

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since the introduction of laparoscopic pancreaticoduodenectomy (LPD) in 1994 by Gagner and Pomp,1 many studies have demonstrated its safety and feasibility.2,3,4 However, owing to the technical complexity of the procedure, surgeons require sufficient training to develop skills for laparoscopic surgery.5,6
In general, PD comprises resection and reconstruction. Several issues are associated with the resection and reconstruction phases of LPD.7 Particularly, in benign and low-grade malignant tumors of the pancreas requiring PD, the remnant pancreas is associated with soft pancreas and small pancreatic ducts, which is the biggest risk factor for postoperative pancreatic fistula (POPF).8,9,10 Laparoscopic reconstruction of the remnant pancreas following the laparoscopic resection of the pancreaticoduodenal component is difficult. Skillful techniques and long surgical experience are required. Hence, a robotic surgical system may improve the surgical performance, safety, and effectiveness.
Robotic surgery has overcome the limitations of laparoscopic surgery.11 The advantages of robotic surgery, such as a minimized fulcrum effect, three-dimensional operative view, unrestricted instrument motion, and no involuntary tremors, enable surgeons to perform the surgery with ease and comfort.12,13 However, the high cost of a robotic surgical system is a great obstacle to its application in clinical practice, as only the commercial da Vinci Surgical System is available.
Fortunately, several robotic surgical systems have been developed to date.14,15,16,17 Recently, Meerecompany Inc. in Korea successfully manufactured a robotic surgical system called Revo-i. In recent studies, Chang et al.18 and Kang et al.19 performed robotic prostatectomy and cholecystectomy, respectively, using Revo-I, without any serious complications in the first human clinical trial. Finally, Revo-i was commercialized after obtaining the approval from the Korean Food and Drug Administration (KFDA).
Lately, we successfully conducted a robot-assisted minimally invasive PD (laparoscopic resection and robotic reconstruction) using Revo-i. Here, we report our first experience with Revo-i PD in a patient with insulinoma and discuss the current limitations and future of robotic surgery.
Go to : 
CASE
Case presentation
A 65-year-old woman was referred to our hospital for a pancreatic head tumor, detected as an incidental finding during a routine check-up. The patient had been treated for hypertension and had no family history of cancer. However, she reported of frequent neuroglycopenic symptoms during fasting conditions. There were no physical abnormalities, and her body mass index was 26.04 kg/m2. The laboratory data indicated a slight elevation of the level of insulin to 25.47 IU/ml (reference range: 1.0–10.7) and C-peptide to 4.60 ng/ml (reference range: 0.6–2.3), but no other abnormal findings. The tumor marker values were within the normal ranges: carcinoembryonic antigen 0.97 ng/ml and cancer antigen 19-9, 7.6 U/ml. Preoperative imaging (Fig. 1) revealed a pancreatic uncinate process tumor measuring 13 mm with no other significant focal lesions, suggesting a neuroendocrine tumor.
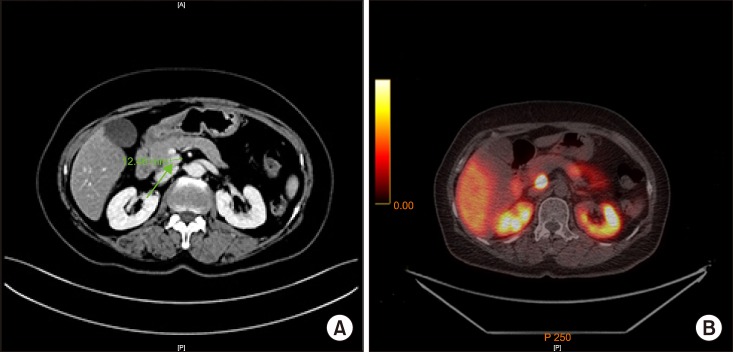 | Fig. 1Preoperative imaging. (A) Contrast abdominopelvic computed tomography revealed pancreatic uncinate tumor measuring around 13 mm in diameter, with no other focal lesions. (B) Positron emission tomography-computed tomography Ga-68 DODTATOC demonstrated significant focal intense DOTATOC uptake in the uncinate process of pancreas, suggesting neuroendocrine tumor.
|
Surgical procedure
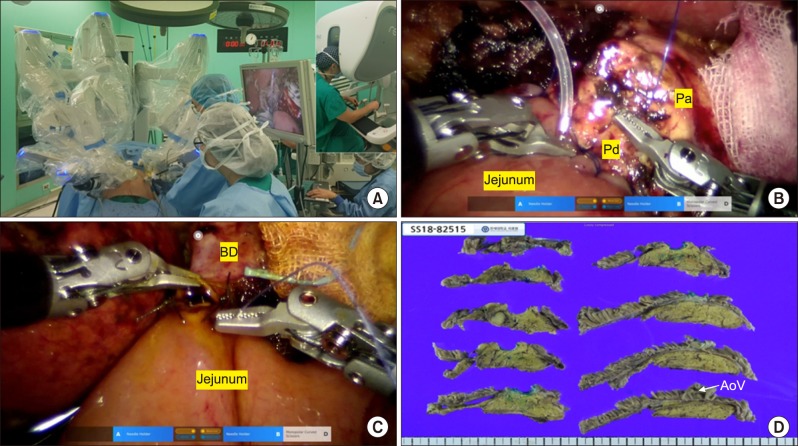
The patient underwent surgery on December 21, 2018. She was placed in a supine position. The surgery consisted of two processes: laparoscopic resection and robotic reconstruction. The laparoscopic resection technique used in our institution had been previously published.20 The total operation time for laparoscopic resection was 3 hours and 30 minutes, and the Revo-i robotic surgical system was docked (Fig. 2A). Revo-i-assisted pancreaticojejunostomy (PJ) with a double-layered duct-to-mucosa anastomosis (4 inner interrupted sutures for pancreatic duct less than 2 mm with a short stent and all interrupted sutures for the outer layer of PJ) (Fig. 2B) and choledochojejunostomy (CJ) (posterior continuous and anterior interrupted sutures using 4-0 absorbable sutures for 8 mm of remnant bile duct reconstruction) were performed (Fig. 2C), which took about 4 hours. The total operation time was noted to be 514 minutes. The estimated blood loss was 200 ml. No intraoperative transfusions were required. After the delivery of the specimen through the small, vertical, extended umbilical wound, duodenojejunostomy was performed manually. Two-armed closed suction drains were inserted around the anastomosis sites.
Postoperative course
The postoperative course was uneventful, except for mild fever. Her surgical drains were removed on postoperative day 5. A follow-up computed tomography (CT) was performed on postoperative day 7. Scant fluid along the PJ site was noted on CT. The patient was discharged 10 days after the operation, without any complications.
Pathological examination
The pathological diagnosis was neuroendocrine tumor (NET), measuring 11 mm in size (Fig. 2D). The mitotic count was 1 per 10 high-power fields, and the Ki-67 labeling index was 3/760 (0.4%). These results indicated Grade 1 NET based on the 2017 World Health Organization classification. No lymphovascular invasions were detected. A total of 6 lymph nodes were harvested, with no lymph node metastases. All the resection margins were negative.
Go to :
DISCUSSION
The robotic surgery system has gained popularity because of various advantages over the laparoscopic surgery. It enables a more delicate and finer procedure. Furthermore, robotic surgeries show decreased postoperative morbidity and hospital stay and faster recovery of patients compared to the open approaches.21 They have now been widely applied in abdominal surgeries. According to the 2016 Intuitive Surgical Annual Report, there are over 3700 robotic surgical systems worldwide and over 3,000,000 robotic surgeries have been performed.22 Robotic pancreaticoduodenectomy is also feasible and safe in select patients.23,24,25 However, the high medical costs of robotic surgery, which have been an impediment to their development and evolution, have been constantly discussed.25,26,27 New robotic surgery systems with lower medical costs are required.
The Meerecompany Inc. has been developing a new robotic surgical system called Revo-i in Korea since 2006. Several preclinical studies have been conducted on robotic surgery using Revo-i in a porcine model.19,28,29,30 Kang et al.19 and Lim et al.30 simultaneously verified the safety and efficacy of robotic cholecystectomy performed using Revo-i in a preclinical experiment. Abdel Raheem et al.29 also showed the feasibility of fallopian tube surgery using Revo-i in a preclinical chronic porcine model. Owing to these results, the Revo-i received approval for clinical use from the KFDA in 2016. In the first clinical trial of Revo-i, Chang et al.18 successfully carried out 17 robotic surgeries on patients with localized prostate cancer, without any serious complications. In addition, Kang et al.19 performed successful Revo-i cholecystectomy in the first human clinical trial. Based on these positive perioperative outcomes in the human clinical trials of Revo-i, it was commercially licensed in August 2017.
In a previous study, the Revo-i characteristics were compared to the da Vinci Surgical System.30 The da Vinci Surgical System differed mainly with regard to energy sources. Currently, Revo-i has only mono-polar and bi-polar energy delivery systems. Therefore, Revo-i can be effectively used in the reconstruction phase of PD, but not in the resection phase, which requires fine dissection and rapid hemostasis. The next generation of Revo-i would be equipped with energy devices, such as vessel sealers and harmonic scalpels.
To the best of our knowledge, this is the first report of PPPD performed using Revo-I, which is an alternative robotic surgical system for the da Vinci Surgical System. In a previous human clinical trial of Revo-i cholecystectomy and prostatectomy, it was found technically feasible and safe in performing delicate and complex surgical procedures, such as PJ in remnant pancreas with a pancreatic duct shorter than 2 mm and CJ in a remnant bile duct smaller than 1 cm. The articulating movement of a robotic instrument and effective third-arm intervention are useful during the reconstruction phase of PD. However, for a safer and more reliable clinical application of Revo-i in advanced minimally invasive surgeries, improving the durability and fine tuning of robotic instruments and quality of vision should be mandatory. An additional clinical trial to investigate the safety of Revo-i in advanced minimally invasive hepatobiliary and pancreatic surgery should be performed.
In summary, we have successfully performed PD using Revo-i to treat a patient with insulinoma of the pancreatic uncinate process. This case demonstrated the technical feasibility of the Korean robotic surgical system Revo-i. We hope that other robotic systems would be developed to overcome the current limitations regarding cost effectiveness and to provide high-quality, minimally invasive surgeries in the near future.
Go to :
 XML Download
XML Download