

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Severe fever with thrombocytopenia syndrome (SFTS) is an emerging hemorrhagic infectious disease caused by the SFTS virus (SFTSV), renamed Huaiyangshan banyangvirus (genus Banyangvirus; family Phenuiviridae) [1]. SFTS has become an endemic disease in central and eastern China, Japan, and Korea, with a high mortality rate (6.3%–30%) [23]. The clinical manifestation of early stage SFTS is non-specific with fever, headache, myalgia, and gastrointestinal symptoms, followed by thrombocytopenia and leukopenia [4]. In fatal cases, multiple organ failure develops with other clinical symptoms, including disseminated intravascular coagulation, neuropsychiatric symptoms, and sustained thrombocytopenia [2].
Early diagnosis and effective management of SFTSV infections require accurate and reliable diagnostic assays. Several molecular assays have been developed and are currently used for SFTS diagnosis, such as real-time reverse transcription (RT)-PCR and loop-mediated isothermal amplification combined with reverse transcription. The majority of molecular assays were de1signed to target the L, M, or S segments of the SFTSV genome; of these, the S segment is known to be the most conserved gene [5678910].
The SFTS-QS kit (MiCoBioMed, Seongnam, Korea) is a new molecular assay for the rapid detection of the S segment of SFTSV; it is a one-step real-time RT-PCR kit based on lab-on-a-chip technology. The PowerChek SFTSV Real-time PCR kit (PowerChek kit; Kogene Biotech, Seoul, Korea) is another new one-step real-time RT-PCR kit for the qualitative detection of the S and M segments of SFTSV. The performances of the two kits have not been compared previously. We evaluated the analytical and clinical performance of the SFTS-QS kit in comparison with that of the PowerChek kit for the qualitative detection of SFTSV.
This study was approved by the Institutional Review Board (IRB) of the Samsung Medical Center, Seoul, Korea (IRB No. SMC 2016-05-043), and informed consent requirements were waived. From July 2013 to July 2019, a total of 117 serum samples from patients with clinically suspected SFTS were collected and stored at −70℃ until analyzed. Eleven other viral pathogens ((Dengue virus type 1 [Hawaii strain, ZeptoMetrix, Buffalo, NY]), Dengue virus type 2 [New Guinea C strain, ZeptoMetrix], Dengue virus type 3 [H87 strain, ZeptoMetrix], Dengue virus type 4 [H241 strain, ZeptoMetrix], Yellow fever virus [17 D strain, ZeptoMetrix], Japanese encephalitis virus [KUMC-27, Korean Bank for Pathogenic Viruses, Seoul, Korea], Seoul virus [clinical isolate], Hantaan virus [clinical isolate], and Zika virus [MR766, PRVABC59 strains, American Type Culture Collection, Rockville, MD; DakArD41662 strain, ZeptoMetrix]) were used to evaluate analytical specificity.
Viral RNA was extracted from the collected serum samples using the QIAamp DSP Viral RNA Mini Kit (QIAamp kit; Qiagen, Hilden, Germany), according to the manufacturer's protocol. The total volume of samples was 200 µL. The RNA was eluted in 100 µL, and the two real-time RT-PCR assays were simultaneously performed. The remaining RNA samples were stored at −70℃ until use in Sanger sequencing.
Analysis using the SFTS-QS kit was performed on the Veri-Q PCR 316 system (MiCoBioMed, Seongnam, Korea), according to the manufacturer's instructions; the total reaction volume was 10 µL (7 µL of PCR mixture and 3 µL of template RNA). The SFTSV cut-off value was set at a cycle threshold (Ct) value ≤40. SFTSV-positive/negative controls and an internal control were included in each run.
Analysis using the PowerChek kit was performed on the Bio-Rad CFX96 system (Bio-Rad Laboratories Inc., Hercules, CA, USA) in a total volume of 20 µL (15 µL of PCR mixture and 5 µL of template RNA), according to the manufacturer's instructions. Positive results were defined by a Ct value ≤35 for the S or M segments.
Sanger sequencing targeting the S and M segments of SFTSV was used as a reference method and performed according to previous studies [1112]. Nested RT-PCR was performed for the S segment; a second round of amplification was conducted if no product was visible in agarose gel electrophoresis after the first round. Following detection by agarose gel electrophoresis, the PCR product was purified and sequenced.
The analytical specificity of the SFTS-QS kit was determined using the 11 viruses listed above. The limit of detection was evaluated using SFTSV RNA transcripts. Probit analysis was used to determine the 95% limit of detection, and serial dilutions were analyzed with eight replicates per dilution, according to the Clinical Laboratory Standards Institute (CLSI) EP17-A2 [13]. Precision, including reproducibility and lot-to-lot precision, was determined using two concentrations, according to a modified CLSI EP15-A3 protocol [14]. Reproducibility was assessed by triplicate analysis of each concentration for five days at two different test sites. Lot-to-lot precision was evaluated by analyzing the duplicates of each concentration for five days using two different lots.
The positive percent agreement (PPA) and negative percent agreement (NPA) values and kappa coefficient were calculated to determine the agreement between the results of the SFTS-QS and PowerChek kits. The clinical sensitivities and specificities were calculated based on the results of the reference method. Statistical analyses were performed using the VassarStats website (http://vassarstats.net/).
The total turnaround time, defined as the time interval between reagent preparation for amplification and obtaining the final result, of the SFTS-QS and PowerChek kits was measured for workflow analysis. It was measured for processing five samples in a batch.
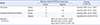
Of the 117 serum samples, 14 and 16 were SFTSV-positive by the SFTS-QS and PowerChek kits, respectively; 14 of these samples were identical. The SFTS-QS results were concordant with those of PowerChek for 115/117 (98.3%) samples. The agreement, including PPAs, NPAs, and kappa values, between the two kits and the accuracy, including sensitivities and specificities, are shown in Table 1. Fourteen samples were SFTSV-positive based on the reference method. The SFTS-QS and PowerChek kits correctly identified 103 and 101 of the 103 SFTSV-negative samples, respectively (Table 1). The two samples with false-positive results in the analysis with PowerChek also gave negative results in an assay conducted by the Korea Centers for Disease Control & Prevention.
The 95% limit of detection of the SFTS-QS kit was 5.3 copies/µL. In the analytical specificity assay, all 11 viruses gave negative results and no cross-reactivity was observed. In the reproducibility assay, the coefficient of variation (CV) ranged from 2.46% to 3.65%. The lot-to-lot variation CV ranged from 3.13% to 3.49%. The total time (55 minutes) required to perform the SFTS-QS assay was shorter than that required for the PowerChek assay (135 minutes).
The recent increase in SFTS cases in East Asia has highlighted the need for a reliable and rapid diagnostic method [234]. Sun, et al. [9] developed a quantitative real-time RT-PCR assay targeting the L, M, and S genes of SFTSV, which showed 98.6% clinical diagnostic sensitivity and over 99.0% specificity. In addition, a two-tube multiplex real-time RT-PCR assay developed by Yoshikawa, et al. [10] for SFTSV detections exhibited a sensitivity of 100% and a specificity of over 99%. Our study demonstrated that the SFTS-QS and PowerChek kits have good sensitivity and specificity for SFTS diagnosis.
The SFTS-QS assay performed on the Veri-Q PCR 316 system required shorter total turnaround time compared with the PowerChek kit. Based on microfluidic devices (also known as lab-on-a-chip devices), the Veri-Q PCR 316 system can achieve rapid thermal cycling by circulating pre-heated liquids in microfluidic chips positioned over the heaters, enabling the performance of 30 cycles of real-time PCR in 15 minutes [1516]. Our findings were also consistent with previous findings that PCR processing time was significantly reduced to <40 minutes (for 45 cycles) with the Veri-Q PCR 316 system compared with other real-time PCR systems, which took approximately two hours for amplification [17].
In conclusion, we demonstrate that both the SFTS-QS and PowerChek kits yielded accurate results, but the SFTS-QS kit required a shorter total turnaround time. Based on the high speed and simplicity, the SFTS-QS kit is a potentially useful diagnostic tool for the rapid detection of SFTSV.
 XML Download
XML Download