

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In the context of increased life expectancy, the number of patients in older age groups aiming to live an active life has been on the rise, despite their higher risk of developing osteoarthritis and hip osteoarthritis specifically1). Recently, due to quicker postoperative recovery, and pain reduction compared to open surgical procedures2), hip arthroscopy is gaining popularity as a hip-preserving surgical approach for those presenting with hip joint lesions345).
Hip arthroscopy in young patients has been proven as an effective treatment option678), while its effects in relatively older patients are controversial91011). Sing et al.2) reported that of all patients, those aged between 40 and 49 years undergoing hip arthroscopy accounted for the highest proportion (over 28% of cases) and those older than 60 years constituted more than 5%. Recent reports have shown promising outcomes with appropriate selection of middle-to-older-aged patients121314).
However, clinical outcomes after hip arthroscopy in middle-aged patients with early osteoarthritis rather than with specific diagnoses (e.g., femoroacetabular impingement [FAI], labral tears) are rarely reported1516). Therefore, the authors analyzed patients undergoing hip arthroscopic surgery among symptomatic patients aged 40 years or older with hip osteoarthritis. This retrospective observational study was designed to assess clinical and radiological outcomes after hip arthroscopy in middle-aged patients with early hip osteoarthritis with varying etiologies.
Go to : 
MATERIALS AND METHODS
The design of this study and protocol were approved by the Institutional Review Board at the Chungnam National University Hospital, and the requirement for informed consent was waived (IRB No. CNUH 2019-03-114).
Between January 2010 and December 2015, 250 patients who were older than 40 years and diagnosed with hip osteoarthritis underwent hip arthroscopic treatments and were possible enrollees for this study. Arthroscopic surgical indications required that patients had symptoms which persisted or deteriorated after preservation treatment (i.e., decreasing activity, medication, physical therapy, weight loss) and progressed after the occurrence of an obvious symptom. Upon physical examination, the combined hip range of motion (ROM) and levels of pain were measured using provocation tests, and the maximum value of joint motion was measured using a goniometer. Of the 250 possible subjects, 61 patients were excluded for one of the following reasons: (1) psychiatric medical history, (2) secondary gain, (3) a medical history of receiving hip arthroscopy on the same side, (4) a Tönnis score of greater than grade II, (5) non adherence to outpatient visits for at least three years, or (6) did not respond to the survey. The authors assumed that patients with secondary gain who were injured at work or injured in an accident and postponed the return to work or daily living. The remaining 189 patients were included in this study (118 male and 71 female; mean of 70.3 months [range: 36 to 107 months] follow-up). The mean age of the patients at the time of the index surgery was 48.0 years (range: 40–67 years). The mean body mass index was 23.7 kg/m2 (range: 18.1 to 31.6 kg/m2). Patients with early osteoarthritis of various diagnoses underwent hip arthroscopy (Table 1).
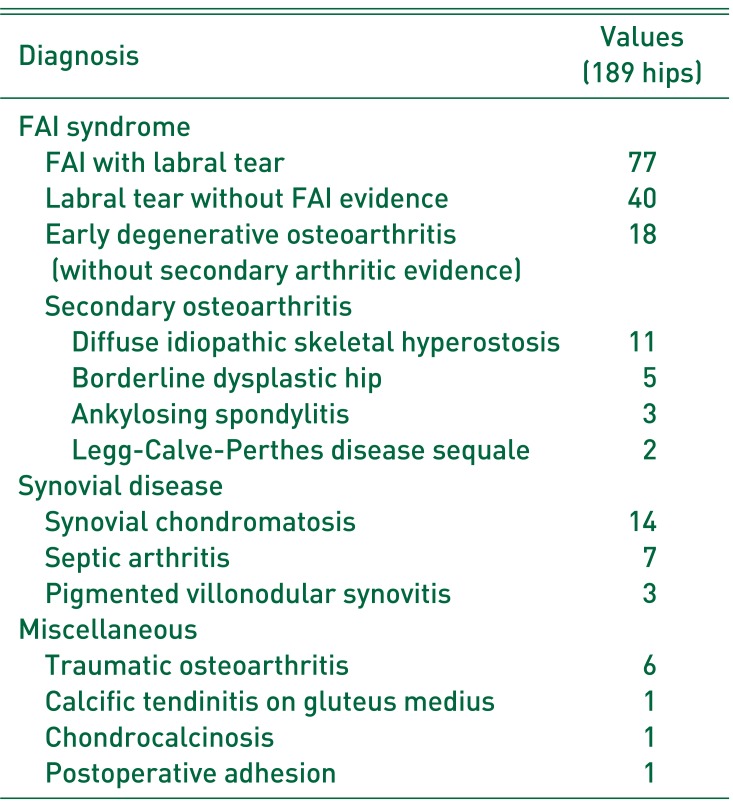
Table 1
Categorization of Patients Who Received Arthroscopic Surgery by Diagnosis
![]()
Arthroscopic surgeries in our study were performed in the typical manner by a highly skilled arthroscopic surgeon according to diagnosis or arthroscopic findings. Osteoplasty was performed to patients with FAI, and labral repair was performed in case of labral tear (Fig. 1). Patients with diffuse idiopathic skeletal hyperostosis or ankylosing spondylitis underwent femoroplasty and/or acetabuloplasty, and labral repair was considered as first treatment of choice when it was possible. Only four patients underwent labral debridement instead of labral repair in this study. Early osteoarthritis of various diagnoses, which is not typical FAI, was also treated with femoroplasty if there was a subchondral sclerosis or there was a possibility of impingement when the hip was flexed during surgery. In cases of cartilage damage, chondroplasty was performed on the acetabulum and/or femoral head. Thorough debridement, mass excision, and lavage were performed for synovial disease. Surgical failure was defined as a case that underwent revision arthroscopy or that required conversion to total hip arthroplasty (THA).
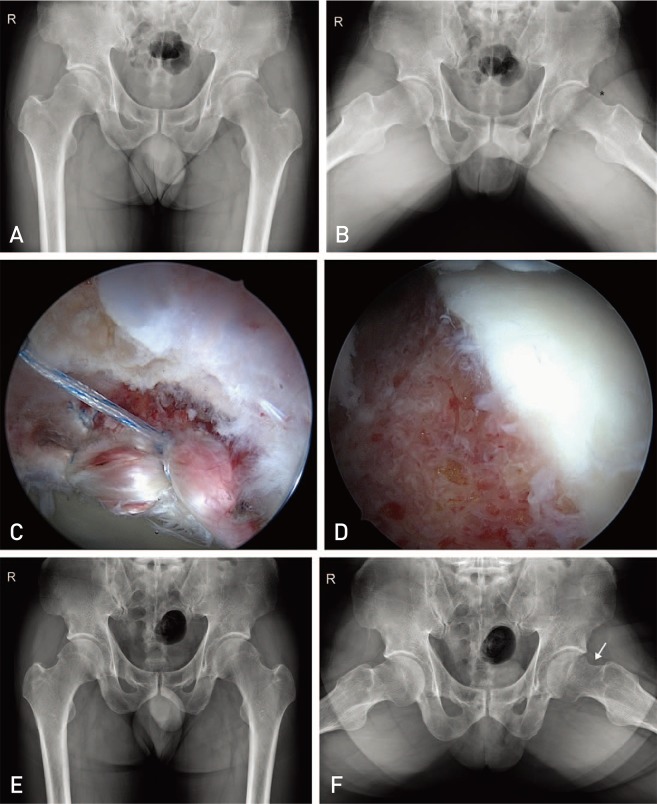 | Fig. 1A 49-year-old male had a left hip femoroacetabular impingement with acetabular labral tear. He underwent arthroscopic labral repair using two anchors and arthroscopic osteoplasty. (A, B) Preoperative anteroposterior and frog-leg simple radiography. A Tönnis grade I osteoarthritis and decreased offset (asterisk) was observed. (C) Two anchors were used for labral repair. (D) Arthroscopic osteoplasty was performed to an existing femoral neck bump. (E, F) The last 50-month follow-up radiography. A Tönnis grade did not change (grade I), and sufficient osteoplasty was observed (arrow).
|
Patient diagnoses were categorized with symptoms, signs, and imaging findings that meet the Warwick Agreement into the FAI syndrome patient group17). Those suffering from disorders of the synovium were classified into the synovial group, whereas those with other diagnoses formed the other group (Table 1). Early degenerative osteoarthritis diagnosis was performed if either typical FAI or other secondary osteoarthritis forms were excluded18). The severity of osteoarthritis was categorized using the Tönnis classification.
1. Clinical Outcome Measure
Modified Harris hip score (mHHS), hip outcome score-activities of daily living (HOS-ADL), visual analogue scale (VAS) for pain, and VAS satisfaction were evaluated for all patients. With no single patient-reported outcome questionnaire available for patients undergoing hip arthroscopy, various outcome measurements were conducted at different points of time19). This survey was conducted prior to surgery, as well as six months, one year, and every year after surgery during outpatient visits. Scores were measured before surgery and at the midterm last follow-up for each patient, and collected data were then analyzed and presented in the form of statistics. The VAS satisfaction score reflects the outcome of the midterm last follow-up.
The patients' hip ROM was also measured, and only the internal rotation and flexion important to the anterior impingement test were used20). Internal rotation was measured while the hip was flexed at 90 degrees. Hip ROM was measured prior to surgery, as well as at six months, one year, and every year after surgery during outpatient visits. Angles before surgery, at one year of surgery, and at the midterm follow-up were measured for each patient and used for statistical analyses. To determine the effects of osteoplasty on ROM changes, patients diagnosed with FAI, diffuse idiopathic skeletal hyperostosis, or ankylosing spondylitis were categorized into Group 1 and the others as Group 2. Then, hip ROM of patients in Group 1 was compared with that of patients in Group 2.
2. Radiological Measure
Before surgery, simple radiography was used to obtain images in the pelvic anteroposterior view, false-profile view, frog-leg side view, and cross-table view. Threedimensional computed tomography (CT) and magnetic resonance imaging (MRI) were performed to identify lesions and aid in differential diagnosis. Simple radiographs were taken preoperatively, as well as at six months, one year, and every year after surgery during outpatient visits. CT and MRI were also performed postoperatively if needed. Osteoarthritis of the hip joint was graded by the Tönnis classification through the findings of joint space narrowing, osteophytes, and bone contour or sclerosis in the pelvic anteroposterior view in the radiograph taken before and after surgery. Tönnis grade 0 are difficult to differentiate with or without arthritis. The authors therefore regarded patients with Tönnis grade 0 as having early osteoarthritis along with patients with Tönnis grade I. Tönnis grade II or more are classified as having advanced osteoarthritis21). Patients with Tönnis grade II or more were excluded. All radiographic films were independently interpreted by two specialists: a hip orthopedist participating in none of the surgeries and a musculoskeletal radiologist. They had to make final judgements and reach a consensus about cases with different interpretations, if any. Diagnosis of borderline dysplasia was considered in cases with lateral center-edge angle values between 20 and 25 degrees.
3. Statistical Analysis
Statistical analyses were performed using IBM SPSS software ver. 24.0 (IBM Corp., Armonk, NY, USA). For the analyses of mHHS, HOS-ADL, and VAS for pain before surgery and at the final follow-up, paired t-tests were used. Independent t-test was used to compare the changes in Tönnis grades between groups. Changes in values by the time of hip joint ROM measurement and those by the time of measurement between groups were analyzed using repeated measures ANOVA. In all analyses, P<0.05 was defined as being significantly different.
Go to :
RESULTS
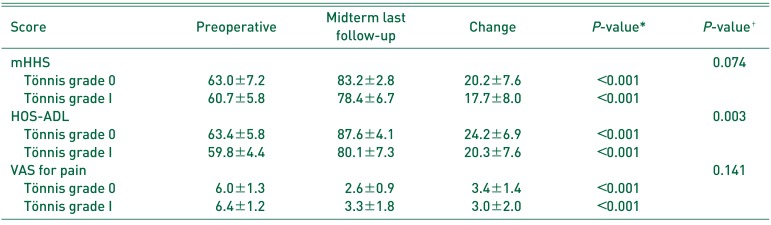
When comparing clinical outcomes at latest follow-up with preoperative assessments, all outcomes tested were significantly improved at each follow-up period (Fig. 2). At the latest follow-up, the mean preoperative and final mHHS and HOS-ADL improved from 61.2 and 60.6 to 79.5 and 81.8, respectively. The mean VAS pain score decreased from 6.3 to 3.2 (P<0.001). Clinical outcomes in patients with Tönnis grade 0 and I were significantly improvements. Differences were observed in the levels of change only in HOS-ADL among those groups (Table 2). The mean VAS satisfaction score at the midterm last follow-up was 7.8 out of 10.
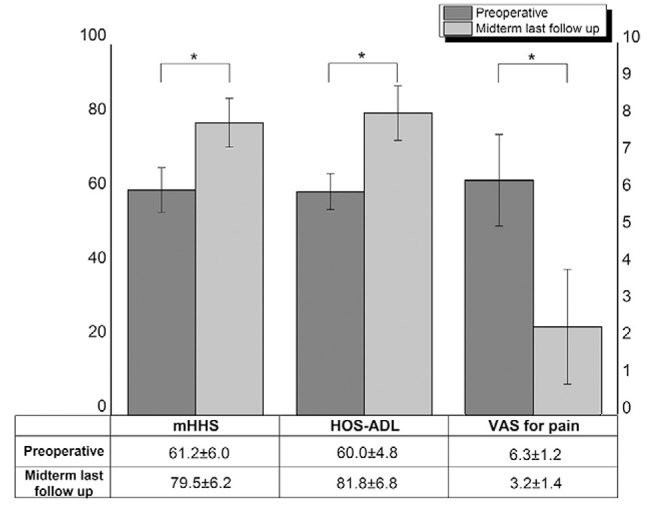 | Fig. 2Patient-reported outcomes (PROs) collected preoperative and at the midterm last follow-up. There was a significant difference in all PROs between preoperative and midterm last follow-up.mHHS: modified Harris hip score, HOS-ADL: hip outcome score-activities of daily living, VAS: visual analogue scale.
* Paired t-test, P<0.001.
|
Table 2
Patient-reported Outcomes of the Two Groups Divided by Tönnis Grade (0 and I)
Values are presented as mean±standard deviation.
mHHS: modified Harris hip score, HOS-ADL: hip outcome score-activities of daily living, VAS: visual analogue scale.
* P-value: Paired t-test between before and after surgery.
† P-value: Independent t-test comparison of change values between before and after surgery by group.
![]()
Although the mean range of internal rotation and flexion increased from prior to surgery to 1-year after surgery, these values were slightly lower at the final follow-up (Fig. 3A). Significant differences were observed in changes in internal rotation and flexion values over time (P<0.001). Repeated measures ANOVA revealed significant differences in the mean changes in ROM between Groups 1 and 2 divided to determine the effects of osteoplasty on ROM changes (Fig. 3B, C).
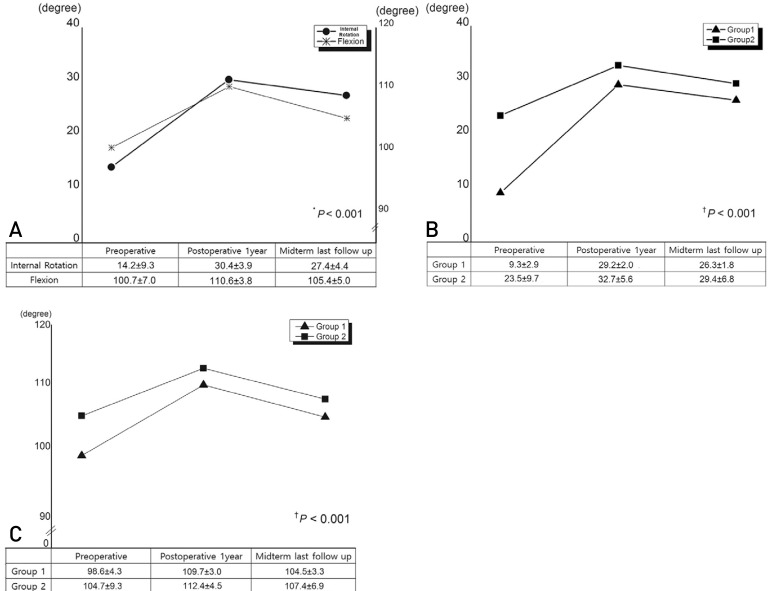 | Fig. 3The graphs reveal changes in range of motion over time. (A) Significant differences were observed between changes in the mean of internal rotation and flexion over time. (B, C) Repeated measures ANOVA revealed significant differences in the mean range of motion (ROM) (internal rotation, B; flexion, C) changes between the Group 1 and Group 2 divided to determine the effects of osteoplasty on ROM changes.Group 1: patients diagnosed with femoroacetabular impingement, diffuse idiopathic skeletal hyperostosis, ankylosing spondylitis, Group 2: patients diagnosed with the others.
* Huynh-Feldt epsilon, P<0.001
† Repeated measures ANOVA, P<0.001.
|
At index surgery, 41 patients had Tönnis grade 0, 148 had Tönnis grade I (mean, 0.78). At the final follow-up, 18 patients had Tönnis grade 0, 127 had Tönnis grade I, 38 had Tönnis grade II, and 6 had Tönnis grade III (mean, 1.17).
Eight patients (4.2%) underwent revision arthroscopic surgery and three (1.6%) were converted to THA. Patients undergoing revision arthroscopy included three cases of labral tear without evidence of FAI, two cases of FAI with labral tear, one case of ankylosing spondylitis, borderline dysplastic hip, and synovial chondromatosis. Three patients who were converted to THA were diagnosed as experiencing early degenerative osteoarthritis, chondrocalcinosis (Fig. 4), and septic arthritis. Conversion to THA was performed in all of these three patients, since they had Tönnis grade III at the time of re-surgery and reported pain VAS scores of 7 to 8.
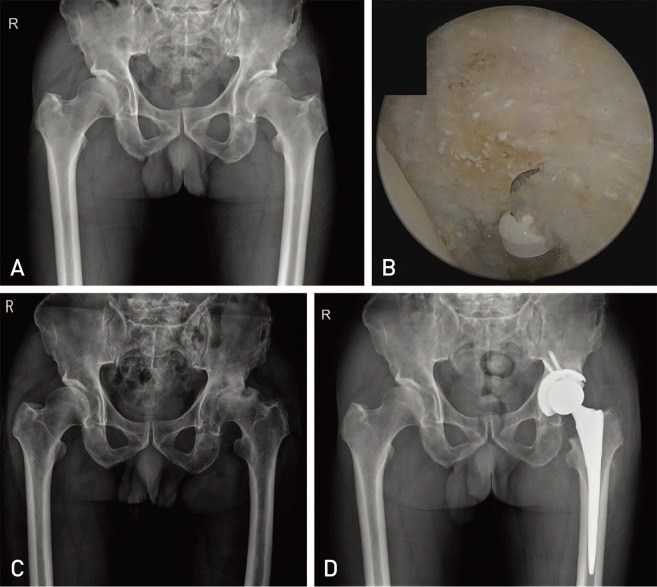 | Fig. 4A 64-year-old male received arthroscopic partial removal of chondrocalcinosis and debridement on left hip. Primary diagnosis was chondrocalcinosis and borderline dysplastic hip. (A) This patient had a dysplastic hip on the right side and a borderline dysplastic hip on the left side (lateral center edge angle: 16° on right hip, 21° on left hip), and chondrocalcinosis on both sides. A Tönnis grade of 0 was observed in the preoperative period. (B) Arthroscopic debridement was performed on anterosuperior labrum. Calcific materials were observed. (C) A Tönnis grade III osteoarthritis was noted at the 12-month follow-up and his visual analogue scale for pain was 8. (D) He underwent conversion to total hip arthroplasty.
|
Go to :
DISCUSSION
Studies regarding clinical outcomes after hip arthroscopy in middle-aged patients with early osteoarthritis of various diagnoses are uncommon1516). This study demonstrates that: (1) the mean preoperative and final mHHS and HOS-ADL were significantly improved at latest follow-up and (2) the mean VAS decreased significantly. The mean ROM of patients also increased, and the VAS safisfaction score was 7.8 out of 10. The results of this study suggest that middle-aged patients with early osteoarthritis have good clinical results after hip arthroscopy.
Although pain and clinical symptoms improve after hip arthroscopy, surgical outcomes in patients with more severe osteoarthritis became worse1516). Horisberger et al.22) identified that those with Tönnis grade III have poorer prognoses compared with those with Tönnis <III. Several other studies also suggested better prognosis in groups with lower Tönnis grades232425) and others identified an association between intraoperative cartilage degeneration and poor prognosis1026). According to Philippon et al.27), patients aged 50 years or older with joint space width of less than 2 mm needed THA 9.9 times more than younger patients. A follow-up study pointed that in patients older than 50 years of age who underwent hip arthroscopy for FAI, about 80% with joint space width of less than 2 mm underwent THA28). Herrmann et al.10) also noted that patients older than 40 years of age with a joint space width of <2 mm had a 75% likelihood of receiving THA.
Bedi et al.29) found that appropriate osteoplasty in symptomatic patients with FAI can improve ROM and reduce secondary chondral injury through CT and 3-dimensional modeling. In this study, internal rotation and flexion increased significantly after surgery, especially among patients receiving osteoplasty (Group 1) (P<0.001). The leading cause of revision arthroscopy is insufficient osteoplasty3031). Ross et al.30) found that 90% of symptomatic patients (45 of 50) with residual deformity received resurgery. Philippon et al.31) reported that re-surgeries were performed approximately 20.5 months after FAI and that the leading causes included hip pain, decreased ROM, and functional disability. After re-surgery, most patients were reported to partially recover from decreased functions within 1 year. In this study, six out of eight cases of revision arthroscopy were thought to be caused by insufficient osteoplasty. After sufficient re-osteoplasty, all six patients had improved symptoms.
Kemp et al.16) reported that patients with hip osteoarthritis received conversion to THA about 2 years after hip arthroscopy, while about 9.5% to 50% of patients in another review by Piuzzi et al.15), depending on the articles, underwent THA after a mean of 13.5 months. In our experience, during the 3- to 9-year midterm follow-up, three patients (1.6%) received conversion surgery to THA. Here, it was thought that as surgery was only indicated in patients with early osteoarthritis or low Tönnis grade, lower THA conversion rates compared with other articles was achieved.
In this study, the mean Tönnis grade rose from 0.78 to 1.17, however, the clinical outcomes achieved were good. Kim et al.32) reported that hip pain was discordant with radiographic hip osteoarthritis. Repair of the labrum (which has sensory nerve endings), and osteoplasty (to prevent impingement) were thought to be the most important causes of pain relief33). In addition, increased ROM due to sufficient osteoplasty may have contributed to the improvement of clinical results and patient satisfaction.
This study has some limitations. First, it is retrospective in nature and used midterm follow-up data. Secondly, patients had a variety of diagnoses and with the exception of FAI and labral tear, most diagnoses included a relatively small number of patients, hence, size bias can occur in the interpretation of study results. Thirdly, selection bias can occur as all patients were treated in the outpatient setting. A possible explanation is that the skilled arthroscopy surgeon with his experience and knowledge selected patients to receive surgery who might inherently achieve good clinical outcomes. Finally, patients with diagnoses other than FAI rarely had early osteoarthritis with Tönnis grade 0. If the severity of osteoarthritis had been radiologically divided using Tönnis classification before surgery and there had been a control group, better outcomes might have been obtained.
Go to :
CONCLUSION
This study finds that patients with early-staged osteoarthritis of various diagnoses and with Tönnis grade 0 and I achieve improved clinical outcomes. Therefore, hip arthroscopic procedures in middle-aged patients can be a good surgical option if the surgeon selects appropriate patients and uses proper surgical procedure (e.g., sufficient osteoplasty).
Go to :
 XML Download
XML Download