

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Three-dimensional (3D) printing technology is additive manufacturing that produces 3D shapes by stacking twodimensional (2D) cross-sectional shapes with various materials. It is used for laminated manufacturing, such as rapid prototyping (RP). In the early days, there were a number of key limitations in printing materials, molding time, size, precision and strength of the moldings, which limited industrial uses. In recent years, however, printing materials have been diversified including metals, and printing equipment has been developed accordingly. The paradigm of industrial use is rapidly changing as the production of complex shapes and customized products become possible.
Today, 3D-printing technology can be used to create simulation models or medical implants, thus significantly aiding doctors and medical companies by optimizing the way a surgeon plans and executes a procedure1). The application of 3D-printing technology to clinical medicine has already become the fastest growing innovation in the medical field2).
The use of 3D-printing in the field of orthopaedic surgery is rapidly increasing. The ease of segmenting bone from computed tomography (CT) scans, and the variety of available 3D printers enables researchers, manufacturers, and surgeons to easily use 3D-printing technology. Over the last decade, there have been significant developments in the orthopedic surgery field, especially in hip and pelvic surgeries. Many scientific papers have been published regarding research in the field of 3D-printed hip prosthesis3).
Currently, the use of 3D-printing technology in hip and pelvic surgeries can be divided into four important categories. First is the development of anatomical models based on patient imaging; these bone models can facilitate an improved understanding of the patho-anatomy and surgeons can use it to simulate the surgery to potentially improve execution. Second is the synthesis of patient-specific instruments (PSI) that may increase the accuracy of a surgery; most PSIs are manufactured in the form of guides or jigs. Third is the production of arthroplasty implants; 3D-printed hip implants are advantageous because ingrowth surfaces can be modified to optimize bony ingrowth. Forth is the development of custom implants. Unlike standard sized implants, a custom implant created using patient-specific medical images can be a perfect match for the patient's unique anatomy. Importantly, the use of 3D-printed custom implants has recently been reported in not only pelvic tumor surgery but also in difficult revision hip arthroplasty with severe acetabular bone loss4).
PREOPERATIVE PLANNING AND SIMULATION
In conventional orthopedic procedures, surgeons have to integrate all preoperative 2D images and formulate a 3D-surgical plan. 2D-CT images can be reconstructed into 3D-stereoscopic images, but eventually the information is received two-dimensionally by the surgeon via a computer monitor. For surgeries involving the hip and pelvis, preoperative planning is particularly difficult especially in cases of complex anatomy and severe deformity. Therefore, a variety of new preoperative planning methods are being developed, such as via digital radiographs5). Above all, however, 3D-printed anatomical models provide surgeons with an opportunity to better understand individual patient anatomy. Simulation surgery using 3D-printed bone models allows a surgeon to develop better surgical approaches, test the feasibility of procedures and determine the optimal location and size of implants.
1. Intertrochanteric Fractures
Intertrochanteric fractures (ITF) are one of the most common fractures of the hip and primarily occur in elderly people with osteoporosis. Intramedullary fixation has become the most commonly used method of treating unstable ITF. Zheng et al.6) performed CT scanning and used proximal femur nail antirotation (PFNA) with a 3D RP model for a group of 19 patients and compared outcomes to another group (n=20) who underwent conventional PFNA operation. The 3D RP model was generated using the fused deposition modeling technique and the length and diameter of the main screw blade was measured during the simulation. It was demonstrated that the 3D RP model-assisted procedure resulted in more effective reduction of the neck shaft angle. Furthermore, patients undergoing surgery with the 3D RP model experienced a significant reduction in surgery duration (P<0.01), and reductions in intraoperative (P=0.02) and postoperative (P=0.03) blood loss, compared with those treated with conventional surgery. In this study, the 3D RP modelling technique was able to create an accurate model of the ITF, which facilitated surgical planning and fracture reduction, thus improving the efficiency of PFNA surgery for ITFs.
2. Acetabular Fractures
Treatments for acetabular fractures aim to restore the biomechanical property of the pelvis and acetabulum through reconstructing the articular surface and restoring anatomical structure. Because of the complex anatomy of the pelvis and nearby neurovascular structure, acetabular fracture surgery has always been challenging.
In 2015, Yu et al.7) published on the benefit of augmented stereoscopic 3D CT reconstructions to allow for an appreciation of the normal 3D anatomy of the pelvis on the fractured side and use of models for subsequent intraoperative contouring of pelvic reconstruction plates. In 2019, Chen et al.8) summarized the results of a retrospective analysis of 52 bicolumnar acetabular fracture cases which were divided into two groups for comparison; patients in group A (n=28 patients) underwent, computer-assisted virtual surgical procedures and 3D printing of patient-specific precontoured plates, while patients in group B (n=24) were treated with the conventional method. Fracture type, operative blood loss, surgical time, complications, radiographic quality of reduction, and hip function were compared between groups. The final surgical procedure conducted on all patients in group A was almost identical to the preoperative virtual operation. Operative time and intraoperative blood loss were significantly reduced in group A compared with group B (P<0.05); quality of postoperative fracture reduction and patient satisfaction with resultant hip function was also slightly higher in group A compared with group B (Fig. 1).
3. Total Hip Arthroplasty
Total hip arthroplasty (THA) in dysplastic hips or sequelae of septic arthritis is technically demanding due to the distorted anatomy. Patient specific (CT-based), 3D RP models were used to plan for acetabular cup placement so that a surgeon could identify pelvic structures, assess the ideal extent of reaming and determine the size of cup after a reconstructive procedure.
In 2013, Won et al.9) published the results of a THA study using an RP model in 21 complex hips; all surgeries were completed successfully and the acetabular component used was within 2 mm of the predicted size in 17 hips (80.9%). All of the acetabular components and femoral stems had radiological evidence of bone ingrowth and stability at the final follow-up (mean, 35.5 months), without any detectable wear or peri-prosthetic osteolysis. Several similar studies have been reported in recent years1011).
PATIENT SPECIFIC INSTRUMENT
Orthopaedic surgeons and engineers are constantly looking for methods to improve the surgical positioning of prostheses in accordance with the purpose of the operation. Navigations and robotics have been used to improve the accuracy of hip surgery but have had limited use because of high costs, increased operative times and other logistical issues. More recently, PSI has been developed to guide the positioning of a prosthesis during orthopaedic surgery. We reviewed the currently reported PSI techniques used for hip surgery.
1. Femoro-acetabular Impingement
Cam-type femoro-acetabular impingement (FAI) can be treated by performing an osteochondroplasty to remove the excess impinging bone from the head neck junction of femur. Verma et al.12) reported a case of Cam-type FAI in an 18 year-old male, who underwent surgical treatment by osteochondroplasty. CT-based virtual surgical planning was conducted to design the femoral head and neck jigs, which were 3D printed and used intra-operatively to guide for adequate and optimum excision of bone at the femoral head neck junction. They concluded that their customized jigs were accurate and useful for the surgery.
2. Osteonecrosis of Femoral Head
For the treatment of early osteonecrosis of femoral head, the conventional method of core decompression is usually performed under C-arm fluoroscopy. However, in 2018, Li et al.13) reported the clinical efficacy of a 3D-printing guide plate for core decompression instead of C-arm fluoroscopy. The 3D-printed guide plate could be tightly attached to the proximal part of the femur during the operation and one Kirschner wire could be inserted into the pinhole on the guide plate to obtain an appropriate decompression position. Compared with 20 patients who underwent conventional core decompression under C-arm, fluoroscopy time, and intraoperative blood loss in 20 patients treated with a 3D-printing guide plate was significantly less. There was also a significant difference between the groups in the last follow-up of Harris hip scores (HHS).
3. Total Hip Arthroplasty
Recently, PSI has been developed to guide the positioning of components during hip arthroplasty. This technique uses imaging techniques such as CT and magnetic resonance imaging to plan surgery in a virtual 3D environment. The surgeon can plan orientation and position of the prosthesis relative to a chosen standard frame of reference and execute the plan using simple intraoperative patient-specific guides.
Acetabular guidance systems aim to optimize the cup size, implant medialization, anteversion, and inclination. Femoral guidance systems aim to optimize the stem size and alignment, offset, leg length (height of neck cut), and stem version. Several PSI systems (e.g., Signature Hip [Zimmer Biomet], OPS [Corin Group], Hip Plan [Symbios], and MyHip [Medacta]) are currently licensed for use in the United States and Europe14) (Fig. 2).
PSI THA guides have been shown to improve the accuracy of implant positioning and may play an important role in reconstructing complex anatomy. In a prospective randomized controlled trial, Small et al.15) compared 18 patients undergoing THA with conventional instrumentation and 18 patients undergoing THA with PSI. Results demonstrated a statistically significant difference in version of the acetabular component between standard instrumentation and PSI. However, the effects on long-term functional outcomes or survival of PSI THA guides are controversial. More clinical research is needed to better characterize the potential benefits of PSI in terms of surgical accuracy.
PROSTHESES SYNTHESIZED WITH 3-DIMENSIONAL-ADDITIVE MANUFACTURING
Most applications of 3D-printing technology in the orthopedic area have focused on high customization or patient-specific manufacturing. On the other hand, advances have been made in terms of materials that can be leveraged along with 3D-printing technology. In particular, the material called trabecular titanium, which has a structure similar to the trabecular bone of the human body, can be reproduced only with high-quality additive manufacturing technology. By applying trabecular titanium material to a hip prosthesis, it is possible to produce a prosthesis that is mechanically stability, biocompatible while promoting osseointergration.
1. High Porous 3-dimensional-printed Trabecular Titanium Cup
Recently, the development of electron beam melting 3D-printing technology has led to orthopaedic manufacturing with integrated trabecular surfaces, melting thin layers of metal powder in finely tuned 3D constructs1617). This additive manufacturing provided a bulk cup with a constant porosity (65%), each pore sizing 700µm16). Such a pore size, which is not achievable through conventional manufacturing approaches was demonstrated to provide a high fixation capacity in the early weeks and a deep bone ingrowth in an in vivo study by Taniguchi et al.18). Asti et al.19) also reported the results of an in vitro study revealing that a trabecular titanium scaffold facilitated better osseointegration compared with other synthetic scaffolds.
Hip prostheses made from high porous trabecular titanium is already used worldwide. In 2019, Castagnini et al.20) reported eight years results comparing and evaluating survival rates and reason for revisions with trabecular titanium cups and conventional cementless cups. Trabecular titanium cups had a statistically higher survival rate compared with the control group and a statistically lower incidence of cup aseptic loosening (Fig. 3).
2. High Porous 3-dimensional-printed Stems
Arabnejad et al.21) reported that 3D-printed fully porous implants can reduce the amount of bone loss secondary to stress shielding by 75% compared to a conventional fully solid implant. This result also agrees with those of the in vitro quasi-physiological experimental model and the corresponding finite element model for both the optimized fully porous and fully solid implant. These studies demonstrate the merit and potential of modifying material architecture to achieve substantial reduction of bone resorption secondary to stress shielding (Fig. 4).
CUSTOM PROSTHESES
Custom implants may be indicated when: (i) patients' bony geometries fall outside the range of standard implants with respect to implant size- or disease-specific requirements, and (ii) improved surgical results are anticipated due to a better fit between implants and patients' anatomical needs22).
1. Revision Total Hip Arthroplasty
The management of acetabular bone loss is a challenging problem in revision THA2324). Multiple surgical reconstruction options have been described for severe acetabular defects including use of a jumbo acetabular cup, impaction bone grafting combined with a cemented cup, structural allograft, oblong acetabular cup, antiprotrusio cage, and cup-cage construct2526272829). Several studies have assessed a technique to analyze the defect in detail and to reconstruct the acetabulum using a custom-made trabecular titanium implant that matches the anatomy of the bone deficient acetabulum, taking into account the patient's bone quality to achieve primary implant stability293031). Custom-made triflanged acetabular components (CTAC) were developed to restore hip biomechanics and achieve primary implant stability, even in cases of extreme acetabular bone loss. Implant stability is favored by maximizing host bone contact and by three flanges that fit the iliac, ischial and pubic bone32333435). The design of CTACs implants is based on 3D models produced from CT scans. Patient-specific bony situation is evaluated and an implant proposal is formulated including a biomechanical assessment. The implant proposal also includes patient-specific screw positions based on bone quality and drill guides to achieve the planned position. Moreover, the medial side of CTACs implants can be developed with a porous defect-filling scaffold to promote osteointegration (Fig. 5).
De Martino et al.36) published a systematic review of 17 articles assessing the clinical results of CTACs; a total of 579 CTACs were implanted. The all-cause revision-free survivorship was 82.7%. The overall complication rate was 29%. Dislocation and infection were the most common complications observed with an incidence of 11% and 6.2%, respectively. This could be due to the extensive approach and the poor quality of the soft tissues in multi-operated patients.
According to current data, CTACs have a high incidence of complications. However, since most cases have been used in patients with significant acetabular bone loss or pelvic discontinuity, CTACs remain an efficacious treatment option and have potential for development. Despite a high complication rate, the use of such implants seems justified in carefully selected patients with massive uncontained acetabular bone defects.
2. Tumor
Historically, the most common method of managing periacetabular malignant bone tumors was hindquarter amputation or external hemipelvectomy37). Prosthetic reconstruction may be a promising treatment for peri-acetabular malignant bone tumors with advances in radiotherapy and chemotherapy38394041). However, this approach is associated with a high complication rate. Therefore, research on prosthesis design is needed, and 3D-printing technology is emerging as an alternative because of acceptable cosmesis, immediate stability, and the possibility of rapid recovery, as well as early weight-bearing activity. Recently, 3D-printed prostheses have been used for hemipelvic reconstruction and have obtained good short-term functional results4243).
Liang et al.44) reported the results of 35 patients who underwent resection of a pelvic tumor and reconstruction using a 3D-printed prosthesis. Three patients underwent reconstruction using an iliac prosthesis, 12 using a standard hemipelvic prosthesis and 20 using a screw-rod connected hemipelvic prosthesis. After a mean follow-up of 20.5 months, 25 patients survived without evidence of disease, five were alive with disease and five had died from metastatic disease. For the surviving patients, the mean clinical score (Musculoskeletal Tumor Society 93 score) was improved.
Wang et al.45) reported 11 patients with periacetabular malignant bone tumors treated by personalized 3D-printed hemipelvic prostheses after en bloc resection. During an average follow-up of 15.5 months, patients have shown acceptable functional results without severe complications. Hip dislocation was detected in two patients, while delayed wound healing occurred in one patient. Local tumor recurrence was not observed. They concluded that reconstruction arthroplasty using 3D-printed pelvic prostheses can facilitate the precise matching and osseointegration between implants and the host bone. Reconstruction arthroplasty using 3D-printed pelvic prosthesis provides a promising alternative for those patients with peri-acetabular malignant bone tumors.
DISCUSSION
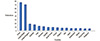
An increase in research and publications involving 3D-printing applications in orthopedic surgery and related fields was observed, especially in recent ten years. Overall, most papers were published from China (75 papers), followed by United States (69 papers), United Kingdom (17 papers), Australia (15 papers), and India (11 papers). The number of studies published in Korea (8 papers) on orthopaedic applications of 3D-printing technology is relatively low compared to that of the USA, China, and advanced European countries (Fig. 6)46).
3D-printing technology has many advantages when applied to orthopaedic surgeries, especially in the hip and pelvis, however, it is not without its limitations. Firstly, the accuracy and resolution remain to be further proven. Soft tissue and cartilage are usually excluded during the processing of CT-based radiological images. Depending on the purpose of technology, the inclusion of such information may be affected. When constructing a 3D-printed model or PSI, structures such as blood vessels, nerves and tendons are not taken into account, which may lead to unexpected problems during surgery. Moreover, the 3D printing process can be influenced by artificial factors. Additionally, the cost of 3D printing is relatively expensive. At present, the cost for a 3D model of the hip and hemipelvis can vary from $200 to $1,000 depending upon factors, such as the materials used, the size of the print, and the type of printer used47).
A few years ago, only plastics could be 3D-printed into anatomic models and PSIs. Then, metal powders, such as titanium or cobalt-chrome, were used to fabricate custom implants by 3D printing48). The advances in biomimetic materials for 3D printing will be one major direction for future development in 3D-printing technology applied to the development of patient-specific orthopedics. The material should be biocompatible and sterilizable for intraoperative use49).
Surgeons might not easily master the steps in the working process such as image postprocessing, creating 3D images that highlight regions of interest, planning a surgery with various reconstructive options, and even preoperative biomechanical evaluation of the implant design or a reconstructive method. To increase the popularity of 3D-printing technology among orthopedic surgeons, an integrated all-in-one computer platform should be developed to allow for easy planning and seamless communication among different care providers (e.g., radiologists, orthopaedic surgeons, engineers, implant companies)50)
In order to actively apply 3D-printing technology to the hip surgery field and expand the market, there is a need to improve the medical insurance cost. Let's take a look at the situation in countries that are leaders in 3D-printing technology. The US FDA applies an exception that exempts the approval process for cases where 3D-printing related medical technologies are not based on FDA guidelines, but where their effectiveness and safety are demonstrated. In Japan, national medical insurance have been applied to 3D-printing simulation modeling techniques since 2016. Currently, preoperative planning and simulation surgery using 3D-printing technology is used to perform various orthopaedic surgeries, including hip and pelvic surgery.
In Korea, some surgeons have combined 3D-printing technology with orthopaedic surgery and consistently appreciate its usefulness and potential, however, the government's policies have not yet reached the level of advanced countries. In particular, in orthopaedic surgery, despite the fact that 3D-printing technology has many possible applications and may be the best option in certain cases, more effort to gain government support is required. Also, the Korean FDA should be more proactive to ensure that the standards and guidance for 3D applications can guarantee the safe and effective use of 3D-printed orthopaedic devices.
For the hip and pelvis, simple plastic bone models are very useful in planning some difficult cases of fracture and arthroplasty for deformed hips. PSI may have limited additional benefits for routine hip arthroplasty, but maybe much useful in complex pelvic tumor resection and complex reconstruction. 3D-printed metallic implants are increasingly used for the reconstruction of critically sized acetabular defects in complex revision hip replacement surgery and tumor endoprosthetic reconstruction in many countries. We look forward to seeing a larger series of clinical studies, but the guidelines are still lacking. In the near future, access to 3D-printing technology will gradually increase in the medical field. Orthopaedic surgeons should be aware of the various degrees of regulatory requirements imposed by different countries and implement necessary validation and quality assurance steps when using customized tools and implants. Orthopaedic surgeons should also develop guidelines that increase the benefit of patients through discussion and collaboration with governments and engineering groups.





 XML Download
XML Download