

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With the development of minimally invasive surgery, abdominal endoscopy has been extensively used in the diagnosis and staging of malignant tumors of the abdominal cavity12 Recent interest in laparoscopic surgery for intraperitoneal surgery, There has been a comparative study of laparotomy and laparoscopic surgery.34 Laparoscopic surgery has advantages such as reduction of hospital days, reduction of intra-operative hemorrhage, and reduction of complications. Laparoscopy has become the basic procedure for cholecystectomy due to the development of the technique.567 Despite the increase in laparoscopic surgery, there is a different opinion on which operation is beneficial between the laparoscopic and open surgery in distal pancreatectomy (LDP vs. ODP).8 Pancreatectomy requires caution because serious complications such as pancreatic fistula can occur. The aim of this study was to compare preoperative and postoperative laparoscopic and open surgery in distal pancreatecomy in benign, pre-malignant, and low grade malignant pancreatic tumors.
Go to : 
MATERIALS AND METHODS
Patients and clinical review
We conducted a retrospective review of all patients who underwent laparoscopic and open distal pancreatectomy from January 2008 to December 2018 performed at Chonnam National University hospital, Gwangju & Hwasun, Jeollanam-do, Korea (n=150). All pancreatectomies were performed by experienced hepatopancreatic and biliary surgeons. All clinical, operative and pathological data were abstracted from patient's medical records. Other laparoscopic surgery for pancreatic malignancy and pancreatic procedures were excluded from this study. We reviewed each patient's history for age, sex, pathologic diagnosis. Specific outcomes that were includeed hospital stay, operative time (in minutes), operative blood loss (in milliliters), 30-day major morbidity and mortality (Clavian-Dindo classification), pancreatic leak rate (grade of leak A, B, or C), pancreatic hemorrhage, delayed gastric emptying, wound complication and readmission.
Definition
Per International Study Group on Pancreatic Fistula910 recommendations, pancreatic leak is defined as the case when the concentration of amylase in drained fluid measured at 3 days after surgery is more than three times the serum concentration, and even if fluid collection is observed around the pancreas in postoperative imaging. Grade of pancreatic leak is also in accordance with International Study Group on Pancreatic Fistula definitions. A grade A POPH (BL) no longer is considered a true pancreatic fistula or an actual complication. The BL has by definition no clinical impact, therefore, does not affect the normal hospital course. Grade B, this grade refersto a properly defined fistula involving increased amylase activity in the fluid from drain in association with a clinically relevant condition. Leakage is manipulation of surgical drains or intervention for percutaneous drainage into a peri-pancreatic fluid collection. Patients maybe kept with holding oral food and fluids and supported with enteral or parenteral feedings. If reoperation is needed or organ failure occurs, the fistula shifts to a grade C. Grade C leak is one that involves major change in the patient's management likely use of somatostatin analogues, intravenous antibiotics, intensive care unit admission, and/or reoperation.
An International Study Group of pancreatic Surgery (ISGPS) recommend postpancreatectomy hemorrhage (PPH) grade.11 PPH grade A has no major clinical impact and should not be associated with delay of hospital discharge. Grade B will lead to therapeutic consequences such as need for transfusion, ICU care, and potential invasive therapeutic interventions. It will prolong the hospital stay. Grade C should always be considered potentially life threatening. Immediate diagnostic and therapeutic consequences are needed. The hospital stay of Grade C is always prolonged.
Laparoscopic method
We perform LDP in the following manner. Under general endotracheal anesthesia, in the supine position with pads beneath the back. Trocars were performed with a four-trocar technique (two 12-mm trocars and two 5-mm trocars). The pneumoperitoneum through the umbilical 12 mm scope trocar. Other trocars were placed under direct scope vision.12 The locations of the trocars are shown in Fig. 1. Two 5 mm trocars (one locates the RUQ area for operator use and the other locates the left. Flank area for assistance) and two 12 mm trocars (one locates the umbilicus area for camera port and the other locates the mid-clavicular line parallel to the camera port for the operator's right hand). The table is placed in a reverse-Trendelenburg position to displacement of the transverse colon and small bowel from the field. Great omentum dissection from transverse colon. The lesser sac is opened by the lysis of the vascular plane between the transverse colon and the greater omentum to exposure pancreas body and tail. Lift the stomach posterior wall and fix the fundus, body, and antrum to the abdominal wall using the prolene 1-0. After fixation, the common hepatic and splenic arteries were seperated from the superior border of the pancreas. The inferior border of the pancreas was dissected carefully. Open the window at the isthmus between the anterior surface of the portal vein and the posterior part of pancreas. The window is completely dissected, and the isthmus is encircled and retracted with cotton tape. LDP with splenectomy, first the splenic artery and, then, splenic vein were ligation by Hemo-lock. The pancreas was transected with a triple row stapler. If the case is splenic preservation, the splenic artery and vein were dissected from isthmus toward the hilum of the spleen. If injuries occur during the vessel preservation process, perform vessel ligation near the spleen hilum. Take care not to damage the short gastric arterybranch and the left gastroepiploic artery branch at this time.
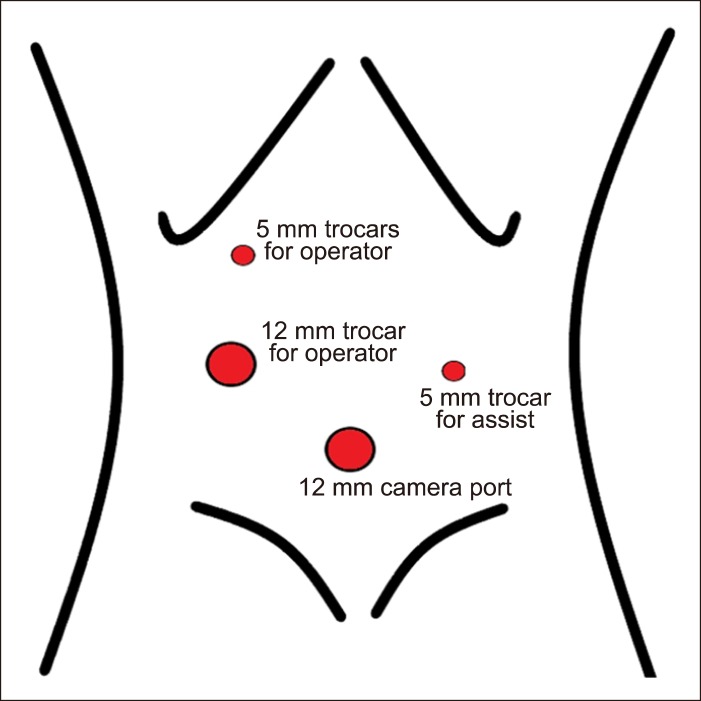 | Fig. 1Placement of trocars for LDPR. Two 5 mm trocars (one locates the RUQ area for operator use and the other locates the left. Flank area for assistance) and two 12 mm trocars (one locates the umbilicus area for camera port and the other locates the midclavicular line parallel to the camera port for the operator's right hand).
|
Statistical analysis
Statistical analysis was performed using IBM SPSS tatistics ver. 23.0 (IBM Co. Armonk, NY, USA). The categorical variables were expressed as number and percentage and were compared between groups using the chi-square testor Fisher exact test as appropriate. Continuous variables were presented as median (range) using the Mann-Whitney U-test. A p-value of <0.05 was considered to indicate statistical significant.
Go to :
RESULTS
Baseline characteristics of patients
From 2008 to 2018, there were 150 patients underwent distal pancreatectomy with or without splenectomy for benign pancreatic disease. 81 patients underwent open and 69 patients underwent LDPR (involves laparoscopic spleen preserving distal pancreatectomy, Warshaw, distal pancreatico-splenectomy). One patients in the LDPR group had open conversion due to bleeding. The clinico-pathologic characteristics are presented in Table 1. There were no significant differences in the age, sex, BMI, history of pancreatitis and pancreas thickness between the two groups. The ASA score (p=0.04) and pathology finding (p=0.042) was significant differences between the two groups.
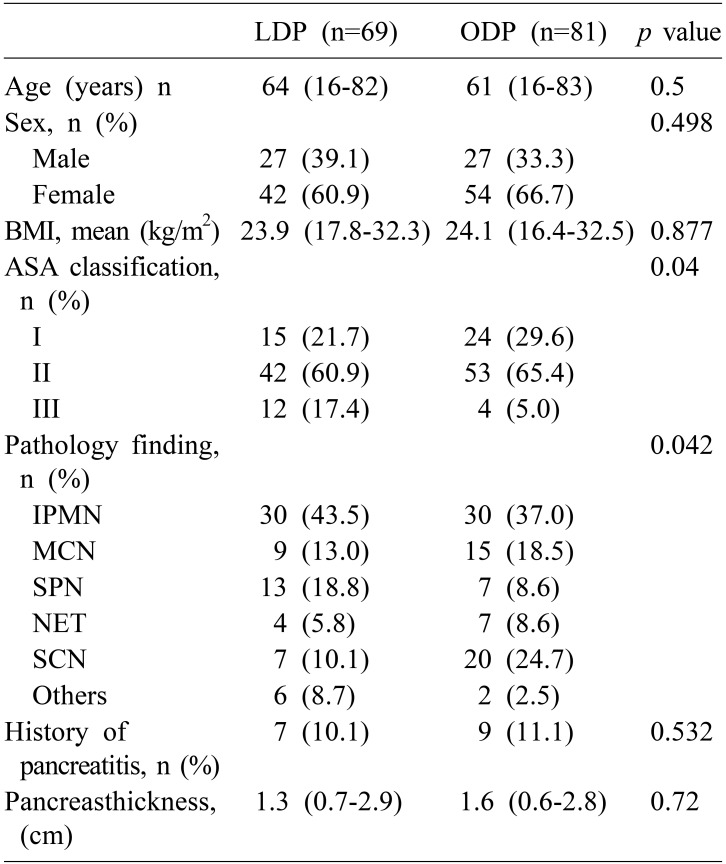
Table 1
Baseline characteristics of patients
LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy; BMI, body mass index; ASA, american society of anesthesiologists; IPMN, intraductal papillary neoplasm; MCN, mucinous-cystic neoplasm; SPN, solid pseudopapillary neoplasm; NET, neuroendocrine tumor; SCN, serous-cystic neoplasm
![]()
Operative parameters
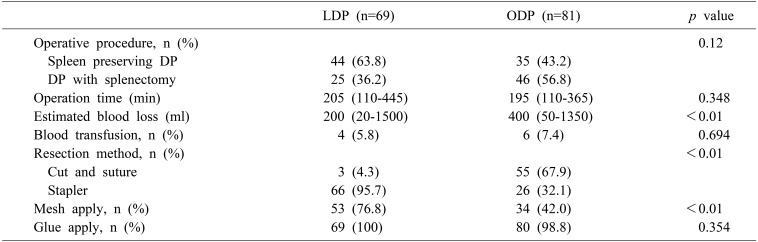
Operative parameters are shown in Table 2. LDP with spleen preserving was planned in 44 of the 69 patients (63.8%). LDP with splenectomy was 36.2% (25/69) because of difficulty control of bleeding and/or difficulty dissecting the splenic vein and tumor. OPD with spleen preserving was planned in 35 of the 81 patients (43.2%). ODP with splenectomy was 56.8% (46/81). This was done for the same reasons as LDP with splenectomy. The operation time of the LDP group was slightly longer than that of the OPD group, but there was no statistically significant difference between the two groups (205 vs. 195 min, p=0.348). Intra-operative estimated blood loss was significantly lower in the LDP group than in the OPD group (200 vs. 400 ml p<0.01). There was no difference in blood transfusion between the two groups. There was a significant difference in the resection method between the two groups (p<0.01) and there was a significant difference in the use of mesh for prevention of postoperative pancreatic fistula (POPF) (53 vs. 34 p<0.01).
Postoperative outcomes and complications
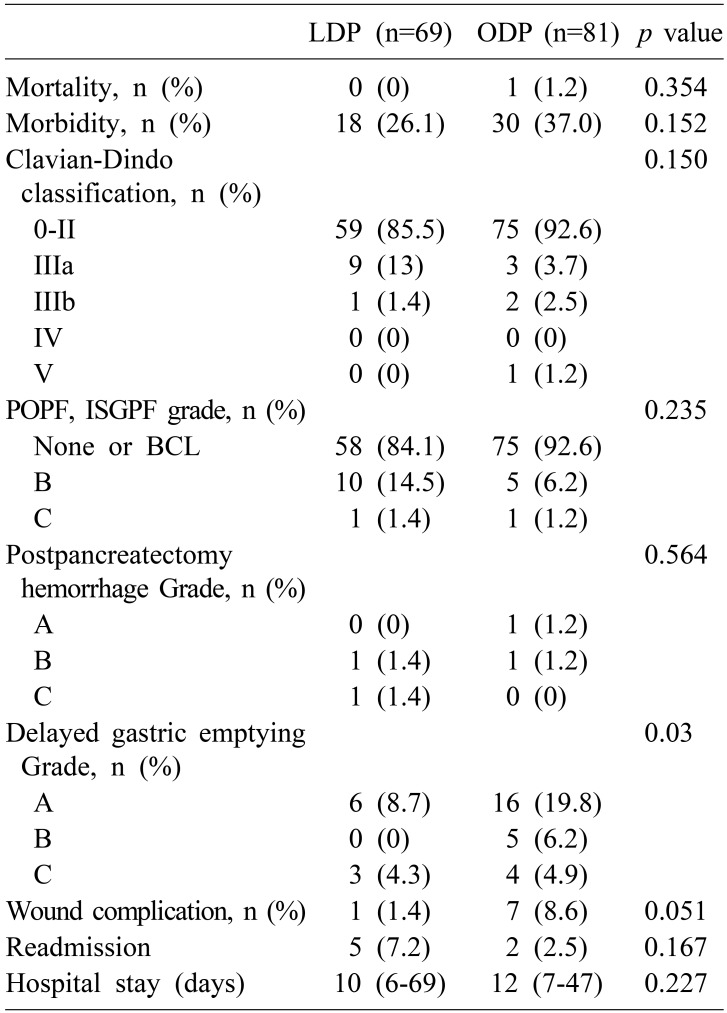
As shown in Table 3, POPF defined by the ISGPF classification system, 10 patients (14.5%) in the LDP group and 5 patients (6.2%) in the ODP group developed grade B fistula. One patient in each group was found to be grade C, there was no significant difference in incidence between the two groups (p=0.235). In the LDP group, 1 case occurred in the ODP group while the mortality was zero. Overall morbidity defined as Clavian-Dindo classification more than grade II developed in 10 patients (14.4%) in the LDP group and 6 patients (7.4%) in the ODP group. Severe complications of grade IIIb or more were more common in the LDP group (1.4% vs. 3.7%). There was no significant difference in the morbidity rate between the two groups (18 vs. 30 p=0.152). There were also no significant differences in the other complications. including post - pancreatectomy hemorrhage, wound infection, hospital stay and readmission. When comparing the two groups in terms of delayed gastric emptying, it can be known that LDP group occurred less than in the ODP group. From the point of view of feeding advance, LDP is more advantageous than ODP. In summary, there was a difference in the method of resection between the two groups and the use of mesh for the prevention of POPF, but there was no difference in the occurrence of POPF. In contrast, intra-operative blood loss was significantly lower in the LDP group than in the ODP group, and LDP was also significantly better in the view point of the feeding advance. In other words, LDP is safer and more favorable to patients than ODP.
Go to :
DISCUSSION
Laparoscopic surgery is predominant in the surgical field with minimal invasive surgery. In particular, laparoscopic surgery is less hospital stay, less pain, and less complication than open surgery.13 Our study, laparoscopic group showed longer operation time but less estimated blood loss than the open group. There was a difference in the method of resection between the two groups and the use of mesh for the prevention of POPF, but there was no difference in the occurrence of POPF. According to Hayashibe et al.14 study, distal pancreatectomy with mesh reinforced stapler was thought to be favorable for the prevention of clinically relevant POPF. Our study yielded different result, which may be due to the fact that the number of patients included in our study was more than twice as large compared to their study. In our study, there were no differences in the morbidity, post-pancreatectomy hemorrhage grade, wound complication, and hospital stay between the two groups.
In a recent meta-analysis study, there was a report that the LDP group had lower blood loss, shorter hospital stay, and faster patient recovery than ODP.15161718 The first multicenter study of minimal invasive distal pancreatectomy versus open distal pancreatectomy (LEOPARD) was reported.19 According to their report, minimal invasive distal pancreatectomy (MIDP) reduces the time to functional recovery compared with open distal pancreatectomy (ODP). From this point of view, similar results were obtained in our study. In our study, when comparing the two groups in terms of delayed gastric emptying, it can be known that LDP group occurred less than in the ODP group. From the point of view of feeding advance, LDP is more advantageous than ODP. However, in our study there was no significant difference between the two groups in terms of hospital stay (10 vs. 12, p=0.227).
Resently, the major complication (Clavian-Dindo grade≥III) and POPF (grade≥B) rate hve been reported as 8–38% and 11–39% for LDP and ODP.1020 When compared with this, our study showed the Clavian-Dindo grade≥III complication rate was 14.4% after LDP vs. 7.4% after ODP but Clavian-Dindo grade≥IIIb complication rate was 1.4% after LDP vs. 3.7% after ODP. POPF grade≥B was seen 15.9% after LDP vs. 7.4% after ODP. Comparing our study results to existing study result, we can see that the results are better. However, it is difficult to say that this result is absolute because the number of our study population is relatively small.
In conclusion, intra-operative blood loss was significantly lower in the LDP group than in the ODP group, and LDP was also significantly better in the view point of the feeding advance. There were no significant differences were found in the morbidity, POPF grade, postpancreatecomy hemorrhage, wound complication and hospital say, LDP should be the first line treatment for benign pancreatic disease.
Go to :
 XML Download
XML Download