

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Microscopic radical resection (R0) is a key predictor of long-term outcome in patients with non-metastatic pancreatic cancer.12 Borderline resectable and locally advanced tumors can involve adjacent organs or vascular structures. Thus, they potentially require extended pancreatectomy to achieve a curative radical resection.3456 Over the past decades, heterogeneous definitions of extended pancreatectomy and the indiscriminate use of the terms “extended pancreatectomy” and “multi-visceral resection” have led to a lack of evidence in terms of indications, surgical outcomes and oncological long-term results for this procedure. In 2014, the International Study Group for Pancreatic Surgery (ISGPS) established an unequivocal definition of ‘extended distal pancreatectomy’ as a standard distal pancreatectomy (DP) associated with resection of any of the following involved organs: gastric resections, colonic or small bowel resections, left adrenal gland, left kidney, diaphragm, contiguous liver. Major arterial or venous resections were also included in the definition.3 Nevertheless, the indications for extended DP are still controversial, particularly in the era of neoadjuvant treatments, with only heterogeneous data available to assess its results.
We present here a case of a locally advanced tumor of the pancreatic tail wherein extended DP with combined multi-visceral resection and thoracic wall resection was performed after a long-course downstaging, along with a brief literature review.
Go to : 
CASE
A 53-year-old previously healthy man, American Society of Anesthesiologists 2, complained of epigastric abdominal pain irradiating to the left flank, associated with 8 kg weight loss and low-grade fever over the last 3 months.
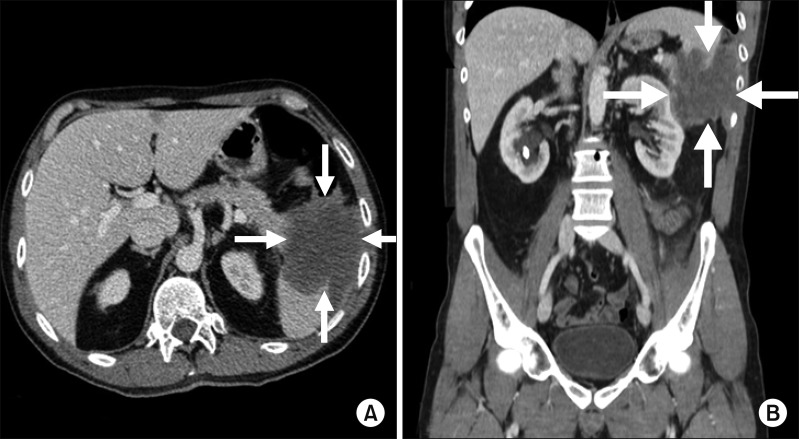
Physical examination revealed left upper quadrant abdominal tenderness with no rebound. No jaundice was present. Tumor markers were within normal range with serum carbohydrate antigen 19-9 (CA 19.9) 4.5 U/ml (normal value (n.v.) <27 U/ml) and serum carcinoembryonic antigen (CEA) 1.2 ng/ml (n.v. <5 ng/ml). Contrastenhanced computed tomography (CECT) showed a bulky tumor in the left flank, measuring 95×96×75 mm, which involved the tail of the pancreas, the spleen, the splenic flexure of the colon, the left kidney and the left adrenal gland (Fig. 1). A massive retroperitoneal infiltration was present, with extension to the lateral abdominal wall and to the lower ribs. No distant metastasis were detected. The mass was histologically confirmed as biliary-pancreatic tumor by a colonoscopic biopsy. The 18-FDG-PET confirmed elevated metabolic activity of the mass along with enhanced FDG uptake on the left thoracic wall and left anterior costovertebral angle. The patient was diagnosed with locally advanced pancreatic cancer of the pancreas tail at the institutional multidisciplinary board, and referred to neoadjuvant treatment. He underwent systemic chemotherapy with FOLFIRINOX (folinic acid 400 mg/m2, fluorouracil 2,400 mg/m2, irinotecan180 mg/m2 and oxaliplatin 85 mg/m2). Overall, 12 cycles were administered, two of which with dose reduction to 80% because of neutropenia.
Beside the above-mentioned side effect, chemotherapy was well tolerated and the time between the beginning of treatment and the last cycle was uneventful, except for one episode of fever and abdominal pain, likely due to a pericolonic abdominal collection with possible colonic leakage as confirmed by the CECT scan. The episode required inpatient conservative treatment with broad spectrum intra-venous antibiotic.
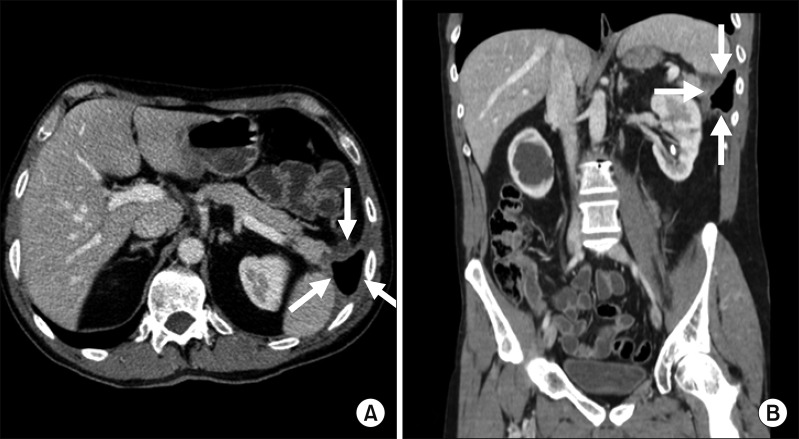
At the CECT for the reevaluation after chemotherapy, the mass was significantly reduced in size, even though borders were barely discernable (Fig. 2). The MRI with paramagnetic contrast confirmed the infiltration of the retroperitoneum, the left perinephric fat and the thoracic wall up to the muscular layer. Tumor markers were still low, with Ca 19.9 4.0 U/ml (n.v <27 U/ml) and CEA 2.5 ng/ml (n.v <5 U/ml).
At the institutional tumor board reevaluation after chemotherapy, once the long-course effective neoadjuvant treatment was considered, curative surgery was planned, although R0 resection still seemed to require extended distal pancreatectomy with resection of contiguous organs including the thoracic wall. Surgery was scheduled for 17 days after the end of chemotherapy.
Neither peritoneal dissemination nor distant metastasis was found at laparotomy. After entering the lesser sac by dividing the gastrocolic ligament the tumor was found to involve the pancreatic tail, the spleen, the splenic flexure of the colon, the left perinephric tissues, the diaphragm and the thoracic wall. The left colic vessels were identified and divided and both the transverse colon and the descending were transected with a linear stapler (Echelon Flex™ GST system, Ethicon® US, LLC) (Fig. 3A). The splenic artery and splenic vein were divided and the splenophrenic ligament was dissected. Once the retropancreatic tunnel was developed, the pancreas was transected by a reinforced stapler (Echelon Flex™ GST system, Ethicon® US, LLC) (Fig. 3B, C). The left renal artery, vein and ureter were divided (Fig. 3D, E) and the left kidney, together with the perinephric fat, was separated up to the iliopsoas plane. A left thoracotomy was performed and the latissimus dorsi muscle was divided (Fig. 4A). After dividing the intercostal muscles and bundles, the 9th and 10th ribs were identified and transected anteriorly and posteriorly to the tumor's infiltration (Fig. 4B). Pancreatic dissection was then extended to the left and around the tumor, including part of the lateral diaphragm (Fig. 4C). The resected thoracic wall was eventually removed en bloc with the specimen (Fig. 4D). Lymph node stations 8a, 8p, 9, 12a, 12p and 12b were selectively sampled. Because of the contaminated field due to the pre-operative collection and the colonic resection, the use of a mesh was unadvisable. Thoracotomy was directly repaired, as well as the diaphragmatic defect (Fig. 4E). Two running absorbable sutures were used for the end-to-end colonic anastomosis and one closed-system suction drain was left in close proximity to the tumor bed. The overall operative time was 390 minutes and no blood transfusions were required. Patient was admitted to the Intensive Care Unit for 24-hour monitoring and eventually transferred to the ward.
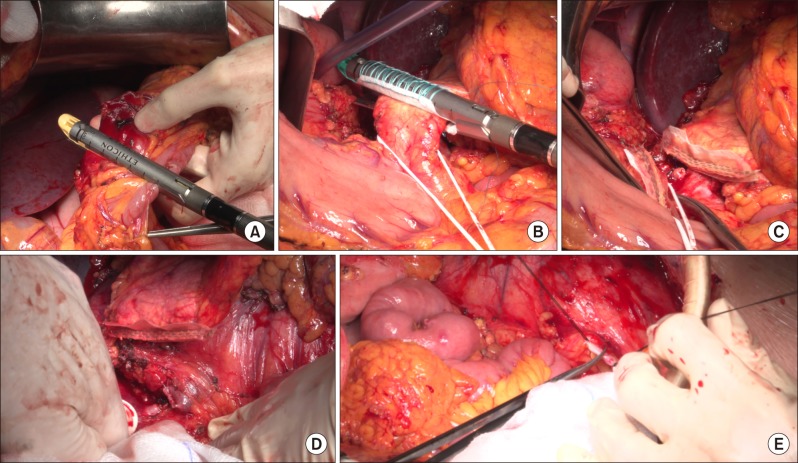 | Fig. 3(A) The transverse colon was transected with a linear stapler. (B) The pancreatic transection was performed by a reinforced stapler. (C) Closure of the pancreatic stump. (D) Left renal artery and vein were divided. (E) Left ureter was identified and divided.
|
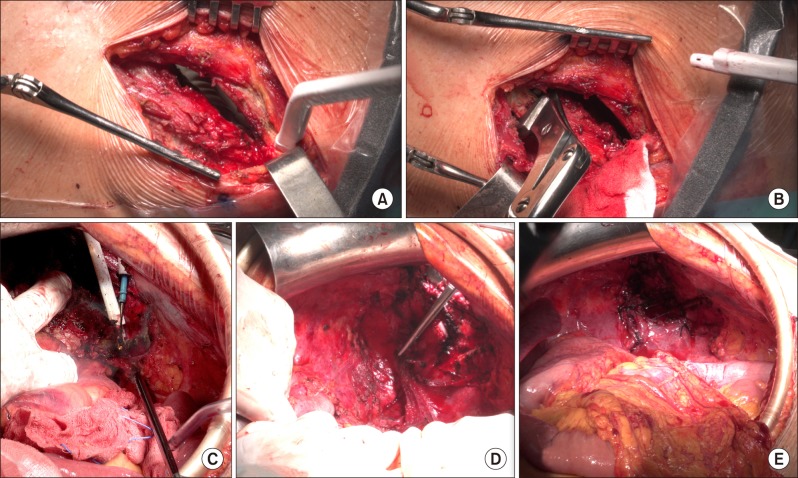 | Fig. 4(A, B) Left thoracotomy was performed and the 9th and the 10th ribs were transected. (C) Pancreatic dissection was extended to left up to the thoracic wall. (D) The specimen was removed en bloc and a wide diaphragmatic defect was observed. (E) The thoracotomy and the diaphragmatic defect were directly repaired.
|
The early post-operative course was uneventful and patient was discharged on post-operative day (POD) 7. He was subsequently readmitted on POD 17 because of fever associated with upper abdominal pain and a CT scan evidence of an abdominal sub-phrenic collection. The treatment consisted of a percutaneous drainage, and amylases rich fluid was collected. Patient was diagnosed with grade B post-operative pancreatic fistula (POPF)7 and finally discharged. The percutaneous drain was removed on POD 29 at the outpatient clinic.
Final pathology showed complete response of the pancreatic cancer. No viable tumor cells could be identified in the specimens and all margins of resection were negative for tumor infiltration (R0) (Fig. 5). Tumor stage was pT0, pN0 (0/41), M0.
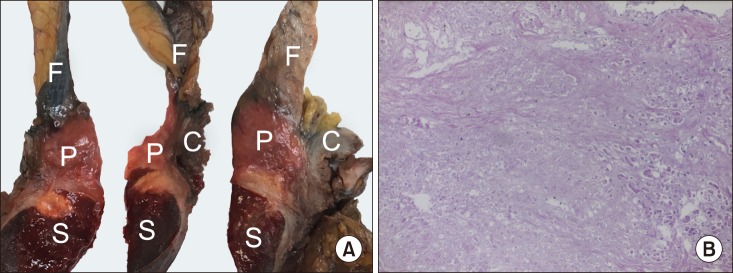 | Fig. 5(A) The macroscopic analysis (A) of the specimen included the tail of the pancreas (P), the spleen (S), the left kidney, the left colonic flexure (C) the left adrenal and the thoracic wall resection. Peripancreatic fat (F) is also shown. (B) Histological exam with H&E stain revealed complete response with diffuse fibrosis. No viable tumor cells were detected.
|
At the 6-month post-operative follow-up, the patient was doing well and no recurrence of disease was detectable at the CECT scan.
Go to :
DISCUSSION
Indications and outcomes of extended pancreatectomy have been barely investigated and no definitive conclusions have been drawn. Beside providing unambiguous definitions for different types of extended pancreatectomy, the International Study Group for Pancreatic Surgery (ISGPS) aimed to assess post-operative surgical and oncological outcomes of the procedure. Despite the heterogeneity of the available data, they concluded that the long-term survival provided by extended pancreatectomy for pancreatic cancer was similar to that of standard pancreatectomy, with 3-year OS ranging from 16% to 19.4%. However, increased duration of surgery, blood loss, need for transfusions and overall morbidity, along with longer duration of ICU stay and hospital stay were reported.3 Particularly, overall morbidity was assessed between 42% and 60% after extended pancreatectomy, and between 34% and 58% after standard pancreatectomy.
A subsequent large retrospective monocentric analysis on 611 consecutive cases by Hartwig et al.6 confirmed a considerable reduction of perioperative outcome for patients undergoing extended pancreatectomy,8 with surgical morbidity of 42.7% (vs 34.2% among those undergoing standard pancreatectomy) and 30-day mortality of 4.3%. A similar decrease in post-operative outcome was reported by Schwartz et al.,9 when colectomy was associated to standard pancreatectomy, with 30-day morbidity increasing from 37% to 54% and mortality from 2% to 9%. Nevertheless, in a recent study, Mitra et al. found no significant differences in peri-operative morbidity (37% vs 29%) and mortality (6% vs 4%) among patients undergoing extended pancreatectomy when compared to standard pancreatectomy, and similar conclusions were reported by Low et al.10 by analyzing a small retrospective cohort.
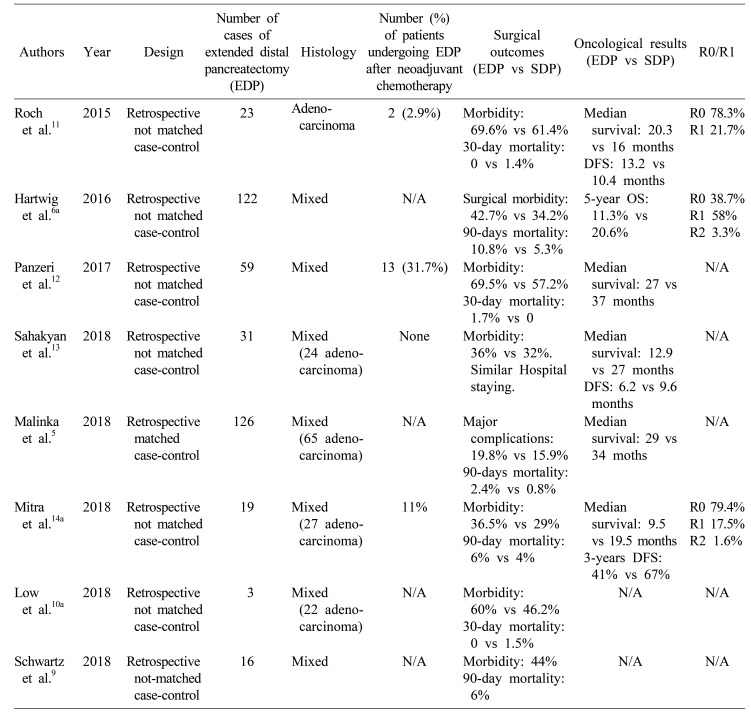
Other series only focused on indications and outcomes of extended DP. Roch et al.11 compared patients undergoing standard DP with those undergoing extended DP in a retrospective analysis. They concluded that similar morbidity and mortality were found between the two groups as well as comparable oncological results. Panzeri et al.12 reported acceptable morbidity and long-term survival among patients undergoing DP associated with multi-visceral resections. Finally, in a retrospective case-matched analysis by Malinka et al.5 no differences in terms of complications and survival between standard DP and DP combined with multi-visceral resections were detected. Table 135691011121314 summarizes the studies including series of extended DP and published subsequently to the ISGPS group consensus paper (2014).
Despite the definition provided by the ISPGS group, firm conclusions about indications and outcomes of extended DP are yet to be reached, partially due to the misleading use of the terms ‘multi-visceral resection’ and extended DP, which included also major vascular resections. Many of the reported series analyzed both extended pancreaticoduodenectomy and extended DP, without providing any subgroup analysis and often including both pancreatic ductal adenocarcinoma and non-malignant diseases. Moreover, none of them focused on the role of neoadjuvant treatments, neither as possible selection tool for surgery nor as a potential predictor of outcome.
Neoadjuvant strategies such as chemotherapy and radiotherapy have shown to have a key role in terms of disease control and effective downstaging, with excellent rates of subsequent radical resections.15161718
It is well accepted, therefore, that patients with locally advanced or borderline resectable pancreatic cancer should undergo neoadjuvant treatments at first, with upfront surgery remaining a viable option mainly for those with resectable tumors. Despite the lack of evidence supporting the role of neoadjuvant therapy for bulky tumors with involvement of adjacent organs,19 preoperative downstaging might be helpful in these cases too, by reducing the tumor burden, minimizing the extension of surgical resection and eventually increasing the chance to achieve negative margins. However, once maximized, long-course neoadjuvant treatments have been applied, as in the case we reported, surgical resection represents the last curative option, even though patients still have locally advanced tumors with invasion of contiguous organs. In this setting, challenging and technically demanding surgeries like extended pancreatectomy, with major vascular resections or resection of adjacent organs, should be considered, and the limit of resection might be tailored on every single case.
Highly selected patients with borderline resectable and locally advanced pancreatic tumors affecting adjacent structures might be eligible for extended pancreatic resections, particularly after pre-operative maximized neoadjuvant treatment and following a multidisciplinary evaluation. In high-volume centers with ample experience in pancreatic surgery, extended pancreatectomies represent a viable curative chance with acceptable post-operative morbidity and mortality. Challenging tailored extended resections might be taken into account, as an attempt to achieve negative margins.
Go to :
 XML Download
XML Download