

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hip arthroscopy has largely replaced open techniques to treat various conditions including femoroacetabular impingement syndrome (FAIS), extra-articular lesions, septic arthritis, loose bodies and others1234). Most patients treated with hip arthroscopy for FAIS–the most common indication for hip arthroscopy-experience improved functional outcomes and a low rate of postoperative complications456789). The cumulative risk of reoperation (revision hip arthroscopy, hip arthroplasty) following an arthroscopic hip procedure was recently reported as 5.5%5). Although residual bony abnormality has been reported as the most common reason for revision hip arthroscopy, other patients require revision as a result of hip instability59).
Iatrogenic instability caused by a non-repaired capsulotomy or capsulectomy is being recognized with increased frequency91011); reports have described hip subluxation or dislocation following arthroscopic procedures11121314). Increased attention has been focused on the role of the hip capsule in post-arthroscopic pain and instability1516). In fact, several biomechanical studies have demonstrated the importance of the hip capsule on hip stability1718192021), with a focus on the function of the iliofemoral ligament (IFL)1922). Wuerz et al.20) revealed that larger-sized capsulotomies resulted in increased joint mobility, while Khair et al.18) demonstrated that sequential distraction with 2, 4, 6, and 8 cm interportal capsulotomies significantly altered IFL strength leading to a reduction in the force required to axially distract the hip. Both studies reported complete reversal of hip instability when capsular anatomy was restored. Clinical studies have corroborated these biomechanical findings, with some studies demonstrating improved clinical outcomes with complete capsular repair compared to capsulotomy or partial repair2324).
Based on the above, the treating hip arthroscopist must balance creating a capsulotomy large enough to adequately visualize and address underlying pathology while not compromising the ultimate integrity of the hip capsule, especially the IFL25262728). Regarding the most preferred capsulotomy techniques, most surgeons take an interportal approach, followed by T-capsulotomy (T-shaped incision of the capsule) and others2930). An interportal capsulotomy between the standard anterolateral portal (ALP) and standard anterior portal (SAP), may be much larger than necessary to complete the tasks required of arthroscopic hip surgery. To reduce the iatrogenic capsular morbidity, the authors prefer an interportal capsulotomy between the ALP and the modified anterior portal (MAP), an approach which still allows for the successful completion of the procedure. No previous study has characterized potential anatomical differences between the aformentioned interportal capsulotomy techniques, including the extent of IFL damage.
The purpose of this study was to identify and characterize potential differences in capsulotomy size and cross-sectional area (CSA) of interportal capsulotomies made with the SAP compared to the MAP. We hypothesized that the MAP will yield a significantly smaller interportal capsulotomy size and CSA compared to the SAP, thus resulting in less damage to the IFL.
Go to : 
MATERIALS AND METHODS
This was a cadaveric study without specimen identification, therefore approval by the Institutional Review Board was not required. Ten fresh-frozen cadaveric hip specimens consisting of the ipsilateral hemi pelvis and femur were used. Each cadaveric specimen was placed supine on a surgical table and mounted to simulate hip arthroscopic positioning. Axial traction was applied to achieve 1 cm of distraction across the femoroacetabular joint, simulating intraoperative traction necessary to access the central compartment.
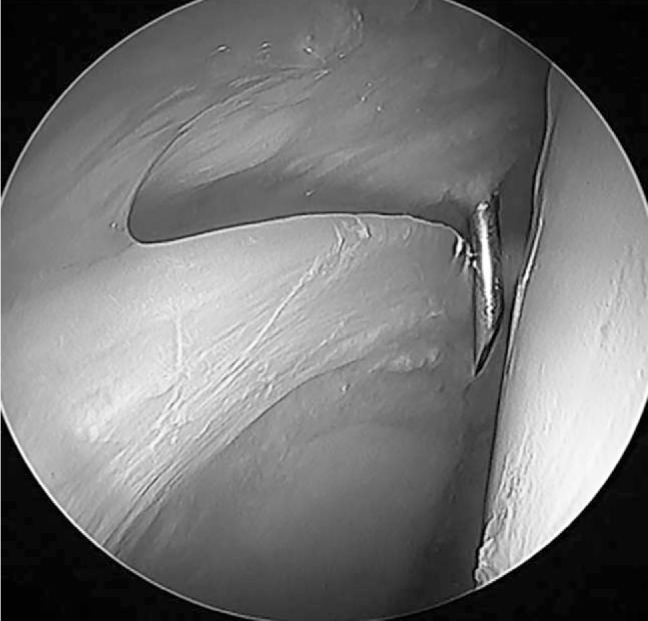
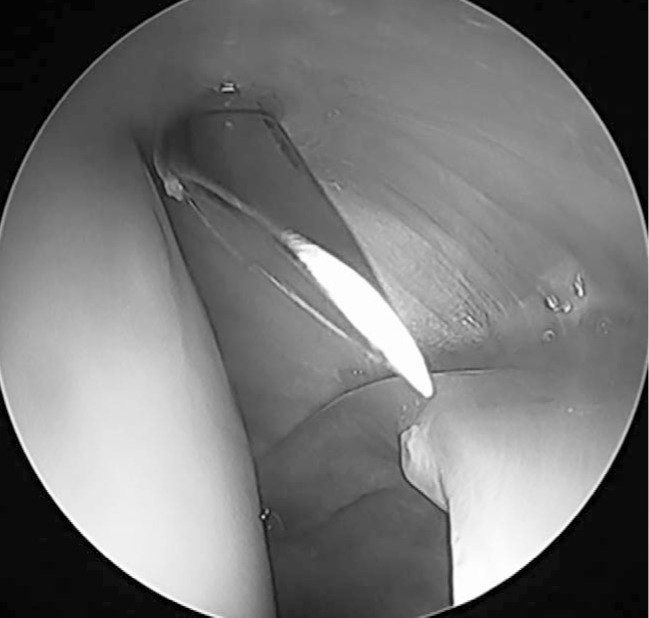
A standard ALP was created 1 cm anterior and 1 cm proximal to the anterolateral tip of the greater trochanter, and the arthroscope was inserted into the hip joint central compartment. Hips were then randomized to the SAP group (n=5) or MAP group (n=5) (Fig. 1). Under direct arthroscopic visualization, a spinal needle was used to localize the SAP or MAP position. For the SAP, the superficial landmark was palpated at the intersection between a horizontal line from the tip of the greater trochanter and a vertical line from the anterior superior iliac spine (ASIS), followed by placement of the spinal needle at the center of the anterior triangle (Fig. 2). The superficial landmark for the MAP was palpated 1 cm distal and 1 cm lateral from the intersection between a horizontal line from the tip of the greater trochanter and a vertical line from the ASIS. The deep MAP landmark was located 1 cm anterior to the tip of ALP. Specifically, the spinal needle was introduced into the central compartment such that the tip could touch the arthroscopic camera cannula (Fig. 3). A nitinol wire was then introduced through the spinal needle and a cannula was placed over the nitinol wire. The interportal capsulotomy was then completed between the established portals in all hips with the Samurai blade (Stryker Sports Medicine, Greenwood Village, CO, USA).
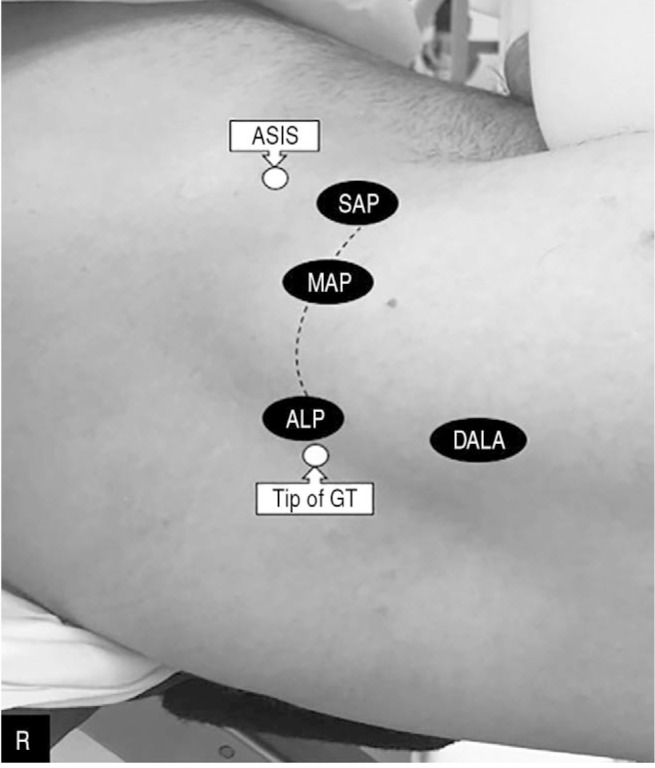 | Fig. 1Demonstration of the superficial landmarks and common arthroscopic portals used to correct femoroacetabular impingement lesions on a right (R) hip: anterolateral portal (ALP), mid-anterior portal (MAP), and standard anterior portal (SAP), distal anterolateral portal (DALA), greater trochanter (GT), anterior superior iliac spine (ASIS). The line demonstrates the connection between ALP-MAP versus ALP-SAP which is performed during the interportal capsulotomy.
|
Once the capsulotomy was completed, the arthroscopic equipment was removed from the hip joint and a Smith–Petersen open approach to the hip joint was performed to the level of the IFL. The length and width of each capsulotomy was measured using digital calipers (Fig. 4). The dimensions of the IFL were also recorded allowing for the length of the capsulotomy to be expressed as a percentage of total IFL side-to-side width (Fig. 5). To calculate CSA, a standardized 1 cm marker was placed immediately adjacent to the capsulotomy and a high-resolution digital photograph was taken at a standardized distance and angle. The area of hip joint exposure for each capsulotomy was determined by measuring joint CSA with ImageJ software (National Institutes of Health, Bethesda, MD, USA). Each pixel was assigned a unit length in centimeters according to the 1 cm calibration marker. The exposed central compartment was then outlined with the ImageJ tracing tool and CSA was calculated in triplicate; the average of the three measurements was used for data analysis.
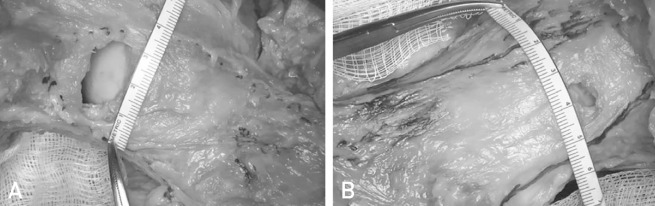
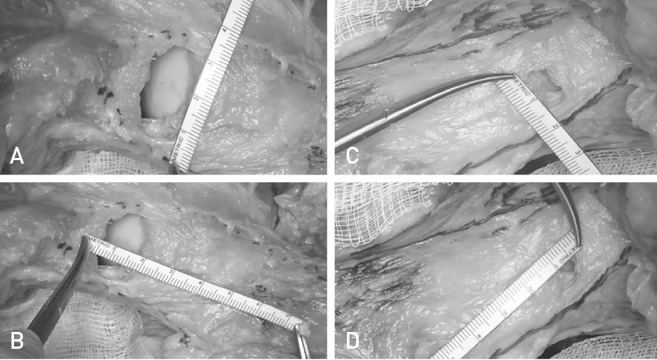 | Fig. 4(A) Measurement of the standard anterior portal (SAP) interportal capsulotomy length. (B) Measurement of the SAP interportal capsulotomy width. (C) Measurement of the modified anterior portal (MAP) interportal capsulotomy length. (D) Measurement of the MAP interportal capsulotomy width.
|
 | Fig. 5(A) Measurement of the iliofemoral ligament (IFL) side-to-side width at the level of the capsulotomy allowing for the width of the standard anterior portal interportal capsulotomy to be expressed as a percentage of total IFL. (B) Measurement of the IFL side-to-side width at the level of the capsulotomy allowing for the width of the modified anterior portal interportal capsulotomy to be expressed as a percentage of total IFL.
|
Statistical analysis was performed using IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA). Data were assessed for normality and statistical comparisons between the SAP and MAP groups were made using a Student's t-test or its nonparametric equivalent. A P<0.05 was considered significant.
Go to :
RESULTS
Cadaveric specimens (5 right and 5 left hemi pelvises) included 1 female and 9 male donors with a mean age of 73.60±3.50 years and a mean weight of 64.6 kg±11.8 kg. There was no significant difference in age or weight between the SAP and MAP groups (SAP 73.4±2.6 years vs. MAP 73.8±4.6 years [P=0.69] and SAP 67.13 ±15.8 kg vs. MAP 62.14±6.35 kg [P=0.53]). There were no differences between SAP and MAP groups with respect to: (i) IFL width at the level of the capsulotomy (SAP 3.71±0.61 cm vs. MAP 3.74±0.19 cm, P=0.92) or (ii) maximum IFL width (SAP 5.22±0.71 cm vs. MAP 4.97±0.30 cm, P=0.54).
Capsulotomy dimensions of each group are presented in Table 1. The capsulotomy length was significantly longer in the SAP group compared with the MAP group (SAP 2.69±0.26 cm vs. MAP 1.21±0.10 cm, P=0.008). When standardized by IFL width, the SAP group had a significantly longer capsulotomy expressed as a percentage of total IFL width when compared with the MAP group (SAP 74.2±14.1% vs. MAP 32.4±3.74%, P=0.008). In addition, the capsulotomy was significantly wider and had a significantly larger CSA in the SAP group when compared with the MAP group (length: SAP 1.51±0.34 cm vs. MAP 0.82±0.069 cm, P=0.002; CSA: SAP 2.16±0.64 cm2 vs. MAP 0.65±0.17 cm2, P=0.008). The plotting distribution of the above measurements are presented for both groups in Fig. 6.

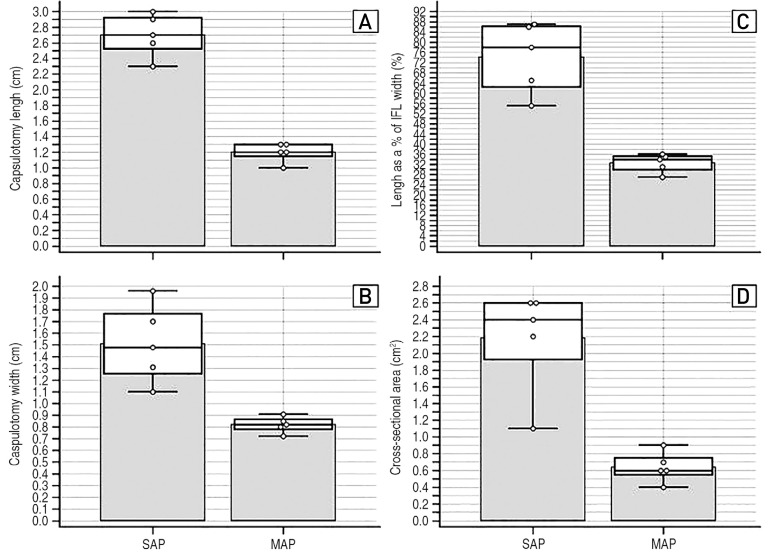 | Fig. 6Plotting distribution of the measurements in the modified anterior portal (MAP) versus standard anterior portal (SAP) groups: (A) Capsulotomy length. (B) Capsulotomy width. (C) Length of capsulotomy as a percentage of iliofemoral ligament (IFL) width. (D) Cross-sectional area of the anterolateral portal (ALP)-SAP and ALP-MAP capsulotomy.
|
Table 1
Capsulotomy Dimensions between Groups
![]()
Go to :
DISCUSSION
The present cadaveric study demonstrates that an interportal capsulotomy created between the ALP and the MAP resulted in significantly less damage (lower percentage) of the total IFL width compared with those created between the ALP and the SAP. In addition, the use of the MAP resulted in an interportal capsulotomy with a significantly smaller CSA compared with the corresponding interportal capsulotomy created with the SAP.
The IFL is critical for the stability of the hip joint and previous studies have demonstrated that this structure is at greatest risk of damage when performing interportal hip capsulotomy. Khair et al.18) demonstrated that sequential distraction with 2, 4, 6, and 8 cm interportal capsulotomies significantly altered IFL strength resulting in less force required to axially distract the hip; however, suture repair was capable of restoring capsular strength to that of an unaltered hip. Myers et al.19) demonstrated that the IFL was a primary stabilizer in both anterior translation and external rotation, while the labrum served as a secondary stabilizer. Bayne et al.22) demonstrated in 13 cadaveric hips that an interportal capsulotomy through the IFL resulted in increased posterior and anterior translation with the hip in a flexed or neutral position, respectively. Our study confirms that the anatomical landmarks of both ALP-SAP and ALP-MAP fall within the borders of the IFL, which constitutes the thickest portion of the hip capsule. One can recognize the IFL originating from the acetabular rim at the 2 o'clock position, as previously described by Philippon et al.31).
This current study demonstrates that an ALP-MAP capsulotomy results in significantly less IFL structural damage compared to an ALP-SAP capsulotomy. We previously mentioned that extensive research has been performed demonstrating the biomechanical effect of interportal capsulotomy on the hip capsule and the stability of the joint10172527283233). In addition, previous cadaveric studies have proven the effectiveness of partial or complete repair of the capsulotomy in restoring hip stabilization17181920263334). Our study did not analyze the biomechanical influence of ALP-SAP or ALP-MAP on hip stability, nor explored whether repairing the interportal capsulotomy would be sufficient to achieve hip stabilization. Our study constitutes an anatomical demonstration of two separate interportal capsulotomy techniques, by comparing the size of native tissue damage, which was also expressed as percentage of total IFL width damage (SAP 5.22±0.71 cm vs. MAP 4.97±0.30 cm, P=0.54). Based on our findings, surgeons might attempt to modify their surgical technique in order to minimize the iatrogenic IFL damage, while accomplishing adequate hip visualization and successfully addressing the existing structural abnormalities. By increasing the ratio of intact capsular tissue to repaired/unrepaired capsular tissue, the likelihood of post-operative hip instability might decrease.
Another advantage of performing a smaller sized interportal capsulotomy is the ability to repair it more efficiently compared to a larger capsulotomy, while also minimizing the capsular defect post-operatively in cases where capsular repair is contraindicated. The rationale behind repairing the capsule is to restore the native hip anatomy, which might positively affect the clinical outcomes following an arthroscopic procedure of the hip. Domb et al.3536) initially found no difference in clinical outcomes at a 2-year follow-up in patients receiving a capsular repair versus those without capsular repair, however, patients with unrepaired capsules had a higher rate of subsequent total hip arthroplasty and lower modified Harris hip score at a minimum follow-up of 5 years. Similarly, Bolia et al.23) reported that patients who did not undergo capsular repair during hip arthroscopy for FAI, were 6.8 times more likely to convert to total hip replacement compared to a matched group of patients with repaired capsulotomy, at minimum follow-up of 6.4 years. Chambers et al.30) have reported successful clinical outcomes in a group of patients who underwent periportal capsulotomy, which was performed by only dilating the ALP and MAP, without completing a full interportal capsulotomy. Overall, accumulating clinical evidence tends to support the preservation of the native capsular tissue, which further reinforces the validity of the current study.
We did not examine possible differences in visualization between the MAP and the SAP capsulotomy during hip arthroscopy. It has been reported that reducing the length of the hip capsulotomy to minimize the iatrogenic injury on the native capsular tissue, might lead to suboptimal hip visualization during the procedure2334). Cvetanovich et al.37) revealed that T-capsulotomy provides better visualization during hip arthroscopy compared to an extended interportal capsulotomy. Since residual FAI has been reported as the most common indication for revision hip arthroscopy, surgeons should ensure that adequate visualization is achieved to avoid under-correction of FAI, while attempting to preserve the anatomic integrity of the IFL to prevent iatrogenic hip instability3839). Our study compared the anatomical characteristics of two different types of interportal capsulotomy, but we did not examine the corresponding anatomy of the T-capsulotomy. According to a systematic review, interportal capsulotomy is the predominant type of capsulotomy used by surgeons and post-operative hip instability is rare, especially when the capsulotomy is repaired upon the completion of hip arthroscopy29).
The results of this study must be interpreted within the context of its limitations. First, the capsulotomy results were not correlated with anatomic variability in the cadaveric specimens which may impact IFL size or structure (e.g., presence of dysplasia or osteoarthritis). In addition, the average age of the cadaveric specimens was 74 years old and 90% were male, thereby limiting the ability to generalize these findings to younger females. With regards to CSA measurements, visualization of the hip joint was conducted using a camera from a reproducible angle and distance with a radiographic marker to standardize measurements; however, the results of this approach are two-dimensional representations of visualization afforded by capsulotomy, a limitation since it does not account for three-dimensional femoral head-neck junction morphology. As mentioned above, an objective comparison of the ease of visualization of the central and peripheral compartments between the MAP and SAP capsulotomies was not attempted. Lastly, the external validity of our measurements might have been limited by the use cadaveric specimens. Future research should focus on developing methods to evaluate the anatomical characteristics of the hip capsulotomy during hip arthroscopy on living patients to allow for “customized” capsulotomies to be performed based on unique anatomy and structural abnormalities of each patient.
Go to :
CONCLUSION
The CSA of the interportal capsulotomy is significantly smaller when created between the ALP and MAP when compared with those created between the ALP and SAP. The percentage of total IFL violated is significantly smaller when the MAP is used compared to the SAP. Surgeons should be aware of how much of the IFL is incised while performing an interportal capsulotomy; this will help minimize damage to the native capsule and likely decrease the risk of post-operative hip instability.
Go to :
 XML Download
XML Download