

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Precision medicine is a novel paradigm in clinical practice that determines personalized treatment based on a patient's genetic and environmental factors. Before it can be applied clinically; however, precision medicine still has many issues to overcome. A massive amount of genetic and clinical data is required for the implementation of precision medicine, and recent advances in next-generation sequencing (NGS) make implementation more likely [1].
Compared with other sequencing platforms, NGS technology is beneficial in obtaining large-scale genetic information using single inputs [2]. Although whole-genome and whole-exome sequencing techniques yield more information, targeted NGS (tNGS) is more promising for clinical application because of its cost-effectiveness, rapid sequencing time, and deep sequencing read depth [3]. Because various solid cancers share major molecular pathways, the pan-cancer panel may provide additional useful information for specific cancers [45]. Routine application of pan-cancer panels is not a distant prospect. For example, MSK-IMPACT™ (Memorial Sloan Kettering, New York, NY, USA) and Foundation One are Food and Drug Administration (FDA)-approved multi-cancer NGS panels designed to obtain genetic information on various malignancies that can be applied for therapeutic purposes.
Prostate cancer is the most common malignancy in men and a major cause of cancer-related mortality in Western countries [678]. Geographic and racial differences in the incidence and disease characteristics of prostate cancer suggest that genetic and environmental factors affect disease development and progression [9]. With advances in genetic analysis, genetic factors in prostate cancer development and progression have been exponentially studied over the past decade [9101112]. However, most genetic studies have focused on metastatic or castration-resistant prostate cancer. Furthermore, almost all genetic studies constituted a negligible proportion of the Asian population [1314].
Therefore, we performed a pan-cancer panel assay that contained prostate cancer-related genes for locally advanced prostate cancer in the Korean population. By performing a comparison with The Cancer Genome Atlas (TCGA) database, we aimed to find racial differences in Korean patients that result in aggressive tumor behavior. Using combined clinical data and genetic alterations, we performed univariate and multivariable analysis to evaluate potential risk factors for biochemical recurrence.
MATERIALS AND METHODS
1. Ethics approval and informed consent
This study was approved by the Seoul National University Hospital (SNUH) Institutional Review Board (IRB) (approval number: 1706-103-860). The prospectively collected registry was approved by the SNUH IRB (approval number: 1506-121-682) for use of clinical data for scientific purposes. Informed consent for NGS analysis was obtained from each participant. Fresh frozen tissues were stored in the SNUH biobank. All experiments were performed in accordance with relevant guidelines and regulations.
2. Patient selection
All patients were selected from a prospective, multidisciplinary, and biobank lined cohort, the Seoul National University Prospectively Enrolled Registry for Prostate Cancer-Radical Prostatectomy (SUPER-PC-RP) [15]. This prospective cohort collects comprehensive clinical information, including functional and oncological outcomes, patient-reported quality of life, and bio-specimens. We selected 20 patients with locally advanced prostate cancer at stage T3a or T3b without metastasis. Patients underwent radical prostatectomy from March 2016 to June 2016, with a follow-up of 25.6 months (median). We used tumor and normal tissues collected from the operating room or frozen biopsy room and immediately stored the removed prostates at −195℃ in liquid nitrogen at the SNUH Cancer Tissue Bank.
3. Cancer panel information
The SNUH cancer panel, named the FIRST-panel versions 3 and 3.1, was used for this analysis. This panel contains exons of 183 genes, specific introns of 23 fusion genes, the TERT promoter region, 8 MSI markers, and 45 drug target regions, with a total length of ~1.949 Mbp. We assessed the FIRST-panel composition for major urological malignancies—prostate, bladder, and kidney cancers. We determined prostate cancer-related genes on the basis of a literature review [11121617] and finally selected 40 prostate cancer-related genes, including AR, FOXA1, TMPRSS2, and ERG, in the FIRST-panel v3.0. and 3.1. Among these targets, we reviewed potentially applicable targets for prostate cancer from the OncoKB database [18].
4. DNA extraction
Fresh frozen tumor tissues were homogenized and lysed with proteinase K. Next, total DNA was isolated from each target with the Maxwell 16 CSC DNA Blood kit (Promega Corp., Madison, WI, USA). The extracted DNA was quantitated by use of a Quantus fluorometer (Promega Corp.) and Agilent 4200 TapeStation system (Agilent Technologies, Santa Clara, CA, USA).
5. Capture library preparation
After DNA was extracted paired-end libraries were prepared with an Agilent SureSelectXT Target Enrichment System kit for the Illumina paired-end sequencing library protocol using SNUH FIRST Cancer Panel v 3.0 and v 3.1, according to the manufacturer's instructions. The quality of the DNA library was evaluated by using a Bioanalyzer 2100 (Illumina Inc., CA, USA) and DNA 1000 chips (Illumina Inc., CA, USA).
6. Next-generation sequencing
The tNGS was performed by using the Illumina Hiseq 2500 platform. Sequencing data were transformed as FASTQ files, and quality control by use of FASTQC (0.11.8) and Trimmomatic (0.33) software. BAM formation after alignment was performed based on the reference genome (GRCh 37) by BWA (0.7.12) and Picard (1.134). Quality control of the BAM file was carried out by SamTools (v1.2) and GATK (v3.3). Detection of SNPs was performed by MuTect (1.1.7) and SamTools (v1.2). Indel and copy number variation (CNV) detection were performed by IndelGeontyper (0.36.3336) and CoNIFER software (0.2.2). Fusion search was done using Delly (0.7.2). All data were converted to VCF format and annotated by Annovar.
7. Variant prevalence comparison of SNUH pan-cancer data and TCGA prostate cancer
We downloaded MAF files of prostate adenocarcinoma (TCGA-PRAD) variants from the National Cancer Institute (NCI) Genomic Data Commons (GDC) data portal. From these MAF files, we extracted variants in the following genes: SPOP, ERG, NRG1, KMT2D, MAP3K1, TSHR, FANCD2, ATM, FANCA, BRAF, FANCG, NOTCH4, and AR. Four MAF files were submitted for their corresponding variant callers: MuSE, Mutect2, VarScan2, and SomaticSniper. We selected the variants that occurred in at least two of these files. We classified the mutations into three categories: missense truncating and inframe mutation. The prevalence of such mutations was compared with our FIRST-panel data.
8. Statistical analysis
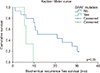
We set biochemical recurrence as the primary endpoint. The prostate-specific antigen (PSA) value at the secondary confirmative level of >0.2 ng/dL was considered biochemical recurrence. Univariate analysis of biochemical recurrence was carried out by using the Kaplan–Meier curve with log-rank test. Known and potential risk factors, including age, initial PSA value, Gleason score at the time of biopsy, prostate volume, pathological Gleason score, pathological T stage, pathological N stage, intraductal carcinoma, and perineural invasion, were selected for univariate analysis to assess the risk of biochemical recurrence. Among the genetic alterations, the 10 most frequently occurring mutations in the genes SPOP, KMT2D, ATM, BRAF, FANCA, FANCD2, FANCG, MAP3K1, TSHR, and ERG fusion were selected for analysis. TP53 and PTEN were also included in the univariate analysis, as their association with biochemical recurrence has been reported [1920]. The variables showing a p-value <0.1 in the univariate analysis were selected for multivariate analysis using the Cox proportional hazard model. Important variables, such as Gleason grade group and T stage, were also included in the multivariate analysis. Statistical analysis was conducted by use of IBM SPSS Statistics 22.0 (IBM Corp., Armonk, NY, USA), and a p-value <0.05 was considered significant.
RESULTS
1. Patient characteristics
The patients' demographic and clinical characteristics are presented in Table 1. Two patients previously treated by neoadjuvant androgen deprivation therapy underwent radical prostatectomy. Eighteen patients underwent pelvic lymphadenectomy, and five patients showed lymph node metastasis in the pathologic examination of permanent sections. The average number of extracted and positive lymph nodes was 17.7 and 2.7, respectively. The average follow-up period was 25.6 months, and only one patient died of pneumonia. During the follow-up period, 14 patients were detected with biochemical recurrence and needed salvage treatments.
2. Sequencing quality control
DNA was extracted from all 20 fresh frozen tissue samples for library preparation and cancer panel analysis. In total, 26,066,448 to 39,586,410 bases were read for this analysis. Average coverage was 574.5±304.1×, ranging from 160 to 996. Average values of coverage above 50 and above 100 were 97.5±2.0% and 94.2±3.9%, respectively. All samples passed sequencing quality control analysis.
3. Pan-cancer panel report
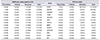
A total of 99 mutations were detected in the pan-cancer panel analysis. Mutations in the SPOP gene, detected in 25% of patients, were the most frequently occurring mutations. Mutations in KMT2D (20%), FANCA, FANCD2, FANCG, TSHR, MAP3K1, BRAF, and ATM (15%) also occurred frequently. ERG fusion was detected in 20% of patients that had mutually exclusive SPOP mutations. The fusion partners of ERG were TMPRSS2 (m/c, 21q22.3), SLMAP (sarcolemmal membrane-associated protein gene, 3p14.3), or SETD4 (SET domain-containing protein 4, 21q22.13). On average, 5 mutations were detected per patient, ranging from 1 to 13 (Fig. 1). Additionally, a patient was detected with only one mutation in the BRAF gene, coding for an amino acid change in K601E (a potential target of PLX8394), at an allele frequency of 0.45. Integrative analysis of the cancer panel is shown in Fig. 2.
We found potential actionable targets for prostate cancer treatment in nine patients (45.0%) in this study. ATM mutations, the target of olaparib, were the most common actionable mutations detected in three patients. Moreover, three patients had BRAF gene alterations, of which two had changes in K601E. Another patient had a mutation in the CDKN2A gene, which is a therapeutic target of abemaciclib, palbociclib, and ribociclib. Mutations in each of FGFR1 and FGFR3 was detected in one patient, which are potential targets of AZD4547, BGJ398, Debio1347, and erdafitinib.
4. Comparison with the TCGA database
Among the 11 selected genes (SPOP, KMT2D, ATM, BRAF, FANCA, FANCD2, FANCG, MAP3K1, TSHR, NOTCH4, and AR), 10 genes were expressed more frequently in our data than in TCGA, with the exception of AR (Table 2). SPOP and KMT2D mutations showed a >5% incidence rate in the TCGA database. In contrast, MAP3K1, FANCD2, TSHR, ATM, FANCA, BRAF, FANCG, and NOTCH4 were detected at a <5% incidence rate. Among these mutations, MAP3K1 (N749K), FANCD2 (V941A), TSHR (R310H), FANCA (G917R, R1011C, A816V), BRAF (K601E), and FANCG (P187Q) were likely to be pathogenic mutations with a Combined Annotation Dependent Depletion (CADD) score of over 20. The BRAF mutation was the only confirmed mutation present in other platforms, such as the Clinvar and OncoKB databases.
5. Univariate and multivariate analysis with clinical parameters
Clinical and pathologic features, as well as genetic alteration data from the pan-cancer panel, of locally advanced prostate cancer were analyzed for their contribution to biochemical recurrence. The results of the univariate analysis are shown in Table 3. The Kaplan–Meier curve with a log-rank test of BRAF mutation is presented in Fig. 3. The multivariate Cox regression analysis revealed that prostate volume (hazard ratio [HR], 0.12; 95% confidence interval [CI], 0.01–0.74; p=0.02), pathological Gleason grade group (HR, 4.11; 95% CI, 1.14–14.88; p=0.03), and BRAF mutation (HR, 9.84; 95% CI, 2.27–149.18; p=0.03) showed a statistically significant association with biochemical recurrence (Table 4).
DISCUSSION
In this study, we successfully performed a pan-cancer panel analysis in patients with advanced prostate cancer. We achieved an average depth of over 500, coupled with a high sensitivity that allowed detection of a low allele frequency mutation (TP53, allele frequency=0.02, missense mutation). The SNUH pan-cancer panel detected less commonly reported mutations compared with previous studies undertaken in Western countries, which may be due to racial differences. Among these mutations, the BRAF mutation was found to be an independent prognostic factor for biochemical recurrence of prostate cancer.
We successfully detected 99 genetic alterations, including structural variations using pan-cancer panel analysis. The general mutation expression profile was similar to that reported by another researcher. The SPOP mutation and ERG fusion were the most common findings and were mutually exclusive as reported previously [11]. The most common ERG fusion partner was TMPRSS2; two additional fusion partners, SLMAP and SETD4, were also detected, which were not reported previously. SLMAP is known to interact with serine/threonine-protein kinase 24. The mutation in this region was related to the Brugada syndrome. SETD4 is a coding gene related to histone modification. Additionally, some rare genetic alterations were frequently detected in our study. For example, SNPs or Indels in MAP3K1, FANCD2, TSHR, ATM, FANCA, BRAF, FANCG, and NOTCH4 genes occurred at <5% frequency in the TCGA database [1117]; however, they were relatively common in our study with frequency ranging from 15% to 20%. Among these differentially expressed genetic alterations, six were potentially pathogenic according to their CADD score; however, only the BRAF mutation (K601E) was confirmed to be pathogenic as per the Clinvar and OncoKB databases. This discrepancy may be due to the small number of Asians studied during the preparation of the TCGA database.
Because the incidence and behavior of prostate cancer is quite different in Western and Asian patients, there could be predisposing genetic differences between the two patient groups. Prostate cancer is less frequently diagnosed but shows more aggressive features in Asians compared with Western population [2122]. A recent large-scale genetic study, comprising 65 whole-genome and 145 targeted sequences in Chinese patients with prostate cancer, observed considerable differences compared with TCGA databases [21]. This discrepancy suggests that there are underlying genetic differences among different races in prostate cancer development and behavior. In our study, multivariate analysis showed that BRAF mutation (HR, 9.84; p=0.03), Gleason grade group (HR, 4.11; p=0.03), and prostate volume (HR, 0.12; p=0.02) demonstrated significant association with biochemical recurrence. BRAF is a serine/threonine kinase family member, and alterations in this gene are commonly reported in malignant melanoma [23] and papillary thyroid cancer [24]. BRAF is a component of mitogen-activated protein kinase (MAPK) pathways, which play a major role in tumorigenesis. The incidence of BRAF mutations in prostate cancer shows considerable racial differences. According to the genetic analysis data mainly collected from white populations [25], BRAF mutations are rare in prostate cancer in Western populations. However, the incidence of alterations in the BRAF gene in the Asian population is relatively high. Cho et al. [26] reported that approximately 10% of Korean patients have BRAF mutations in prostate cancer. Genetic studies performed in a Chinese population also detected a higher incidence of BRAF gene alterations [27]. In this study, we observed that 15% of patients had BRAF-mutation-positive prostate cancers, indicating that BRAF mutation is an independent prognostic factor for biochemical recurrence. Owing to the different behavioral and pathological features of prostate cancer owing to racial/ethnic differences, we suggest that the BRAF mutation may contribute to this discrepancy to some extent.
We discovered five potential therapeutic targets in nine patients (45%); however, they were not FDA-approved in prostate cancer. Each of the ATM or BRAF mutations was present in 3 patients. ATM is one of the DNA repair-related genes, such as BRCA1, BRCA2, ATM, Fanconi anemia gene, and CHEK2, which are targets of poly-adenosine diphosphate ribose polymerase (PARP) inhibitor. Olaparib is a PARP inhibitor that has shown promising results in a patient with prostate cancer harboring a defective DNA repair gene in a Phase 2 clinical trial. BRAF mutation is a target for the FDA-approved drugs vemurafenib and dabrafenib in malignant melanoma. However, no studies to date have focused on prostate cancer treatment. Prostate cancer caused by BRAF mutation is classified as I to II, manifested by kinase activity, Ras-dependency, and dimerization status. BRAF class is important to predict MAPK target therapy response. K601E mutation is a class II BRAF mutation, which is sensitive to MEK inhibitors and vemurafenib in malignant melanoma. The pan-BRAF inhibitor, PLX8394, is a potential drug for targeting BRAF (K601) mutation.
This study had several limitations. One important limitation was the small sample size. Because of the small size, the statistical power of this study was not enough to establish clinical importance of the studied genes. Since we utilized tNGS for genetic analysis, genomic alterations in the regions of interest of our cancer panel could not be detected. Therefore, recently discovered genetic alterations associated with biochemical recurrence could not be assessed. In this study, we undertook retrospective analysis from a prospectively collected cohort, and this approach has a potential risk of bias. The natural course of prostate cancer is relatively slow; thus, a short follow-up period (25.6 months) is another limitation. Despite these limitations, we successfully conducted tNGS using a pan-cancer panel with excellent depth (>500).
CONCLUSIONS
In conclusion, a pan-cancer panel, comprising prostate cancer-related genes, is a useful tool for evaluating genetic alterations in patients with locally advanced prostate cancers. Our results suggest that the BRAF mutation is associated with biochemical recurrence in the Korean population. Nevertheless, a well-designed large-scale investigation is needed for a better understanding of this mutation.





 XML Download
XML Download