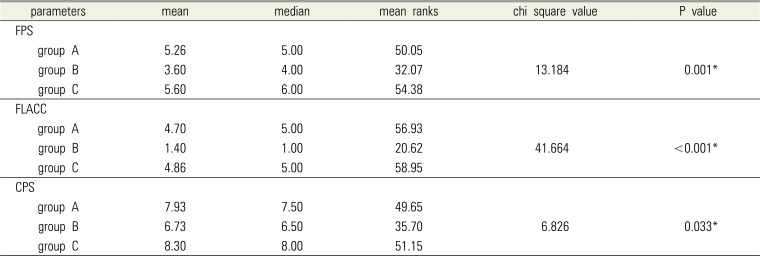
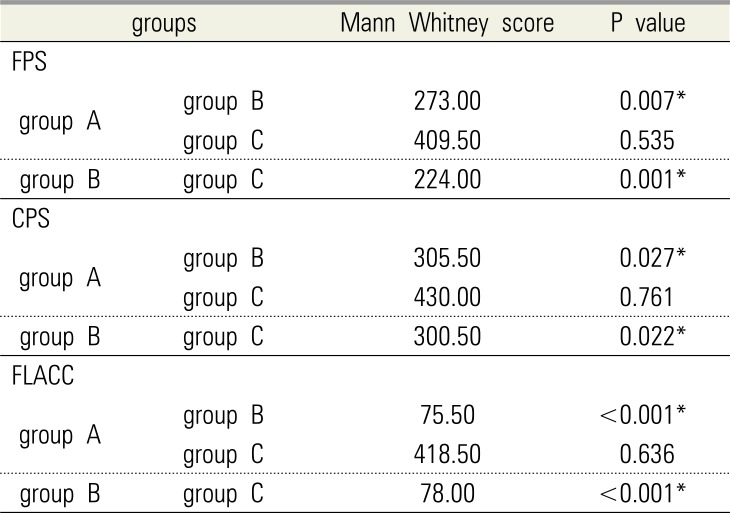
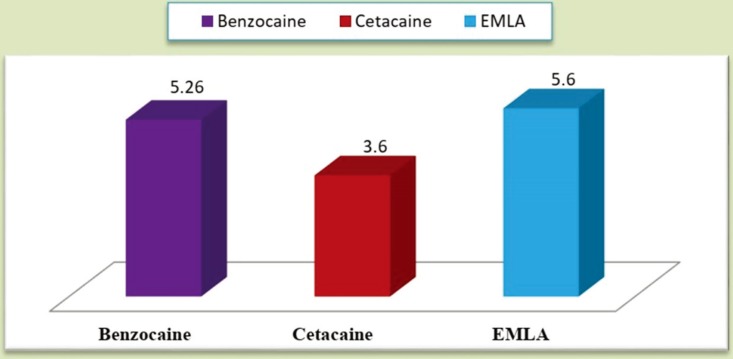
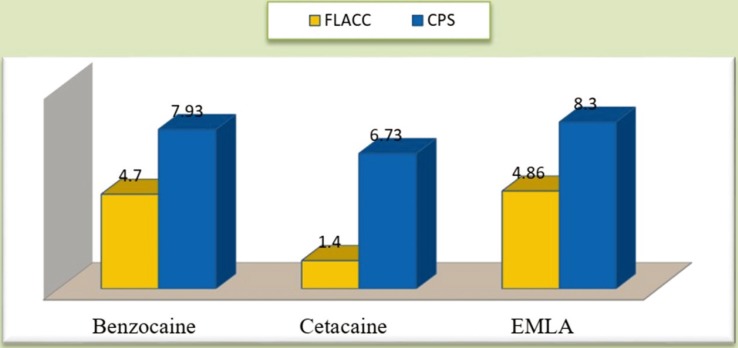
Table 3
Comparison of mean value of subjective and behavioral responses between groups A, B, and C
![]()
Table 4
Pair wise comparison of subjective and behavioral responses between groups A, B, and C
![]()
Go to :
DISCUSSION
Injection of local anesthesia is one of the most fearful treatment procedures in children [22]. Among all the injection techniques, palatal injections are deemed painful and also one of the most traumatic techniques in dentistry. Several methods have been proposed to alleviate pain during local anesthetic administration; [2324252627] one among them is the use of topical anesthetics.
The present study included 90 subjects, 45 boys and 45 girls. Martin et al. [10] found that injection order influenced patient perception of pain, with the second injection being perceived as more painful than the first. As a result, only those with no previous experience of local anesthetic injection were included in the present study. The mean pain scores (FPS-R, CPS, and FLACC) suggest that needle prick with Cetacaine (B) was less painful compared with EMLA (C) or benzocaine (A).
Pain thresholds and physical reactions to stimuli vary among children; therefore, one scale may not quantify the pain of a child. For better outcomes of the present study, three types of scales were used: subjective (FPS-R), objective (CPS, FLACC), and physiological (PULSE OXIMETER) measures [4]. The use of composite scales was found to be ideal by Goodenough [28].
Tsze DS et al. [20] concluded that FPS-R demonstrates strong psychometric properties in children between 4 to 17 years of age, including within subgroups of age, sex, and ethnicity. However, convergent validity is questionable in 7-year-old children. The CPS scale is used for children aged 1 to 7 years. However, the modified CPS was successfully used in a study by Primosch et al. [8] that compared the effectiveness of topical anesthetics in children aged 7–15 years. Nilsson S and Finnstrom B (2008) [21] established concurrent and construct validity of the FLACC as a measure of needle-related procedural pain in children aged 5–16 years. In the present study, there was a significant difference in pain perception among the three groups concerning subjective and behavioral responses [21].
Apart from these scales, the pulse rate was measured as a physiological measure, using a pulse oximeter in the present study. Physiological responses were statistically significant among the three groups. However, statistical data shows that physiological scores were less in cetacaine (B) group compared to that of benzocaine (A) and EMLA (C) groups.
The ability of various topical anesthetics to penetrate the oral mucosa to produce anesthesia has been well documented [29,30]. Cetacaine (Cetylite Industries, Inc, Pennsauken, NJ) is a topical anesthetic that consists of Benzocaine, Butamben, and Tetracaine hydrochloride that has perfect viscosity for soft tissue procedures and also has enough resistance to flow into the target tissue [31].
An innovative cap design allows the practitioner to place any luer lock syringe onto the Cetacaine vial and draw to the required amount (the maximum dosage is 0.4 ml, whereas the minimum is 0.2 ml per office visit). Christensen GJ stated that 81% of 25 evaluators stated they would incorporate Cetacaine Liquid into their practice. 88% rated it excellent or good and worthy of trial by colleagues [32].
Eutectic mixture of local anesthetics (EMLA) contains both lidocaine 2.5% and prilocaine 2.5% [33]. It significantly reduced the injection pain among adults during the delivery of dental anesthetic. Apart from this, EMLA 5% cream was found to be effective in reducing the pain induced with minor restorative dental procedures, gingival probing, periodontal scaling, and even arch bar removal [8].
According to a study by Holst and Evers, also conducted in adults, EMLA is more effective than “conventional” intraoral topical agents in the palate [34]. It was able to eliminate or reduce pain from anesthetic needle prick in the maxillary vestibular mucosa [35]. Though benzocaine 20% gel is the most commonly used topical anesthetic agent [36], it is not potent enough to eliminate pain from a needle prick [3738].
In our present study, pain perception in the cetacaine (B) group was significantly lower compared to that in the benzocaine (A) and EMLA (C) groups whereas, no significant difference in pain perception was observed between the benzocaine (A) and EMLA (C) groups. This finding is similar to a study performed by Primosch RE et al. [8] that concluded there was no significant difference between benzocaine 20% gel (Hurricaine) or EMLA 5% oral adhesive (EMLA 5% cream in Orabase Plain). Contrary to this, a study by Nayak R et al. [39] concluded that 5% of EMLA cream provided superior pain reduction compared to 18% benzocaine gel and 5% lignocaine. However, it was a bilateral double-blinded interventional study done in two phases.
There was a significant difference in the mean pain scores between Cetacaine, EMLA, and benzocaine gel with respect to subjective, objective, and physiological scores. Superior results with Cetacaine may be due to its increased depth of surface anesthesia compared to EMLA and benzocaine gel. It is difficult for EMLA cream to remain in the region of application for a long time because of the low viscosity, and it does not have a very acceptable taste [37]. Even the presence of moisture does not affect the efficacy of cetacaine [40].
The results from numerous studies regarding the use of topical anesthetics in children were contrary to one another because acute pain can be influenced by psychological factors, such as anxiety, fear, trust, and perceived control over the stimulus, which may account for the equivocal findings of dental topical anesthesia efficacy. The objective fears of the child during the administration of local anesthesia also could be from the sight of the needle during needle insertion[38]. Similarly injection rate, solution volume, agent pH, and tissue buffering capacity are additional variables confounding the reported pain experience [41].
In conclusion, cetacaine can be considered an effective topical anesthesia compared to mucopain and EMLA cream, as it reduces pain perception during palatal injections. As drying of the mucosa is not needed prior to the application of cetacaine, it can be considered as a better alternative to Mucopaine gel and EMLA cream, particularly in the pediatric population where isolation is deemed difficult.
Go to :
 XML Download
XML Download