

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With limited new antibiotic classes in the drug development pipeline, the global challenge of antimicrobial resistance, particularly in the treatment of multidrug-resistant (MDR) gram-negative (GN) bacteria, remains critical. Colistin, also known as polymyxin E, has become a last-resort antibiotic for the management of MDR GN bacteria [12]. Colistin, a member of an old class of cationic, cyclic, polypeptide antibiotics was first introduced in Japan in 1947 from the soil bacterium Paenibacillus polymyxa and adopted for clinical use in 1959 [3].
Although its use was abandoned in the 1980s because of concerns of nephrotoxicity and neurotoxicity [4], intravenous injection of colistin sulfate was demonstrated to be safe and could be considered for the management of severe infections from sensitive MDR GN pathogens [5]. Therefore, beginning in the mid-1990s, the clinical use of polymyxins was revived, with a focus on colistin because of its rapid bactericidal effect, broad-spectrum activity against MDR GN pathogens, and the lack of novel antibiotics against the most prevalent MDR GN bacteria [35678910]. The global colistin resistance rate is less than 10%, but is increasing. Increased resistance has been reported in Mediterranean and Southeast Asian countries [11].
The increasing use of colistin over the past several years has necessitated rapid, accurate, and reliable in-vitro antimicrobial susceptibility testing (AST) methods to allow appropriate therapeutic decisions. The disk diffusion test, commonly used in clinical laboratories, is considered to be unreliable because colistin diffuses poorly into agar due to electrostatic interactions with acid or sulfate groups of agar, resulting in smaller inhibition zones [12]. The poor diffusion results in high error rates compared to the broth microdilution (BMD) test for minimum inhibitory concentration (MIC) determination [13]. Other methods, such as the VITEK 2 AST system (bioMérieux, Marcy l'Etoile, France), E-test (AB Biodisk, Solna, Sweden), and agar dilution, also remain unreliable [141516171819]. There is currently no standardized disk diffusion test for colistin susceptibility testing for use in clinical microbiology laboratories [20].
This study aimed to develop a simple disk diffusion test method for colistin susceptibility testing by modifying the commercial Mueller-Hinton medium to improve colistin diffusion in agar.
MATERIALS AND METHODS
Phase I
Disk diffusion test
The colistin disk diffusion test was performed using a 10 mg colistin disk on Mueller-Hinton agar (MHA) plates that were incubated at 35℃ for 16–18 hours in 5% CO2. Disk diffusion test results were interpreted based on the diameter of inhibition zone and compared with MICs determined by BMD according to the 2018 CLSI guidelines [21].
Optimization of the agar concentration
First, an optimum agar concentration was determined using four strains: P. aeruginosa ATCC 27853, a colistin-susceptible Acinetobacter calcoaceticus-baumannii complex (ACB) strain, a colistin-resistant ACB strain, and mcr-1-harboring Klebsiella aerogenes. Assays were run in triplicate. Species were identified using a Microflex LT Biotyper (Bruker Daltonics, Leipzig, Germany). MHA was modified by reducing the agar granule concentration from 100% (17 g/L) to 30% (5.1 g/L) of the concentration in commercial MHA with 10% intervals (Becton, Dickinson, & Company, Sparks, MD, USA). The optimum concentration was determined based on the least agar concentration that was manageable in the laboratory. Lower the agar concentration, more fragile is the AST determination. The final agar concentration was reduced to 30%.
Optimization of the protamine concentration
We added protamine (Sigma-Aldrich, St Louis, MO, USA) to the modified MHA at various concentrations (1,000 µg/mL, 700 µg/mL, 400 µg/mL, 300 µg/mL, 200 µg/mL, 150 µg/mL, 100 µg/mL, and 50 µg/mL) to determine an optimal concentration that would promote colistin diffusion in agar, but not inhibit bacterial growth. Protamine was measured, mixed with distilled water until completely dissolved, and then added to the MHA before autoclaving.
Phase II
Colistin MIC and inhibition zone diameter around colistin disks on modified MHA
In total, 60 GN clinical isolates obtained from Severance hospital, including P. aeruginosa (N=27) and ACB (N=33), were tested (Table 1). The study was approved by the Institutional Review Board of Yonsei University Health system, Seoul, Korea. (1-2017-0079). The clinical strains were collected from sputum and urine in 2017 and stored at −70℃.
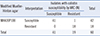
Quality control was performed using E. coli (ATCC 25922), P. aeruginosa (ATCC 27853), and mcr-1-harboring K. aerogenes (a clinical isolate). Colistin MICs were determined by BMD for all 60 strains using colistin sulfate salt (Sigma-Aldrich, St. Louis, MO, USA) and polystyrene 96-well microplates (Corning, NY, USA). As shown in Table 1, disk diffusion AST results were interpreted based on the breakpoints, which showed good agreement with the MIC determined by BMD according to the 2018 CLSI guidelines [21]. Each strain was tested using predetermined media, i.e., commercial MHA (100% agar concentration), MHA with 30% agar (MHA30), and MHA30 with 100 µg/mL protamine (MHA30P100), which were selected based on the optimization in phase I. The colistin disk diffusion test was performed using a 10 mg colistin disk on MHA plates that were incubated at 35℃ for 16–18 hours in 5% CO2.
Statistical analysis
Descriptive and statistical analyses were performed using SPSS 21 (Armonk, NY, USA) and MedCalc Statistical Software 18.10 (MedCalc Software, Ostend, Belgium; http://www.medcalc.org). Colistin MICs, as reference test, and disk diffusion results were compared to calculate sensitivity, specificity, and Kappa value of this simple disk diffusion test. Area under the curve (AUC) for inhibition zone diameters cutoff was determined from the receiver operating characteristic curve. P<0.05 was considered statistically significant.
RESULTS
Phase I
Colistin diffusion was optimized using MHA30, because we could not use the MHA with 20% or 10% agar (data not shown). At 30% agar concentration, the addition of protamine inhibited bacterial growth and enhanced colistin diffusion. Colistin diffusion in the agar improved with protamine supplementation and a reduction in the agar concentration Su. Inhibition zone diameters on MHA30P100 and MHA30 supplemented with 150 µg/mL of protamine (MHA30P150) were similar for all bacterial isolates tested. MHA30P100 was determined as the optimal medium because bacterial growth was hampered at higher protamine concentrations (Supplemental Data Table S1).
None of the strains grew on MHA30 with ≥300 µg/mL of protamine. However, colistin-susceptible ACB strain, P. aeruginosa ATCC 27853, and K. aerogenes strains grew well on MHA30 supplemented with 200 µg/mL of protamine, whereas colistin-resistant ACB strains did not. Both P. aeruginosa and ACB strains grew well on MHA30P150 (Supplemental Data Table S1). Inhibition zone diameters differed between MHA30P100 and MHA30P150 (P<0.001) (Fig. 1). Hence, we decide to adopt MHA30P100.
Phase II
We could not discriminate between colistin-susceptible and -resistant strains using commercial MHA. The categorical agreements between MICs determined by BMD were 100% in P. aeruginosa (27/27) and 97% in ACB (32/33), when bacteria were grown on MHA30P100 (Table 1). Inhibition zone diameters were larger on MHA30P100 than on MHA and MHA30 (Table 2, Fig. 1). The overall agreement between MICs and MHA30P100 inhibition zone diameters was excellent, with a kappa value of 0.961 (95% confidential interval (CI), 0.885–1.0, P<0.001). The agreement was 100% for P. aeruginosa and colistin-susceptible ACB isolates, whereas it was 94.7% (18/19) for colistin-resistant isolates. A strain of Acinetobacter nosocomialis was susceptible in disk diffusion testing using MAH30P100, but resistant in BMD testing (Table 2).
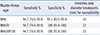
The sensitivity and specificity of colistin disk diffusion testing by using MHA30P100 were 94.7% and 100%, respectively (Table 3). By analyzing the AUC, we found that MHA30P100 medium allowed the best discrimination between susceptibility and resistance in both P. aeruginosa and ACB strains. The AUC of MHA30P100 was 0.995 (95% CI, 0.982–1.0) which was higher than that for MHA (0.979, 95% CI, 0.939–1.0) and MHA30 (0.985 95% CI, 0.953–1.0).
During colistin MIC determination, three ACB strains showed discrepancies of >8 µg/mL between MICs using BMD and disk diffusion, and were retested twice using glass tubes to rule out false resistance finding due to colistin binding to polystyrene wells, which has been previously reported [2223]. Two strains were susceptible to colistin in reference BMD methods, resulting in the same category with disk diffusion tests. However, one strain remained colistin resistant, which was retested using MHA30P100 directly from glass tubes containing 0, 0.5, 1, 2, 4, or 8 µg/mL of colistin. The bacterial isolate was sub-cultured from each tube after MIC measurement and further identified as Acinetobacter nosocomialis belonging to ACB. The isolates identified from the 0.5–1 µg/mL colistin tubes were susceptible to colistin, whereas those from the 2–8 µg/mL colistin tubes were resistant (data not shown).
DISCUSSION
The main objective of our study was to optimize MHA for improved colistin diffusion. We first modified the agar concentration, and optimized the medium composition with protamine (Fig. 1). When protamine was added to MHA30, colistin diffusion further increased, resulting in larger inhibition zones and a clear distinction between resistant and susceptible strains (Fig. 1). The addition of protamine to MHA30 resulted in the same sensitivity and specificity, but facilitated the interpretation of the results because the differences in inhibition zone diameters around the colistin disks on MHA30P100 were increased (Fig. 1, Table 1, and Table 3). Although protamine has bacterial growth inhibition properties [24], bacterial growth was not inhibited at 100 µg/mL, while colistin diffusion increased; therefore, this concentration was used in further experiments as an optimal concentration [12].
Three ACB strains were resistant in BMD tests using polystyrene plates, but susceptible in disk diffusion tests using MHA30 and MHA30 P100. When BMD tests for these three strains were repeated using glass tubes, two strains were susceptible to colistin in line with the disk diffusion test results. However, one strain was resistant. To find the reason, the bacterial isolate was sub-cultured from each tube after MIC measurement. Interestingly, the isolates identified from the 0.5–1 µg/mL colistin tubes were susceptible, whereas those from the 2–8 µg/mL colistin tubes were resistant (data not shown). These findings implicated that A. nosocomialis can mutate in vitro after exposure to colistin in BMD, depending on the colistin concentration.
Colistin diffusion improved in MHA30P100 and therefore, this medium can be a useful tool for detecting colistin resistance. This simple medium was easy to prepare and allowed identifying colistin-resistant isolates of both P. aeruginosa and ACB with 94.7% and 100% specificity, respectively. No very major or major error were detected in P. aeruginosa as demonstrated by the 100% agreement between the MICs and inhibition zone diameters on MHA30P100 (Table 1).
A limitation of MHA30P100 is that it is softer than commercial MHA. Therefore, it needs to be handled with caution to avoid scratches or crumpling. Some strains of P. aeruginosa became more mucoid when grown on 30% agar (data not shown), and mucoid colonies preferentially receded to the inhibition zone. In this case, a reduced incubation time of 12 hours could have resulted in clear inhibition zones around colistin disks. Further evaluation on the effect of incubation time reduction on the performance of this simple disk diffusion test would be required.
In summary, this study demonstrated that reducing the agar concentration to 30% of the concentration in commercial MHA dramatically improved colistin diffusion and resulted in reliable colistin susceptibility testing. This modified MHA is expected to be useful in clinical microbiology laboratories for colistin susceptibility testing.


 XML Download
XML Download