

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Femoroacetabular impingement (FAI) as a cause of early osteoarthritis was proposed by Ganz et al.1) in 2003, and treatment with arthroscopy has been shown to be a reasonable, safe, and successful option for management when non-operative management proves unacceptable23). However, hip arthroscopy for FAI and related conditions, is a technically challenging procedure with a steep learning curve requiring career volumes greater than 519 procedures to significantly reduce the risk of reoperation45). In spite of these challenges, the incidence and complexity of arthroscopic procedures involving the hip joint performed in the USA has increased significantly over the past decade, with an increase in procedure incidence reported to be as high as 365% between 2004 and 2009678). As a result of expansion of the indications for and growing expertise in hip arthroscopy, the number of FAI-related arthroscopies has further increased as much as 55% between 2011 and 201489). As such, one can expect a proportional increase in the number of patients who may face sequelae attributable to arthroscopic FAI repair. Therefore, identification of the potential long-term impact of this procedure, particularly on subsequent surgical interventions, including total hip arthroplasty (THA) specifically is imperative.
An estimated 2.5 million Americans live with prosthetic hip joints, and in 2010, over 300,000 THA procedures were conducted in patients 45 years of age or older–more than double that of the year 20001011). The incidence of THA procedures is expected to rise, most significantly in younger, more active patients (age<65 years)12), which creates the need for evidence-based research to identify factors that increase morbidity associated with the procedure. The findings of such studies will assist physicians in making more astute clinical decisions and thus reduce the burden of complications and reoperations for an increasingly large swath of orthopaedic patients.
FAI procedures are done to prevent or delay the development of hip osteoarthritis, however, it is not uncommon to see patients fail FAI repair procedures and later develop endstage osteoarthritis of the hip requiring THA. Evidence exists to support the risk of negative implications of arthroscopy on subsequent joint replacement in the knee1314). Prior studies evaluating FAI repair procedures as a risk factor for complications after THA were mostly smaller, institutional reviews that were inadequately powered to evaluate risk factors for various outcomes1516171819).
The purpose of the present study was to evaluate whether prior arthroscopically corrected FAI impacts postoperative complication rates in patients receiving subsequent ipsilateral THA, and to examine comorbidities that may affect THA outcomes on a national scale. The authors hypothesize that patients who had arthroscopic repair of FAI prior to THA should not have significantly different outcomes than patients who had no prior interventions.
Go to : 
MATERIALS AND METHODS
1. Database
A commercially available, national insurance-based database – PearlDiver Patients Records Database (www.pearldiverinc.com; PearlDiver Inc., Colorado Springs, CO, USA) – which contains patient records from both private insurers and Medicare was used. The data queried were de-identified and compliant with the privacy rules of the Health Information Portability and Accountability Act, forgoing the need for Institutional Review Board approval. The subset of patients in the database covered by Humana Inc. (Louisville, KY, USA) had data on laterality of their procedures available which was necessary given the nature of the study performed, and as such, these patients were the subject of our inquiry. Patient records (e.g., demographics, comorbidities, procedures, complications – 90-day readmission, aseptic dislocation/revision within 3 years, surgical site infection [SSI] within 3 years, and hip stiffness within 3 years) were catalogued by International Classification of Diseases (ICD) codes and Current Procedural Terminology (CPT) codes and obtained from the database.
2. Study Cohorts
A retrospective review of patients who underwent primary THA (CPT-27130) from 2005 to 2014 was performed. As presented in Table 1, this initial group of patients was further queried to identify patients with a history of arthroscopic FAI repair (CPT-29860, 29861, 29862, 29863, 29914, 29915, 29916). To ensure laterality was the same in the subset of patients who had both procedures, arthroscopic FAI repair and subsequent THA were queried separately according to the side of each procedure. Any patient with a history of prior malignant neoplasm involving the hip, pathological hip fracture, acetabular fracture, or femoral neck fracture based on CPT or ICD codes were excluded from our study. Our control group (or native hip group) consisted of 10,951 patients who did not have arthroscopic repair of FAI prior to THA and our study group (or post arthroscopy group) included the remaining 110 who had arthroscopic repair of FAI prior to ipsilateral THA. The two groups were proportionally matched (1:100) for age, sex, body mass index, and several other demographic and comorbid factors; these patient characteristics were compiled and compared as presented in Table 2.
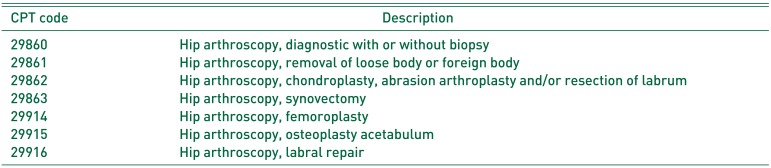
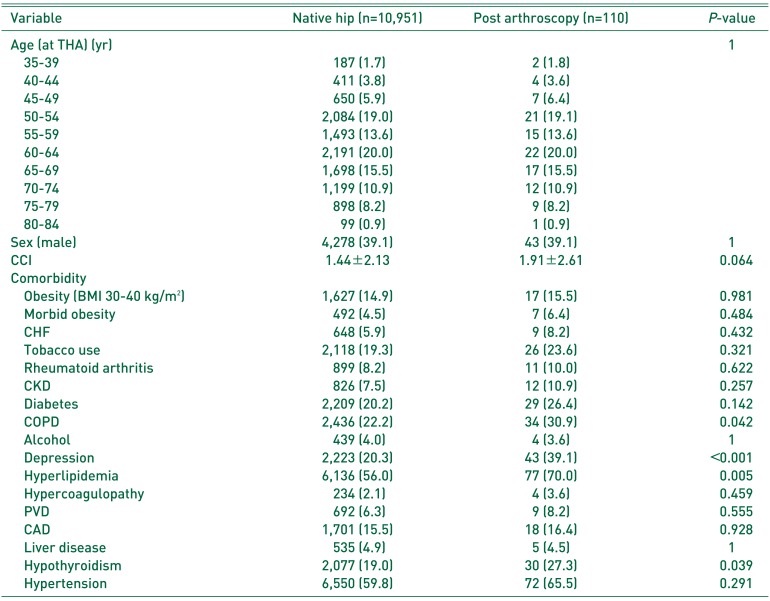
Table 1
CPT Codes Queried for Hip Arthroscopy
![]()
Table 2
Patient Demographics
Values are presented as number (%) or mean±standard deviation.
THA: total hip arthroplasty, CCI: Charlson comorbidity index, BMI: body mass index, CHF: congestive heart failure, CKD: chronic kidney disease, COPD: chronic obstructive pulmonary disease, PVD: peripheral vascular disease, CAD: coronary artery disease.
![]()
3. Risk for Complications after Total Hip Arthroplasty
Postoperative complications (i.e., 90-day readmission, aseptic dislocation/revision within 3 years, SSI within 3 years, and hip stiffness within 3 years) were examined for any potential independent association with either of our two study groups. The total number of each complication and the rates of each complication were calculated for both groups, and P-values were determined to assess significance. The comorbidities faced by both groups were assessed for independent association with the previously stated postoperative complications.
4. Statistical Analysis
R Project for Statistical Computing software (https://www.r-project.org/), available through the PearlDiver database was used for all statistical analyses. The demographics and comorbidities of each group were compared using Pearson's chi-squared analysis and Welch's t-test. The former was used to test for significant differences in categorical data (i.e., age groups, sex, prior comorbid medical diagnoses). The latter was used to test for differences in 10-year survival between the groups as measured by the Charlson comorbidity index score. A P-value was calculated for each comparison.
A multivariate logistic regression analysis was used to assess for any independent effect of various comorbidities on the aforementioned complications. Odds ratios (OR) were calculated from the regression analysis, and a corresponding 95% confidence interval (CI) and P-value was also calculated for each comorbidity. For all statistical calculations, P<0.05 was considered statistically significant.
Go to :
RESULTS
1. Patient Comorbidities
A total of 11,061 patients met our inclusion criteria. 10,951 of them had a THA without prior FAI repairs and 110 had both procedures performed ipsilaterally. There was no significant difference between groups for any of the demographics analyzed. A comparison of prior comorbidities revealed that chronic obstructive pulmonary disease (22.2% vs. 30.9%, P=0.042), depression (20.3% vs. 39.1%, P<0.001), hyperlipidemia (56.0% vs. 70.0%, P=0.005), and hypothyroidism (19.0% vs. 27.3%, P=0.039) were significantly more prevalent in our post arthroscopy group compared to the native hip group.
2. Arthroscopic Femoroacetabular Impingement Repair as a Risk Factor for Postoperative Complications
Patients in the post arthroscopy group did not have significantly higher rates of 90-day readmission (P=0.585), aseptic dislocation/revision within 3 years (P=0.409), SSI within 3 years (P=0.796), or hip stiffness within 3 years (P=0.977) following THA when compared to the native hip group (Table 3).

3. Comorbidities That Affect Outcomes Following Total Hip Arthroplasty
There were several comorbidities that showed significantly increased risk for complications after THA (Table 4). Of the patients who suffered aseptic dislocation/revision, the most significant association was with pre-existing depression (OR=2.42, P<0.001). Morbid obesity (OR=2.16, P<0.001) was the most significant risk factor associated with SSI within 3 years of THA. The most significant risk factors for 90-day readmission were congestive heart failure (OR=1.57, P<0.001) and depression (OR=1.57, P<0.001). Finally, male sex (OR=1.41 P=0.011) was most significantly associated with stiffness within 3 years.
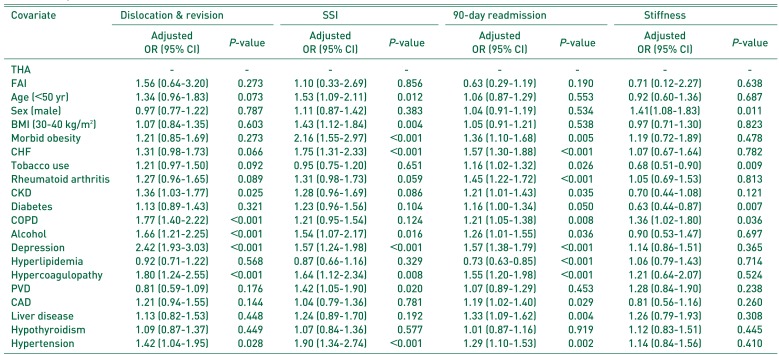
Table 4
Analysis of Comorbid Conditions for all THA
THA: total hip arthroplasty, SSI: surgical site infection, OR: odds ratio, CI: confidence interval, FAI: femoroacetabular impingement, BMI: body mass index, CHF: congestive heart failure, CKD: chronic kidney disease, COPD: chronic obstructive pulmonary disease, PVD: peripheral vascular disease, CAD: coronary artery disease.
![]()
Go to :
DISCUSSION
The present study is among the first to evaluate whether arthroscopic repair of FAI pathology impacts the outcomes of subsequent THA on a national scale in the USA. This study has added to the current body of literature surrounding hip arthroscopy and THA by providing data on long-term hip stiffness, and 3-month readmission rates – two very clinically relevant outcomes to the studied population. In this proportionally matched study, no significant difference was observed in the rates of 90-day readmission, aseptic dislocation/revision within 3 years, SSI within 3 years, or hip stiffness within 3 years between our study and control groups.
Early surgical intervention in the management of FAI was first discussed by Ganz et al.1) in their 2003 study; since then, arthroscopic management of the condition has been described as just as effective, and certainly less invasive than open approaches23202122). Despite advantages of the more minimal approach, the field of hip arthroscopy has been developed relatively recently, the procedure is technically challenging, and high volumes of the procedure are required to reduce complication rates420232425). Most complications associated with hip arthroscopy described to date are minor or transient26), and Kowalczuk et al.27) in their systematic review and meta-analysis of 6962 cases calculated a complication rate of 4.0% (95% CI=2.9–5.2%) for such minor, nonlimb threatening complications. As with many surgical procedures though, major complications do also exist for hip arthroscopy. These major complications have been calculated by Kowalczuk et al.27) to occur at a rate of 0.3% and are discussed by Nakano and Khanduja26).
The literature describing late complications of hip arthroscopy, in particular, the effect on outcomes of future surgical interventions is limited to relatively small study groups151617181928). As the incidences of both arthroscopic FAI repair and THA have been increasing678910) and are only expected to continue to rise12), the need for research to better guide management and counseling of this expanding subset of patients is clear.
Considering strictly morphology, successful arthroscopic FAI repair should not make a subsequent THA more technically challenging, or more prone to complications26). However, in light of the theory that hip arthroscopy may traumatize the native joint leading to scarring and persistent inflammation19), the idea that the procedure may bear some negative effect on a future THA is certainly within the realm of possibility. Furthermore, complications like adhesions and heterotopic ossification are known to occur and the latter has become increasingly common as more arthroscopic FAI repair techniques are described2629). Capsular laxity due to inappropriate management of the hip capsule during arthroscopy has been implicated in compromised stability and kinematics of the joint30). These complications may cause deformity of the native joint which has been shown to be significantly associated with complications after THA31). Finally, given evidence that arthroscopy is related to higher rates of postoperative complications and failures following subsequent joint arthroplasty in the knee1314), it is reasonable to imagine that a similar relationship may exist in the hip, especially considering that arthroscopy in the hip is much more challenging and far less familiar to surgeons.
Recently, Charles et al.15) examined 39 patients who underwent THA after hip arthroscopy for FAI and found no differences between a matched control group in: (i) estimated blood loss, (ii) operative time, (iii) early postoperative physical therapy metrics, (iv) early inpatient narcotics requirements, (v) length of hospital stay, (vi) heterotopic bone formation, (vii) rates of emergency department evaluations, or (viii) superficial and deep periprosthetic infections. Parker et al.32), in their study of 35 patients found no difference in range of motion, complication rate, implant survival, or functional outcomes between naïve hips receiving THA and those previously treated with arthroscopy. The current study corroborates the claims made for dislocation/revision rates, infection rates, and stiffness. These findings were expanded upon through demonstration of no difference in 90-day readmission between groups. Our study found that depression was significantly associated with both aseptic dislocation/revision, and 90-day readmission and that hyperlipidemia had a significant negative association with 90-day readmission. In spite of the fact that both depression and hyperlipidemia were significantly more common in the FAI Group, they did not appear to impact the rates of complications between the groups.
Perets et al.17) have one of the only studies to date that claims a negative relationship between hip arthroscopy and subsequent THA. They found that THA patients with a history of ipsilateral hip arthroscopy had worse patient reported outcome measures (e.g., Harris hip score, Forgotten joint score, satisfaction) than those with no prior surgery. However, it is important to note that their study did not identify any significant differences in rates of complications or visual analogue scale (pain scores) which indeed corroborates the findings presented here.
Limitations exist in our analysis and design. Only patients that were covered by Humana Inc. in our database had data available on the laterality of their procedure. This drastically reduced our potential sample size, power of the study, and of course means our findings may not be truly representative of the USA patient population. Further, given this was a database study, the strength of our findings is hinged to the coding, miscoding, and even non-coding done by physicians, which introduces some inherent error. One of our outcome measures, hip stiffness, depended on the presence of an ICD code (M2.65-) in a patient's chart. The use of the code (i.e., what different physicians deemed hip stiffness, and the degree of stiffness) would certainly vary based on a number of factors for which we could not control. Finally, we did not examine patient reported outcomes which may have added valuable information to the analysis.
Time between arthroscopy and THA as an aggravating factor for complications should be examined. The limitations imposed by our database to protect the privacy of our patients rendered an analysis of clinically relevant intervals of time impossible due to the limited sample size. Furthermore, our sample size also precludes us from performing a subgroup analysis of the risks associated with various types of hip arthroscopy (e.g., labral repair, femoroplasty). As more patients undergo both procedures, future studies should strive to examine the effect of time, and perform subgroup analyses to clarify the narrative set forth by the present study.
Go to :
CONCLUSION
The findings of this study support that arthroscopic repair of FAI pathology is not an independent risk factor for complications following subsequent, ipsilateral THA. Physicians should be confident when counselling patients on the long-term effects of arthroscopic repair of FAI that the intervention should not bear any negative effect on postoperative outcomes if a future THA procedure is required.
Go to :
 XML Download
XML Download