

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Overactive bladder (OAB) syndrome is defined as urinary urgency, often with associated urinary frequency and nocturia, with or without urge urinary incontinence (UI) in the absence of urinary tract infection or other pathology [1]. OAB affects 33 million Americans (16% of the United States [US] population), making it more prevalent then asthma (15 million), osteoporosis (10 million), diabetes mellitus (7 million), or Alzheimer disease (4 million) [2,3]. The condition afflicts all ages and has significant negative effects on quality of sleep [4], physical health [5], and mental health [5,6], all of which correlate directly to symptoms severity.
Insufficient sleep and sleep disturbance are recognized as major factors affecting well-being and physical health [7]. Sleep disturbance is present in a large portion of those with OAB and is directly associated with symptom severity, worsened depression, anxiety, and stress [8]. Poorer sleep quality has been correlated with an increased total daily urgeassociated incontinence episodes, total daily micturitions, and with moderate to severe urinary urge sensation [4].
Current literature focuses on the epidemiology relating sleep disturbance and sleep quality to the diagnosis of OAB and symptom severity with limited information focusing on how treatment affects sleep. In a study investigating antimuscarinic therapy, Warsi et al. [9] found that successful treatment of OAB resulted in improvements in sleep quality and efficiency. Similarly, men with OAB who were treated with solifenacin reported improvement in sleep disturbance [10].
Treatment with advanced therapies such as sacral neuromodulation (SNM) have been shown to decrease night-time voiding symptoms [11] and have been related to sleep improvement when measured using disease-specific health-related quality of life measures [12,13].
Unfortunately, there is a little data relating chronic SNM therapy for lower urinary tract symptoms (LUTS) to sleep disturbance changes measured using the Patient-Reported Outcomes Measurement Information System® (PROMIS). Chronic SNM is associated with significant improvements in urinary symptoms with improved treatment persistence when compared to pharmacologic therapy [14,15,16,17].
PROMIS assess self-reported universal-health across multiple chronic conditions using the design structure of item response theory (IRT) [18,19]. Unlike traditional disease-specific patient-reported outcome (PRO) questionnaires, IRT scales are based upon items of varying difficulty creating a unidimensional scale modeling the items in questions, the respondent, and unobservable characteristics (i.e., stress, knowledge, attitude, etc.) [20]. Investigation using PROMIS item banks has gained popularity in clinical research and had proven content validity in LUTS [8,21,22,23]. Use of IRT based health measures allows for incorporation of computer adaptive testing (CAT) which tailors the questions administered based upon the respondent's prior answers [24]. Use of PROMIS-CAT improves efficiency and decreases patient burden without affecting reliability and precision [24]. Statistical analysis provides more insightful information at the item level and allows for detection of significant changes in smaller samples due to known standard error and higher precision with a scoring system based upon the general US population [20,25,26].
The primary objective of this study was to examine changes in self-reported sleep disturbance using a validated item bank from the PROMIS following implantation of a SNM device for treatment of refractory OAB. We hypothesized that those individuals treated with SNM would have a significant improvement in self-reported sleep disturbance, given the documented improvement in symptom severity needed to quality for implantation of the SNM device. Additionally, we sought to identify factors that may be associated with improvement in sleep disturbance.
MATERIALS AND METHODS
This is a sub-analysis of data collected under an Institutional Review Board (approval number: RSRB00069994) approved retrospective cohort with waived informed written consent at the University of Rochester Medical Center (URMC) in Rochester, NY, investigating factors associated with revision/removal of SNM following successful implantation. This analysis focuses on changes in sleep disturbance in a disease-specific cohort. Sleep disturbance was assessed using the PROMIS item bank–Sleep Disturbance (PROMIS-SD). Only those subjects with pre- and post-procedure PROMIS-SD data related to sleep disturbance were included in this sub-analysis. Subjects were then grouped based upon their change in sleep disturbance, to compare those with improvement to those who had no change or worsened sleep disturbance following SNM implantation. Improvement in sleep disturbance is defined as a PROMIS-SD t-score change of <0.
PROMIS item banks are routinely collected throughout the URMC using tablets that are securely linked to a web-based data-server. These outcomes are then automatically incorporated into the individual's electronic medical record (EMR, eRecord; Epic, Verona, WI, USA). All of the item banks collected at our multi-specialty adult pelvic health clinic take advantage of CAT which limits the patient burden. Item banks collected include: 1) Sleep Disturbance (PROMIS-SD), 2) Physical Function (PROMIS-PF), 3) Depression (PROMIS-D), and 4) Pain Interference (PROMIS-PI). The PROMIS raw scores collected using the CAT item banks are automatically converted into t-scores which range from 0 to 100. All item banks have a mean score of 50 and a standard deviation (SD) of 10, referent to general US population [26]. Higher t-scores indicate a higher level of the specific health domain being investigated. In general an improvement of 5 points, is considered to be a clinically meaningful change for PROIMS t-scores [27].
All data were extracted from the EMR for clinic visits between March 2016 and October 2017. Data collected included age, body mass index (BMI) (kg/m2), American Society of Anesthesiologists (ASA) classification score, race, insurance type (private vs. public), medical and psychiatric comorbidities, and PROMIS t-scores. Pre-procedure diagnoses were categorized as urge UI, OAB, and mixed UI.
All statistical analysis was performed using the open source statistical package R v3.2.2 via the R Studio interface. A one-tailed paired t test was used to investigate significant changes in PROMIS t-scores within individuals within each group. The groups were compared to identify potential clinical or subjective associations with sleep disturbance response, using Fisher's exact test to associate categorical and ordinal variables while continuous variables were analyzed using a two-tailed, independent samples t-test or Mann–Whitney U-test, with p<0.05 considered statistically significant. Age and BMI are presented as the median (range), while nominal and ordinal data are presented as the raw number (n). PROMIS t-scores are presented as mean±SD.
RESULTS
Of the 40 subjects with pre-procedure PROMIS-SD scores, only 14 women had post-procedure t-scores following SNM implantation for refractory OAB. Improvement in sleep disturbance was noted in 7 (50%) of these women.
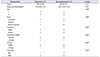
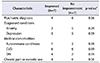
Patient demographics and clinical characteristics are presented in Table 1 with chronic medical comorbidities in Table 2. Those with improved sleep disturbance had a median age of 64 years (range, 53–83 years) and BMI 37.8 kg/m2 (range, 20.1–47 kg/m2) compared to a median age of 58 years (range, 39–72 years) with a median BMI of 36.7 kg/m2 (range, 24.9–47.4 kg/m2) in those who did not have improvement, p=0.25. The groups were similar in ASA classification score (p=0.99), race (p=0.99), insurance type (p=0.99), pre-procedure diagnosis (p=0.52), medical comorbidities (p=0.71), and psychiatric comorbidities (p=0.56). There were no significant differences in number of women with a chronic pain diagnosis and chronic narcotic use between the groups, p=0.47. Only one woman had significant lower extremity edema that required compression stockings. No one in this sub-analysis had obstructive sleep apnea or was taking sleep-aid medication.
Overall, PROMIS-SD scores had a non-significant improvement from 58.68±10.58 to 58.19±12.89 (p=0.72) following SNM device implantation. Within-group analysis was performed to identify whether significant changes in sleep disturbance or additional PROMIS item banks occurred (Table 3). Individuals with improved sleep disturbance improvement did report statistically significant improvement in sleep disturbance following SNM device implantation with a mean change of −3.99 (95% confidence interval [CI], −6.32, −1.65; p<0.01), but did not have significant mean changes in PROMIS-PF −1.71 (95% CI, −5.99, 2.56; p=0.23), PROMIS-PI −2.16 (95% CI, −5.93, 1.62; p=0.16), or PROMIS-D −0.91 (95% CI, −3.40, 1.57; p=0.25). Those who did not have improvement of their PROMIS-SD t-score had only non-significant changes in all PROMIS item banks (Table 3).
Except for depression in the sleep disturbance improvement group, the mean pre-procedure PROMIS scores were worse than that of the general US population. Pre-procedure PROMIS-PF (38.86±2.35 vs. 34.13±5.58, p=0.07), -PI (60.04±6.34 vs. 65.50±6.20, p=0.13), -D (44.2±4.73 vs. 61.29±9.53, p=0.17), and -SD (59.14±6.27 vs. 58.21±14.67, p=0.88) were similar between the groups. Although there was a significant difference in the median t-score change in sleep disturbance between the groups (−4.1 vs. 1.6, p<0.01) following SNM implantation, mean post-procedure scores were similar (p=0.41). T scores following SNM were: -PF (37.14±5.10 vs. 35.44±4.74, p=0.53), -PI (57.89±5.08 vs. 64.73±7.35, p=0.07), -D (54.29±6.25 vs. 57.96±11.42, p=0.47), and -SD (55.16±8.49 vs. 61.21±16.32, p=0.41).
DISCUSSION
To the authors' knowledge, this is the first study investigating changes in sleep disturbance using the PROMIS-Sleep Disturbance item bank following SNM implantation for treatment of refractory OAB. Within our data, 50% (n=7) experienced improvement in self-reported sleep disturbance as measured by the PROMIS-SD item bank. Those with improved sleep disturbance experienced a statistically significant t-score change, with a mean change of −3.99 (95% CI, −6.32, −1.65; p<0.01). Surprisingly, there were no other statistically significant changes in depression (p=0.50), pain interference (p=0.31), or physical function (p=0.47) in those with sleep disturbance improvement.
Overall we were unable to identify a significant change in sleep disturbance in those treated with SNM for urinary symptoms. This is in contrast to other reports that found improvements in self-reported sleep after SNM implantation. Jairam et al. [12] found that sleep was significantly improved following SNM implantation for OAB (n=36) using the Dutch OAB-q. Likewise, Noblett et al. [13] found persistent improvement in self-reported sleep using the same questionnaire at 12 months following SNM implantation compared to baseline scores in 255 subjects followed prospectively for treatment of OAB. An explanation for this may be related to the design of the questionnaire itself. The Dutch OAB-q is a disease-specific questionnaire, which can often lead to overestimation of changes observed within an individual [28,29] while PROMIS item banks are designed IRT [19].
Demographics, clinical characteristics, and chronic psychiatric/medical comorbidities were similar between the groups. Despite some differences in mean pre- and post-procedure PROMIS t-scores that met the accepted 5-point definition of clinically relevant following SNM device implantation, none of these reached statistical significance. This is most likely due to the small sample size, cohort definitions, and the broad range of responses within each group. Appropriately, there was a statistically significant improvement in the median PROMIS-SD t-score (−4.1) in the improved group compared to an increased median t-score (+1.6) in the group without sleep disturbance improvement, p<0.01.
It should be noted that all of the mean PROMIS scores were worse than the general US population (t-score=50) before and after SNM device implantation. In a study evaluating mental health, sleep, and physical function using PROMIS item banks in women seeking care for LUTS, greater sleep disturbance (PROMIS-SD) was noted in a cohort of women reporting UI compared to those without UI (53.5±8.5 vs. 50.7±9.1, p=0.52) [23]. Similarly, Ge et al. [8] noted worse sleep disturbance (PROMIS-SD, 54.3±10.3 vs. 43.8±9.2) in those with OAB (n=51) compared to controls (n=30); however this was not statistically significant after adjusting for age, gender, and nocturia (p=0.21).
We were unable to further investigate factors that may have influenced sleep disturbance improvement due the limitations of data available within the EMR. The charts were reviewed for additional factors not included in the original database that may have influenced sleep disturbance. There was no documentation regarding the potential diagnoses of comorbidities that may affect sleep disturbance such as obstructive sleep apnea or insomnia, in any of the included subjects. None of subjects were taking medications to aid with sleep such as zolpidem or melatonin. A comparison of night time voids, total daily micturitions, and number of urge-associated incontinence episodes may provide valuable information into why only 50% of those included in this subanalysis experienced improvement of sleep disturbance.
Admittedly, this study has several other limitations due to its retrospective design. Data was collected as part of clinical practice with voluntary completion of PROMIS item banks before and after SNM implantation with collection possible at a limited number of clinics within the medical system. Additionally, the PROMIS-SD item bank is the last to be administered in our multispecialty adult pelvic health clinic which may have contributed to limited collection of post-procedure data. Only 35% of those with pre-procedures PROMIS-SD (n=40) data had completed the item bank after SNM implantation which may lead to selection bias. Generalizability is limited, but may be useful in Caucasian women considering SNM for treatment of OAB with similar baseline PROMIS scores.
The main strength of this study is the introduction to PROMIS-SD analysis following chronic SNM therapy for treatment of OAB. Investigation of PROMIS following interventions should continue as it has improved reliability to detect changes within an individual with smaller sample sizes required to come to an accurate conclusion [28]. Also the item bank scoring system provides a reference to the general US population (mean=50) increasing understanding of individual and group morbidity and changes reported within a population affected by multiple chronic conditions [30]. This study adds to our current understanding of the sleep changes one may or may not experience following SNM implantation and provide a framework and reference point for future investigation.
CONCLUSIONS
In conclusion, significant improvement in sleep disturbance following SNM implantation for refractory OAB occurred less commonly than anticipated. There were no notable associations noted between those with improved sleep disturbance and those without improved sleep disturbance. Further investigation of factors that affect sleep disturbance in women with OAB is needed to improve patient-centered care.

 XML Download
XML Download