

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although blood transfusion is an important life-saving procedure performed according to level of anemia in both patients with malignancies and those with various underlying benign conditions, it carries a significant risk for unfavorable outcomes, including incompatibility, possibility for infection transmission, coagulopathy, and allergic reaction [12]. In particular, curative surgery for malignancy is always associated with the risk for massive bleeding; therefore, the probability of blood transfusion may also increase. However, the results of several meta-analyses have consistently indicated the existence of a negative association between perioperative blood transfusion (PBT) and oncologic outcomes, including tumor recurrence and survival, in surgically treated patients with various malignancies, including stomach, lung, liver, and colorectal cancer [34567]. Although the mechanism underlying this unfavorable association is not fully understood, it is hypothesized that immune modulation and inflammatory responses caused by PBT adversely affect oncologic outcomes after radical surgery for cancer [128].
Several trials have also evaluated the effect of PBT on oncologic outcomes after radical surgery in the field of urologic oncology, including bladder, prostate, and kidney cancer [91011121314151617]. Nephrectomy using the radical or partial approach is the standard treatment for nonmetastatic renal cell carcinoma (RCC). Previous reports have shown that rates of PBT range from 10% to 20% and that PBT is associated with worse postoperative outcomes, such as higher recurrence and higher risk for death in patients with localized RCC who underwent nephrectomy [14151617]. However, evidence is scarce regarding the prognostic role of PBT in the Asian RCC population.
In the current study, we aimed to verify the prognostic role of PBT in terms of oncologic outcomes and to elucidate the factors related to the receipt of PBT in a large single-center cohort consisting of Korean RCC patients treated with curative surgery.
MATERIALS AND METHODS
1. Study population
This study design and the use of patients' information stored in the hospital database were approved by the Institutional Review Board (IRB) at Seoul National University Hospital. The approval number is H-1407-197-600. We received exemption from getting informed consent by the IRB because the present study was a retrospective study, personal identifiers were completely removed, and the data were analyzed anonymously. Our study was conducted according to the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
After IRB approval from Seoul National University Hospital, we reviewed the nephrectomy database comprising 2,538 patients who underwent radical or partial nephrectomy for a renal mass from 2000 to 2014. Of these patients, those with incomplete information about PBT, insufficient data on patient demographics, pathologies other than RCC, or metastatic disease at the time of surgery were excluded from the study. Finally, 2,329 patients with nonmetastatic RCC were included in our analysis.
2. Acquisition and definition of data
Radical or partial nephrectomy was performed by several surgeons during the study period. The following preoperative clinical factors were considered: presence or absence of symptomatic presentation, age at surgery, sex, body mass index (BMI; defined as the body weight [in kilograms] divided by the square of height [in meters]), preoperative serum hemoglobin (Hb) and creatinine (Cr) level, smoking status, Eastern Cooperative Oncology Group (ECOG) performance status, hypertension (HTN), diabetes mellitus (DM), and end-stage renal disease (ESRD). Surgery-related parameters included surgical approach (laparoscopic: transperitoneal, retroperitoneal, or hand-assisted/open/robot-assisted), surgical method (radical or partial), operation time, and estimated blood loss (EBL). Tumor-related factors included histologic subtype (clear cell vs. non-clear cell), tumor stage (pT1/T2/T3/T4), Fuhrman nuclear grade (Gr1-2/3/4), tumor size, pseudosarcomatous component, tumor necrosis, and nodal status (pN0/N1/Nx). All pathologic specimens were processed in accordance with institutional standard procedures and were evaluated by expert genitourinary pathologists depending on a standardized reporting protocol. PBT only included transfusion of allogeneic packed red blood cells (pRBCs) during nephrectomy or within the preoperative or postoperative hospitalization period. Because there were no unified institutional criteria with regard to the thresholds for PBT, transfusion was determined at the discretion of the surgeons depending on biomarkers such as patient's anemia level and blood pressure.
3. Follow-up protocol
After surgery, patients were usually followed up every 6 months for the first year and then yearly for 5 years with routine blood examination and imaging studies (chest roentgenography or computed tomography [CT] and abdominopelvic CT scan or magnetic resonance imaging). The endpoints of this study included recurrence-free survival (RFS), cancer-specific survival (CSS), and overall survival (OS). RFS was defined as the duration from the time of surgery to the first time of tumor recurrence. The duration of CSS or OS was calculated as the period from the date of surgery to the date of RCC-related or any-cause death, respectively. Patients who lived with or without RCC were censored from the survival analyses. The date of death was identified by reviewing medical charts or from the annual census of the Korea National Statistical Office. Reason of death was confirmed by the physicians in charge and from death certificates.
4. Statistical analyses
The included parameters were compared between transfused and nontransfused patients using chi-squared or Fisher's exact tests for categorical variables and the Mann–Whitney test for continuous variables. Continuous variables are expressed as the median and interquartile range (IQR); categorical variables are denoted as absolute numbers and relative percentages. The preoperative factors related to the receipt of PBT were evaluated using univariate and multivariable logistic regression analysis. The estimation and comparison of survival outcomes according to the receipt of PBT was assessed by using the Kaplan–Meier method with a log-rank test. Finally, the impact of PBT on each survival outcome was evaluated using multivariable Cox proportional-hazards models. All analyses were performed with IBM SPSS Statistics version 21.0 (IBM Corp., Armonk, NY, USA), and two-sided p-values of <0.05 were considered to be statistically significant.
RESULTS
1. Baseline characteristics of the study cohort
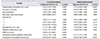
The characteristics of the study cohort and comparative results for each parameter according to the receipt of PBT are listed in Table 1. Among all patients, PBT was performed in 275 patients (11.8%) with a median unit of 3 pRBCs (IQR, 2–5). Compared with the non-PBT group, those who received PBT were more likely to be older, to be female, and to have more frequent symptomatic presentation, lower BMI, lower preoperative Hb level, higher preoperative Cr level, worse ECOG performance status, higher frequency of HTN, higher frequency of DM, higher frequency of ESRD, higher percentage of open and radical approach, longer operative time, more advanced tumor stage, higher nuclear grade, larger tumor size, and more frequent pseudosarcomatous component, tumor necrosis, and nodal invasion (all p-values <0.05). Moreover, the PBT group showed a higher EBL (median, 700 mL; IQR, 300–1,200 mL) compared with the non-PBT group (median, 200 mL; IQR, 100–300 mL; p<0.001). There was a significant difference in the median follow-up duration between the PBT and non-PBT groups (35 vs. 47 months; p<0.001). Univariate and multivariate logistic regression analysis demonstrated that symptomatic presentation, advanced age at surgery, higher preoperative serum Cr, and lower preoperative Hb level were independent preoperative risk factors for PBT (all p<0.05) (Table 2).
2. Impact of PBT on survival outcomes after surgery for RCC
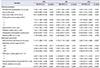
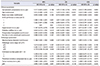
Postoperative recurrence was observed in 235 patients (10.1%), with a median time to recurrence of 39 months (IQR, 17–60 months). A total of 228 patients (9.8%) died of any causes, within a median follow-up period of 45 months (IQR, 24–74), and 150 deaths (6.4%) among these were directly associated with RCC (Table 1). Kaplan–Meier analysis using the log-rank test revealed that the PBT group had worse 5-year RFS (65.1% vs. 91.2%, p<0.001), OS (71.4% vs. 92.8%, p<0.001), and CSS (74.0% vs. 95.5%, p<0.001) compared with the non-PBT group (Fig. 1). However, in the multivariable Cox regression analyses incorporating other clinicopathologic variables in the entire study cohort, PBT was not a significant predictor of RFS, OS, or CSS (Table 3). Multivariable Cox proportional-hazards analyses of the PBT group alone (n=275) showed that an increased number of pRBC units was an independent predictor of worse OS (hazard ratio [HR], 1.043; 95% confidence interval [CI], 1.008–1.078; p=0.016) and CSS (HR, 1.066; 95% CI, 1.033–1.100; p<0.001), but not of RFS (HR, 0.986; 95% CI, 0.936–1.038; p=0.587) (Table 4).
3. Subgroup analyses
Additional subgroup analyses were conducted by RCC histologic subtype (clear cell versus non-clear-cell RCC). Kaplan–Meier plots with the log-rank test suggested there were no significant differences in RFS, OS, and CSS regardless of RCC histologic subtype (Supplementary Fig. 1). In addition, when multivariable Cox regression analyses were conducted to identify the predictors of each survival outcome in each RCC histology group, PBT was not a significant predictor of survival outcomes in either group (Supplementary Tables 1 and 2). Tumor diameter in clear cell RCC (Supplementary Table 1) and lymph node involvement (pN1) in the non-clear-cell RCC group (Supplementary Table 2) were significant predictors of all survival outcomes.
DISCUSSION
Generally, the prognosis, including recurrence and mortality, of cancer patients is primarily determined by tumor-related factors such as tumor stage, nuclear grade, tumor size, and histologic subtype [1819]. Other than these factors, several clinical factors have also been suggested in association with cancer prognosis [1819]. Among these, blood transfusion using allogeneic pRBC units has been extensively examined in various types of cancer, and these studies have suggested a deleterious effect on prognosis [34567]. In addition to the combined impact of surgery and anesthesia-induced immunosuppression, administration of blood products can further aggravate the immunosuppressive status of cancer patients, resulting in transfusion-related immune modulation (TRIM). Although the mechanism has not been fully clarified, the effects of TRIM may be mediated by the suppression of cytotoxic cell and monocyte activity, an increase in suppressor T-cell activity, and the release of a variety of immunosuppressive and inflammatory cytokines, such as prostaglandins, interleukins, interferon-gamma, and transforming growth factor-beta 1, which are induced by various antigens, such as white blood cells and soluble human leukocyte antigen peptides included in allogeneic blood products [28]. These immunosuppressive and inflammatory responses caused by TRIM are thought to promote tumor growth and metastasis and adversely affect the prognosis of cancer patients [28].
The prognostic role of PBT has also been investigated in the field of urologic oncology, including RCC [91011121314151617]. Several retrospective trials demonstrated that in bladder cancer patients treated with radical cystectomy, PBT is associated with increased overall mortality and morbidity [911], and in prostate cancer patients undergoing radical prostatectomy, whereas allogeneic PBT is a significant predictor of worse postoperative biochemical recurrence and survival outcomes, autologous PBT is not [12]. Recent meta-analyses confirmed these associations of PBT with adverse oncologic outcomes in bladder and prostate cancer patients treated with radical surgery [1013]. In the case of RCC, several retrospective studies have reported a negative relationship between PBT and oncologic outcomes. Linder et al. [14] reported that in 2,318 patients with localized RCC who underwent curative nephrectomy including 498 transfused patients (21%), allogeneic PBT was a significant predictor of increased risk of overall mortality, and in those who received PBT alone, an increase in the number of transfused pRBC units was independently associated with worse OS. Tsivian et al. [15] also reported that allogeneic PBT was associated with approximately a twofold increase in the risk of metastatic progression, all-cause mortality, and RCC-specific mortality. One retrospective analysis that included 1,168 RCC patients treated with nephrectomy reported that when analysis was conducted according to the timing of blood transfusion (117, intraoperative; 81, postoperative), intraoperative allogeneic blood transfusion, but not postoperative blood transfusion, was significantly associated with increased risks for postoperative cancer recurrence and mortality [16]. In addition, a recent meta-analysis noted that PBT was a significant predictor of worse OS in patients with nonmetastatic RCC who underwent nephrectomy [17].
This consistent negative association of PBT and RCC-related oncologic outcomes was identified in the current study In our study, PBT of allogeneic pRBC in RCC patients was significantly associated with adverse clinical and pathologic features, such as older age, worse ECOG performance status, more advanced tumor stage, higher nuclear grade, larger tumor size, more frequent pseudosarcomatous component, tumor necrosis, and nodal invasion (Table 1). This result agrees with the results of previous reports [1415]. However, although PBT was a significant predictor of worse survival outcomes in the Kaplan–Meier analysis (Fig. 1), the statistical significance of this association was not confirmed in the multivariable Cox regression analysis with adjustment for well-known prognostic factors of RCC (Table 3). This might be the result of confounding effects due to the prognostic factors more frequently included in the PBT group. To avoid these confounding effects, we conducted an analysis that included only RCC patients receiving PBT. That analysis demonstrated that an increased number of transfused pRBC units was significantly associated with worse OS and CSS. This negative relationship between transfusion volume and cancer prognosis was also identified previously [914]. Therefore, we suggest that for patients with a higher likelihood of receiving blood transfusion, such as those with symptomatic presentations, advanced age, and lower preoperative Hb levels, efforts are required to reduce allogeneic PBT, including the use of preoperative autologous blood collection with or without acute normovolemic hemodilution technique and its intraoperative transfusion, autologous blood transfusion via intraoperative cell salvage techniques, and recombinant human erythropoietin, to improve postoperative survival outcomes [22021].
This study had some limitations as follows. First, owing to the retrospective study design, a selection bias is likely. Thus, unidentified confounding factors might have affected our findings. For instance, we did not investigate or include comorbidities other than HTN and DM, such as cerebrovascular or cardiovascular disease, which might adversely affect survival outcomes. Second, as mentioned earlier, because PBT was administered at the discretion of each surgeon without specific criteria, it is possible that unnecessary PBT might have been performed, with detrimental effects on clinical outcomes. Third, only allogeneic pRBC was considered as a blood product for PBT. Therefore, we did not evaluate the effect of autologous blood transfusion and other blood products, such as fresh-frozen plasma or platelet concentrates on oncologic outcomes. However, according to previous reports, there is currently no clear evidence that autologous blood transfusion has an advantage over allogeneic blood transfusion in terms of cancer prognosis or regarding the influence of other blood products on cancer prognosis [2]. Fourth, blood transfusion was considered as perioperative administration and was not divided into preoperative, intraoperative, and postoperative administration owing to the retrospective nature of the study. If analyzed according to the timing of transfusion, the prognostic role of blood transfusion might be different, as reported in the previous studies [1622]. Last, although the number of enrolled patients in the current study was larger than in previous retrospective studies, the prognostic impact of allogeneic PBT on RCC-related outcomes derived from this study should be explored further through well-designed prospective clinical trials.
CONCLUSIONS
Our data imply that PBT may have an adverse effect on RFS, OS, and CSS in patients with nonmetastatic RCC treated with curative surgery, although a significant correlation was not identified in the multivariable analyses. Particularly, an increase of pRBC units in transfused patients may be problematic considering the high possibility of worse OS and CSS. Therefore, for RCC patients who are likely to receive PBT, such as those with symptomatic presentations, older age, lower preoperative Hb, and high preoperative Cr level, efforts to limit the overuse of PBT seem imperative to improve postoperative survival.



 XML Download
XML Download