

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Surgical extraction of third molars is associated with postoperative pain and swelling at the extraction site [1]. Postoperative pain is usually moderate to severe in the first 12 h after the procedure and lasts for 3–5 days. However, with non-steroidal anti-inflammatory drugs (NSAIDs), these symptoms usually subside within 24 h [2]. NSAIDs are the drug of choice for pain management after surgical extraction of third molars [34].
NSAIDs reduce prostaglandin production by inhibiting cyclooxygenase enzyme activity, thereby reducing the local inflammatory response and peripheral sensitization of nociceptors [5]. Diclofenac sodium, which is an NSAID with analgesic and antipyretic activities, inhibits prostaglandin synthesis [6]. It is among the most extensively used NSAIDs and is prescribed in rheumatoid arthritis, osteoarthritis, bursitis, ankylosing spondylitis, toothache, dysmenorrhea, renal colic, and posttraumatic and postoperative inflammatory conditions [6789101112131415]. Adverse effects of diclofenac sodium are generally mild epigastric pain, nausea, headache, dizziness, and rashes and rarely gastric ulceration and earache [16].
Etodolac is a relatively new indole acetic acid derivative. Its mechanism of action is not completely understood, unlike other NSAIDs, but may be related to the inhibition of prostaglandin synthesis [6]. At lower doses, its gastric tolerance is better than that of other NSAIDs. However, it can cause side effects, including abdominal pain, rashes, and dizziness. It has been approved for use in osteoarthritis, rheumatoid arthritis, and acute musculoskeletal pain and has been successfully used as a postoperative analgesic in dentistry for postoperative pain control [617181920212223].
As postoperative pain after surgical extraction of third molars is moderate to severe, pain relief or control is often challenging to achieve. However, this condition offers an opportunity to study and evaluate the potency of analgesics in validated clinically relevant models [2425]. Various NSAIDs are being used after third molar extractions for pain relief. Diclofenac sodium and etodolac have been studied with different drugs for postoperative analgesia in dentistry, but data are limited on the comparative effect of diclofenac sodium and etodolac for pain control after surgical extraction of third molars in the Indian population. Therefore, the aim of the present study was to compare diclofenac sodium and etodolac in terms of analgesic efficacy and safety at a tertiary care hospital in western India.
Go to : 
METHODS
We procured diclofenac sodium from Unison Pharmaceuticals Private Limited, India, etodolac (Etogesic 400) from Cadila Healthcare Limited, India, and dummy preparations from Shri Sarvajanik Pharmacy College, Mehsana, Gujarat, India. This was a double-blind, double-dummy, randomized, parallel-group, split-mouth study.
The sample size for the study was estimated to be 100, with 95% power, 5% α-error, 10% drop-out rate, and an estimated difference between means of 0.65 [26]. Inclusion criteria were as follows: 1) age between 18 and 60 years; 2) acute pain for less than 4 weeks; and 3) willingness to provide written informed consent. Exclusion criteria were as follows: 1) a history of hypersensitivity to study drugs; 2) tooth injury; 3) acute pain for more than 4 weeks; 4) pregnancy or lactation; 5) inability to participate for the full proposed length of treatment with follow-up visits; 6) unwillingness to provide written informed consent; 7) a history of bypass surgery within the past 6 months; 8) current anticoagulant medication; 9) a history of valvular heart disease; and 10) uncontrolled diabetes, uncontrolled hypertension, neoplasms, known neuropsychiatric illness, blood dyscrasia, coagulation disorders, or metabolic disorders.
Written informed consent was obtained from all participants who met the eligibility criteria. Participants were allocated to two groups after randomization with the RANDO software. Ethical approval was obtained from the Institutional Review Board (IRB), Government Medical College, Bhavnagar, Gujarat, India (Registration No. ECR/557/Inst/GJ/2014; Date: 29/04/2014) for the study protocol and implementation (IRB no. 588/2016). The study was registered prospectively in the Clinical Trials Registry of India (CTRI number: CTRI/2016/11/007437).
Group 1 received 50 mg oral diclofenac sodium 8 hourly and dummy preparations of etodolac for 3 days while group 2 received 400 mg oral etodolac 8 hourly and dummy preparations of diclofenac sodium for 3 days [2728]. Study medications were started 2 h postoperatively and administered orally. Pain was assessed for each participant at baseline (time 0) and 2, 6, 24, 48, and 72 h after administration of study medication using the 100-mm visual analogue scale (VAS) [2930]. Patients were followed-up for 3 days either in the outpatient department of dentistry or over the telephone for pain assessment and safety. If the study medications did not show an effect in 12–24 h, oral tramadol 100 mg stat and 4–6 hourly, as needed, was used for rescue analgesia.
Baseline characteristics (age, sex, and duration of surgery) were compared between the treatment groups. P-values less than 0.05 were considered statistically significant. Data are expressed as mean ± standard error of mean. The mean time to analgesia at different time points and maximum pain relief were compared using the unpaired t-test or Mann–Whitney U test for an intergroup analysis and using the analysis of variance for an intragroup analysis. Patient global evaluation (excellent, very good, good, fair, or poor) was also performed. Statistical analyses was performed using GraphPad InStat trial version 3.06 (GraphPad Software Inc., San Diego, USA).
Go to :
RESULTS
Figure 1 showed the CONSORT flow diagram of patients in this trial.
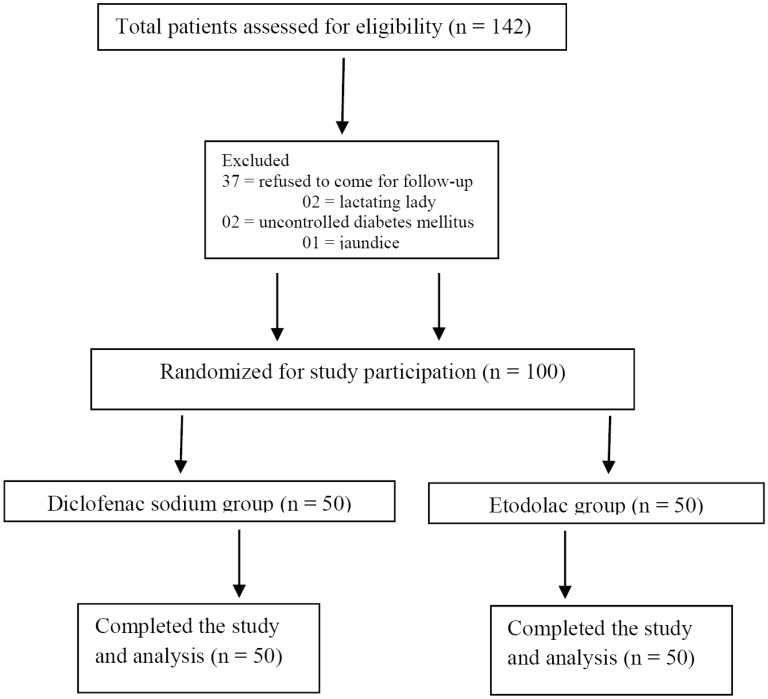
Table 1 shows the baseline characteristics of both treatment groups. The groups showed no significant differences in the baseline characteristics (P > 0.05), duration of surgery, or baseline VAS score (P > 0.05).

Table 1
Baseline characteristics in diclofenac sodium and etodolac groups
![]()
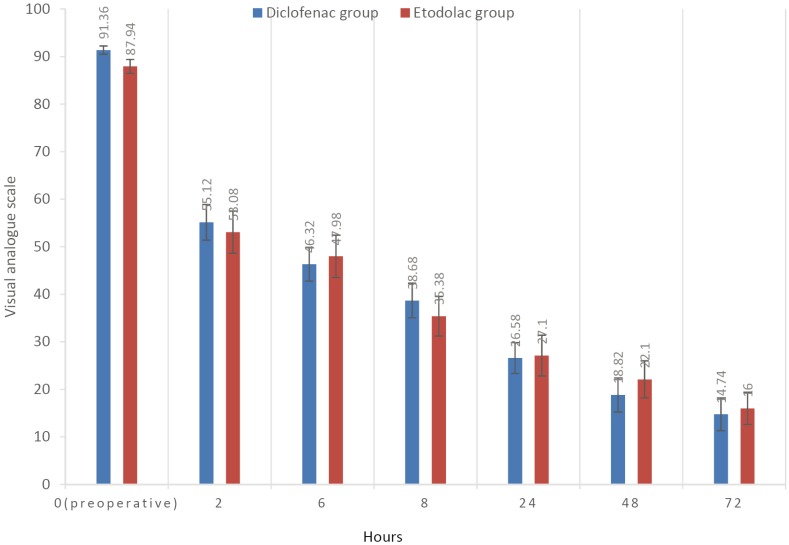
Table 2 shows the comparison of pain intensity based on VAS scores between the two groups. N both groups, pain intensity reduced to half within 2 h postoperatively. The VAS score reduced from 91.36 ± 0.86 to 55.12 ± 3.75 in the diclofenac group and from 87.94 ± 1.46 to 53.08 ± 4.42 in the etodolac group (P > 0.05) 2 h postoperatively. The pain intensity reduced relatively similarly in both groups (P > 0.05) 6 and 8 h postoperatively. The pain intensity reduced to merely one-fifth of the baseline value 24 h postoperatively. The maximum reduction in pain intensity was achieved similarly in both groups (P > 0.05) 48 and 72 h postoperatively.
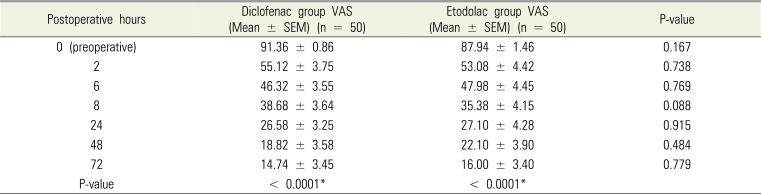
Table 2
Pain intensity values measured on the visual analogue scale preoperatively and 2 and 72 h postoperatively in diclofenac sodium and etodolac groups
n: number of participants; data are expressed as mean ± standard error of mean. Diclofenac sodium and etodolac groups were compared in terms of pain intensity at predetermined times using the Mann–Whitney U test (Table 2), and results were not statistically significant (P > .05). Intragroup comparisons were performed using repeated analysis of variance. *= compared to preoperative value after any postoperative period. VAS = visual analogue scale
![]()
Although etodolac was better tolerated compared to diclofenac sodium, both study drugs caused adverse reactions. Vomiting occurred in two patients in each group (P = 1.000). Earache occurred in one patient in the diclofenac group but in none of the patients in the etodolac group (P = 1.000). Table 3 shows the incidence of adverse reactions.

As the incidence of adverse reactions was low in both groups, both drugs may be considered safe and well tolerable.
Table 4 shows the number of patients who required rescue analgesia. Pain intensity could not be controlled with study medications in three patients of the diclofenac group and two patients of the etodolac group (P = 1.000). In these patients, tramadol 100 mg was orally administered. Table 5 shows the results of the patient global evaluation. Most participants reported the analgesic efficacy of the study medication to be “excellent” or “good.” Only a few participants reported a “very poor” evaluation.

Table 4
Incidence of rescue medication in both study groups
| Rescue medication | Diclofenac group | Etodolac group | P-value |
|---|---|---|---|
| Tramadol | 3 | 2 | 1.000 |
![]()

Go to :
DISCUSSION
In the present study, the safety and analgesic efficacy of diclofenac sodium and etodolac were compared following surgical extraction of third molars. The patients were equally distributed (P > 0.05) between the two treatment groups with respect to demographic features and baseline characteristics. Aging is associated with an increased risk of postoperative complications following surgical extraction of third molars [31]. In the present study, the mean age of study participants in both groups was below 35 years, so the risk of complications was low. The average surgery time was 32.62 ± 1.25 and 36.32 ± 1.44 min in the diclofenac and etodolac groups, respectively. Participants with risk factors for the development of complications or difficult surgery had been excluded. This could have led to biasness. No serious adverse effects or complications related to surgery were encountered in any treatment group throughout the study period.
In the present study, etodolac was as effective as diclofenac sodium in pain alleviation at all postoperative time periods, with no statistically significant difference. The mean VAS score was 55.12 ± 3.75 in the diclofenac group and 53.08 ± 4.42 in the etodolac group 2 h postoperatively (P = 0.738). Pain intensity was moderate to severe preoperatively and reached nearly half the level 2 h postoperatively. Thus, the mean duration for start of analgesia was nearly 2 h for the half-maximal response. As pain intensity is maximum during the first 12 h, the rapid onset of analgesia in both groups reaffirmed the effectiveness of both drugs as good analgesics.
No statistically significant difference was found between the groups at any postoperative time period from baseline to 72 h postoperatively. At 2, 6, 8, 24, 48 and 72 h postoperatively, pain alleviation was estimated using the VAS score, which scaled down to 14.74 ± 3.45 in the diclofenac group and 16.00 ± 3.40 in etodolac group from the initial value to 72 h postoperatively (Fig. 2). A statistically significant difference between baseline and 72-h VAS scores was found individually in both groups (P < 0.01).
Both drugs in this study were found to be safe and well tolerable with regard to adverse events. In the present study, two patients developed vomiting in each group, and one patient developed earache in the diclofenac group. Along with study medications, antacids, including tablet famotidine and capsule omeprazole, and antimicrobial drugs, including tablet amoxycillin-clavulanic acid and metronidazole were prescribed, so adverse reactions were less.
Rescue medication (tramadol 100 mg) was required for three patients in the diclofenac group and two patients in the etodolac group. Only a few participants required rescue analgesia, suggesting the safety of both study drugs. Tablet tramadol has been proven effective as an alternative to NSAIDs for orthopedic pain, so we used it as rescue medication [32]. No statistically significant difference was found between the groups with respect to the patient global evaluation [33].
Akbulut N et al. reported that diclofenac sodium was a better analgesic compared to etodolac, although without statistical significance [26]. Diclofenac sodium and etodolac have been proven effective as an analgesic for pain associated with oral surgery, orthopedic disorders, and rheumatoid arthritis [343536]. Silva et al. reported that etodolac is a better analgesic after surgical extraction of third molars compared to ibuprofen [19]. Etodolac has also been proven a better anti-inflammatory agent compared to other NSAIDs for some particular use [37]. It has shown better gastrointestinal tolerability to diclofenac and other NSAIDs [3438] and has also been proven an effective alternative to diclofenac sodium in orthopedic pain [35]. An etodolac dose of 400 mg has been shown to have better analgesic effects compared to other doses postoperatively. Therefore, in the present study, a dose of 400 mg was administered [20]. Consistent with previous studies, this study showed etodolac to be equally effective in terms of pain alleviation. Our study also provided data on the postoperative use of etodolac as an analgesic in dentistry after surgical extraction of third molars.
In addition to pain, studies evaluating postoperative trismus and edema are underway. As our primary objective was to evaluate the safety and analgesic efficacy of etodolac, we did not evaluate trismus or edema. This can be considered as a limitation of our study. Furthermore, the effect of study medications in difficult surgeries was not evaluated because of the potential risk for bias.
As there is increased need of better and safer alternatives for pain relief after surgical extraction of third molars, etodolac can be a better alternative to diclofenac sodium.
Etodolac can be considered equally effective and safe as diclofenac sodium in terms of analgesic efficacy and safety after surgical extraction of third molars.
Go to :
 XML Download
XML Download