

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Radical nephroureterectomy (RNU) is the gold standard treatment for localized upper tract urothelial carcinoma (UTUC) [1]. In some cases of UTUC, surgeons perform ureteroscopy (URS) preoperatively because it is hard to use only an imaging modality to determine whether the lesion is a real carcinoma or just a benign lesion mimicking a malignant one. Several reports have been published concerning the relationship between preoperative diagnostic URS and the rate of intravesical recurrence (IVR). One previous report of a meta-analysis showed the hazard ratio (HR) of preoperative diagnostic URS for IVR was 1.56 (p<0.001) [2]. Other reports, however, have not shown an association between preoperative diagnostic URS and IVR. In one study of 502 patients, of whom 206 underwent preoperative URS (Pre-U) and 296 did not (Non-U), Pre-U did not increase the risk for IVR (HR, 1.136; 95% confidence interval [CI], 1.00–1.30; p=0.059) [3]. Another meta-analysis showed that Pre-U before RNU did not negatively affect overall survival, recurrence-free survival, cancer-specific survival, or metastasis-specific survival [4]. Furthermore, some studies have reported efforts to reduce IVR during RNU by use of pirarubicin intravesical instillation [5].
URS procedures with or without manipulation including biopsy could influence the seeding or spillage of tumor cells. Also, there are other risk factors for IVR after RNU, such as lymph node invasion and tumor location [67]. Therefore, we investigated whether preoperative diagnostic URS before RNU had an impact on IVR over the long term in a single, large institution.
MATERIALS AND METHODS
1. Study population
This study was conducted in compliance with the Declaration of Helsinki and was approved by Seoul National University Bundang Hospital Institutional Review Board (approval number: B-1907-552-110). Written informed consent was omittable and the omission was also approved. Patients with UTUC who underwent RNU in a single institution from May 2003 to December 2018 were enrolled. Patients who had a history of bladder cancer before RNU, bilateral UTUC, and did not receive bladder cuff resection were excluded. Patients who had a minimum of 1 year of follow-up were enrolled. Accordingly, a total of 453 patients were finally enrolled in this study.
2. Data analysis
We divided the study population into two groups according to the presence of preoperative diagnostic URS (Pre-U group) or none (Non-U group). The following baseline parameters were compared between the Pre-U and Non-U groups: age, sex, smoking, Eastern Cooperative Oncology Group (ECOG) performance status, estimated glomerular filtration rate (eGFR, calculated by use of the Chronic Kidney Disease Modification of Diet in Renal Disease Collaboration formula) [8], tumor laterality, tumor location, hydronephrosis, diabetes mellitus, and hypertension.
We also compared the following perioperative variables and outcomes: operation method, operation time, estimated blood loss, transfusion rates (both perioperative and postoperative), T stage, lymph node invasion, grade, positive surgical margin, angiolymphatic invasion, presence of carcinoma in situ, URS biopsy, interval from Pre-U to RNU, and complications. Complications were defined according to the Clavien–Dindo classification [9]. Pathologic stages were assessed by using the Brierley et al. [10] guideline.
3. Operative method
The operative methods were open, laparoscopic, or robotic. The open method took a retroperitoneal approach with a flank incision. The laparoscopic method took a transperitoneal approach, with the camera port inserted at the rectus muscle margin and two other hand ports inserted. The robotic method also took a transperitoneal approach, with three ports inserted according to the laparoscopic method and a fourth arm port inserted under the xiphoid process. Two additional ports were inserted near the midline for suction, traction, Hem-o-lok or clip insertion, and needle insertion. A Gibson incision and bladder cuffing were also performed in all three methods. In half of the robotic RNU procedures, bladder cuff resection was done robotically. For the Pre-U group, both flexible and rigid URS were used. Flexible URS was performed when the suspicious lesion was hard to reach with rigid URS. Preoperative URS was not done if the patients had definite tumors in the urinary system and positive cytology results; however, the decision about whether to perform preoperative URS was mainly made by surgeon's preference due to legal issues.
4. Statistical analysis
To compare the clinicopathologic characteristics, perioperative outcomes, and renal function between the two groups, independent t-tests and chi-square tests were performed. For prediction of the factors that affect IVR, multivariate Cox logistic regression analyses were conducted. To compare cancer-specific survival and overall mortality between groups, Kaplan–Meier analyses were performed. All p-values were two-sided, and p<0.05 was considered statistically significant. Analyses were performed using the IBM SPSS Statistics version 19.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Of the 453 patients total, 226 patients (49.9%) had undergone diagnostic URS before RNU (Pre-U group), and 227 patients (50.1%) had not (Non-U group). The demographics and preoperative characteristics of the patients in each of the two groups are compared in Table 1. There were no significant differences between the groups in terms of age (65.85 vs. 66.98 years), sex (male, 68.6% vs. 72.7%), smoking (14.6% vs. 15.9%), ECOG performance status, or hypertension (54.9% vs. 46.8%). Preoperative tumor characteristics were comparable, with the exception of tumor location. The Pre-U group had a significantly higher rate of lower-location tumors (24.8% vs. 14.1%, p<0.001). The preoperative eGFR was significantly higher in the Non-U group (70.75 vs. 65.55 mL/min/1.73 m2, p=0.022).
1. Perioperative outcomes
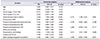
Perioperative outcomes in both groups are described in Table 2. In the combined patient group, 164 patients (36.2%), 143 patients (31.6%), and 146 patients (32.2%) received RNU via the open, laparoscopic, and robotic surgery methods, respectively, and there were no significant differences in operation method between the groups (p=0.393). There were also no significant differences between groups in terms of estimated blood loss (247.17 vs. 281.94 mL), rate of transfusion (16.4% vs. 22.5%), or complication rate (Clavien–Dindo classification grade ≥3, 3.1% vs. 4.0%, p=0.617).
2. Pathologic outcomes
In the patients who underwent RNU, there were 127 (28.0%), 147 (32.5%), and 168 (37.1%) patients with pathologic T1, T2, and T3 to T4 UTUC, respectively (Table 2). There was no significant difference in pathologic stage after RNU between the two groups (p=0.949). Of the 143 patients (31.6%) who received lymph node dissection during RNU for clinical N+ stage, 45 patients had lymph node invasion (22 [9.7%] in the Pre-U group vs. 23 [10.1%] in the Non-U group, p=0.721). Positive surgical margins were reported in 5.3% of patients in the Pre-U group and 7.9% of patients in the Non-U group (p=0.262). The Non-U group had significantly more angiolymphatic invasion (22.6% vs. 35.7%, p=0.002).
3. Intravesical recurrence
With a median follow-up duration of 452 months, IVR occurred in 99 patients (43.8%) in the Pre-U group and 61 patients (26.9%) in the Non-U group (p=0.001, Table 2). The 5-year IVR-free survival rates were 56.2% and 73.1% in the Pre-U group and Non-U group, respectively (log rank test, p<0.001, Fig. 1A). The univariate Cox proportional hazards model showed the following factors to be significant for IVR: tumor location (lower vs. others; HR, 2.038; p<0.001), preoperative hydronephrosis (HR, 1.433; p=0.046), hypertension (HR, 1.401; p=0.034), and Pre-U (HR, 1.638; p=0.002) (Table 3). After adjustment for these factors in the multivariate analysis, tumor location (HR, 1.775; 95% CI, 1.248–2.525; p=0.001) and Pre-U (HR, 1.413; 95% CI, 1.015–1.965; p=0.040) remained significant for IVR.
We performed additional subgroup analyses with an organ-confined subgroup (T2 or less) and a non-organ-confined subgroup (T3 or more). In the organ-confined subgroup, the univariate analysis showed the following factors to be significant for IVR: preoperative eGFR (HR, 0.984; p=0.017) and Pre-U (HR, 1.949; p=0.039) (Supplementary Table 1). After adjustment for these factors in the multivariate analysis, preoperative eGFR (HR, 1.959; 95% CI, 1.040–3.692; p=0.037) and Pre-U (HR, 0.984; 95% CI, 0.971–0.997; p=0.037) remained significant for IVR. However, in the non-organ-confined subgroup, the univariate analysis showed that the following factors were significant for IVR: tumor location (HR, 2.103; p<0.001), Pre-U (HR, 1.539; p=0.023), and presence of carcinoma in situ (HR, 1.580; p=0.047). After adjustment for these factors in the multivariate analysis, tumor location (HR, 1.836; 95% CI, 1.201–2.807; p=0.005) remained significant for IVR.
4. Other survival outcomes
Other oncological outcomes are also shown in Table 2. There were no significant differences between groups with respect to recurrence except for urinary system (32.3% vs. 36.6%, p=0.374) and cancer-specific mortality (5.8% vs. 8.4%, p=0.277). Overall mortality was higher in the Non-U group (7.1% vs. 13.2%, p=0.031). Cancer-specific survival was not significantly different between the two groups (Fig. 1B, C).
DISCUSSION
The purpose of the present study was to examine the relationship between preoperative diagnostic URS and IVR. Our results showed that Pre-U was an important factor in IVR during follow-up. The results of previous reports have been conflicting regarding the effect of Pre-U on IVR; however, our results showed a promising positive association between Pre-U and IVR. We also performed subgroup analysis according to tumor stage. In the group with organ-confined disease (T2 or less), Pre-U increased the HR, but this was not the case in the non-organ-confined subgroup (T3 or more). Perhaps tumor stage is an important factor, and this point needs further study. In summary, we found that Pre-U increased the HR of IVR. Other disadvantages may occur, but it is recommended that patients not undergo URS before surgery.
Data from Liu et al. [11] also suggested that diagnostic URS is more likely to result in IVR (HR, 1.592; 95% CI, 1.143–2.218; p=0.006). In that report, which included 81 Pre-U patients and 583 Non-U patients, multifocal tumor (HR, 1.596; 95% CI, 1.206–2.111; p=0.001) and tumor size <3 cm (HR, 1.459; 95% CI, 1.104–1.929; p=0.008) were also related to IVR [11]. Another retrospective study reported that diagnostic flexible URS is associated with an increased incidence of postoperative IVR (HR, 4.0; 95% CI, 1.4–11.9; p=0.01) [12]. In that study, in which the Pre-U group had 23 patients and the Non-U group had 73 patients, the rate of IVR was similar to the rate in our study (59% in the Pre-U group vs. 26% in the Non-U group compared with 43.8% and 23.6%, respectively, in our study) [12]. In a retrospective study by Luo et al. [13], with 115 Pre-U patients and 281 Non-U patients, diagnostic URS was related to IVR (40.9% vs. 27.8%, p=0.011). A multivariate Cox regression showed that Pre-U (HR, 1.44; 95% CI, 1.00–2.08; p=0.05) was associated with IVR [13]. Concurrent bladder cancer (HR, 2.98; 95% CI, 2.08–4.25; p<0.001) and multifocal tumor (HR, 1.48; 95% CI, 1.01–2.19; p=0.05) were also related to IVR [13]. Cancer-specific survival was not significantly different in Kaplan–Meier curves (p=0.526) [13]. Sankin et al. [14] reported that patients are at higher risk for IVR after RNU when they have undergone prior diagnostic URS (HR, 2.37; 95% CI, 1.34–4.20; p=0.003). In their study, however, which consisted of 144 Pre-U patients and 57 Non-U patients, cancer-specific survival, metastasis-free survival, and overall survival were not significantly affected. Several studies have reported results similar to ours [1516].
In the meta-analysis by Marchioni et al. [2], there seemed to be a significant association between the use of diagnostic URS and increased risk for IVR (HR, 1.56; 95% CI, 1.33–1.88; p<0.001). The data in that study were based on six studies identified from PubMed, Ovid, and Scopus, with a total of 820 Pre-U patients and 1,770 Non-U patients. The other systemic review and meta-analysis based on PubMed, Web of Science, and EMBASE, which included eight studies, also reported that Pre-U before RNU increases the risk of IVR (HR, 1.51; 95% CI, 1.29–1.77; p<0.001) [4]. However, none of the following were associated with Pre-U: cancer-specific survival, overall survival, recurrence-free survival, or metastasis-free survival [4].
There are several theories to explain the occurrence of IVR after RNU. Intraluminal tumor seeding, intraepithelial cancer migration, and urinary tract cancerization are among the theories for how URS could increase the risk [1317]. During URS, irrigation increases the intrapelvic pressure to greater than 50 cm H2O [18]. The manipulation by URS that increases intrapelvic pressure may promote pollination of cancer cells [19]. A distal tumor location increases the HR, and we assumed that distally located tumors were near the bladder, thus increasing the possibility of seeding. However, research comparing proximally and distally located tumors is limited, and further study should be conducted.
This study had several limitations. First, this was a retrospective cohort study. Second, we did not validate our results with multicenter data. Other limitations could be the presence of microscopic, concurrent bladder cancer. Although we excluded patients with a previous history of bladder cancer, there could be some portion of cancer cells in the bladders of some patients. The URS was selectively done in cases of a mimicking situation, where the radiographic image was not definite; therefore, the lack of guidelines for Pre-U could be another limitation. We excluded patients whose duration of follow-up was less than 1 year because we needed a longer follow-up duration to find IVR. The overall mortality rate differed between the two groups; however, this could have been due to the nature of the retrospective method and the small event number of deaths. The patients who did not receive preoperative URS had relatively definite tumor lesions on the radiologic image, and this could have affected the results although the pathologic outcomes were not significantly different. Therefore, our findings should be validated in a future prospective study.
CONCLUSIONS
Preoperative diagnostic URS before RNU was a significant factor in IVR. Therefore, we should carefully consider preoperative diagnostic URS before RNU for nonobvious ureteral lesions. Rather, it is better to not perform URS before surgery. These results should be validated in a prospective study.




 XML Download
XML Download