

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Though the use of bisphosphonate (BP) to inhibit bony resorption and other antiresorptive or antiangiogenic agents during dental procedures is widespread, it can induce medication-related osteonecrosis of the jaw (MRONJ)1. MRONJ is most frequently observed following tooth extractions or minor dental surgery2—with the former procedure being one of the most common in the field of dentistry. The mechanism underlying the onset of MRONJ after tooth extraction may involve trauma to the alveolar bone during the procedure as well as complications arising during recovery345.
Preventive dental treatment should be conducted to preclude the need for invasive dental treatment and BP therapy6. Previous research has attempted to devise preventative methods that can be used during dental procedures and BP therapy to reduce the incidence of MRONJ7. A BP drug holiday prior to invasive dental treatment was also suggested as a means of reducing the serum level of free BP and decreasing the incidence of MRONJ89. However, the incidence of MRONJ after tooth extraction is relatively low among patients exposed to oral BPs1011, and a short-term drug holiday may not effectively decrease the incidence of MRONJ after tooth extraction1213.
A complete protocol has not been developed for the discontinuation of BP treatment before tooth extraction9. Whether the long-term discontinuation of BP treatment before tooth extraction affects the risk of developing MRONJ after the extraction or whether systemic side effects occur as the result of the long-term drug holiday remains unclear12131415.
The present study assessed the incidence of MRONJ in patients who underwent tooth extraction, had not discontinued BP therapy prior to the procedure, and were determined to not have MRONJ at the extraction site prior to surgery.
Go to : 
II. Materials and Methods
In the present non-randomized, single-center, retrospective cohort study, we analyzed the medical records of patients who were treated with BP and underwent tooth extraction between March 1, 2008 and December 31, 2017. Records that lacked information concerning the medication regimen and its duration, even if they were reported by the patient, were excluded from the study. Only cases in which BP was formally prescribed by our hospital and we could access complete prescription records were included. All the patients included in the study received BP medication prior to tooth extraction. None of the patients had undergone radiation therapy. Patients whose preoperative symptoms indicated the presence of MRONJ as defined by the American Association of Oral and Maxillofacial Surgeons guidelines were excluded9. The study also excluded patients with an unclear diagnosis of MRONJ before tooth extraction who exhibited osteonecrosis during the procedure.
Tooth extraction was performed under local anesthesia. Procedures consisted of the simple removal of the maxillary or mandibular teeth, surgical extractions requiring curettage, and surgical extractions requiring bone removal and root separation. After the extraction procedures, filling material (i.e., bone graft material such as collagen or fibrin) was not applied to the extraction socket. All the patients received oral prophylactic antibiotics 1 hour before the procedure. Patients exhibiting postoperative symptoms indicative of MRONJ were assumed to have developed the condition after the extractions.
All the patients were categorized into one of two groups: BP-continuation (BPC) and BP-discontinuation (BPDC). In the BPC group, all the patients were prescribed BP medication before and up until the tooth extraction procedure. Patients in the BPDC group had received BP medication but discontinued the BP therapy prior to the tooth extraction procedure. The reasons for BP discontinuation were not clearly defined in the medical records. Descriptive statistics were used to determine the effectiveness of discontinuing BP prior to tooth extraction. Patients who took BP for more than 3 years were analyzed separately. All statistical analyses were performed in IBM SPSS Statistics (ver. 23; IBM, Armonk, NY, USA). Significance was set at P≤0.05. Differences in age and the duration of BP medication were compared by t-tests. Differences in the incidence of MRONJ after tooth extraction, sex, number of extracted teeth according to the maxilla/mandible and anterior/posterior lesions, and extraction method were compared between the two groups using chi-squared tests.
Go to :
III. Results
The medical records of 465 patients (420 females) for a total of 1,323 extracted teeth were assessed. The mean ages of the male (±standard deviation [SD], 63.7±10.5 years) and female (69.3±8.8 years) were significantly different (P<0.001). The BPC and BPDC groups included 179 and 286 patients, respectively. The mean age of the BPC group (70.3±9.2 years) was significantly higher than that of the BPDC group (67.8±8.9 years; P=0.003).
With regards to the period of BP discontinuity, the patients in the BPDC group did not receive BP therapy during 39.0±35.5 months (mean±SD) prior to tooth extraction.(Table 1) Concerning the method of BP administration, 149 patients in the BPC group received oral BP, while 260 patients in the BPDC group received oral alendronate sodium (P=0.040). Fifteen patients in both groups received alendronate and intravenous (IV) injections of ibandronate. The mean duration of the medication regimen was significantly different (P<0.001) in the BPC (40.0±35.6 months) and BPDC (14.0±16.8 months) groups. Fifteen patients in the BPC and BPDC groups received IV injections of ibandronate for 23.0±18.7 months and 13.4±18.6 months, respectively (P=0.171).
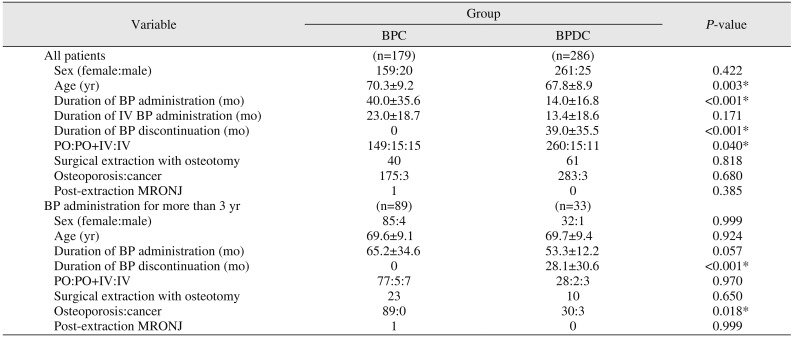
Table 1
Characteristics and incidence of post-extraction MRONJ according to BP discontinuation (n=465 patients)
![]()
In the BPC and BPDC groups, 89 and 33 patients, respectively, received BP therapy for more than 3 years. The mean ages of the patients in these groups (BPC, 69.6±9.1 years; BPDC, 69.7±9.4 years) were not significantly different (P=0.924). Patients in the BPDC group did not receive BP therapy during the 28.1±30.6 months prior to tooth extraction. The BP-administration method did not differ significantly between the 77 patients in the BPC group who received oral BP and the 28 patients in the BPDC group who received oral alendronate sodium (P=0.970). The mean duration of the medication regimen did not significantly differ (P=0.057) between the patients in the BPC and BPDC groups (65.2±34.6 months and 53.3±12.2 months, respectively).
The number of teeth extracted from the 179 patients in the BPC group totaled 537 (306 and 231 from the maxilla and mandible, respectively). Overall, the extracted teeth were composed of 125 incisors, 180 canines and premolars, and 232 molars. Of the 179 patients, 40 underwent surgical extractions accompanied by alveolar bone removal.
The number of teeth extracted from the 286 patients in the BPDC group was 786 (434 and 352 from the maxilla and mandible, respectively). Overall, the extracted teeth were composed of 173 incisors, 279 canines and premolars, and 334 molars. Of the 286 patients, 61 underwent surgical extractions accompanied by alveolar bone removal.
The BPC and BPDC groups included 175 and 283 patients, respectively, who received BP therapy for the treatment of osteoporosis. In both groups, three patients with cancer received IV injections of ibandronate.
Of the 465 patients included in the study, only one patient in the BPC group developed MRONJ after tooth extraction, while none of the patients in the BPDC group developed MRONJ. The incidence of MRONJ was not significantly different between the two groups (P=0.385).
The patient with MRONJ was a 79-year-old woman with a history of hypertension, but not diabetes, who had received IV injections of ibandronate for 50 months. She had undergone left mandibular second premolar extractions twice to remove remaining dental roots in the same area at the local dental clinic before being admitted to our hospital with a residual root at the site of the extracted tooth. After surgical extraction of the residual root, the patient developed MRONJ. The patient subsequently underwent maxillary incisor and premolar extractions to remove a torus on the lingual side of the left mandible without developing MRONJ.
Go to :
IV. Discussion
In the present study, only 1 patient from among the cohort of 465 patients developed MRONJ after tooth extraction. This patient received ibandronate for over 4 years and had already undergone two extraction procedures before visiting our hospital. Therefore, the trauma of having undergone three extraction procedures for the complete removal of the root at the same site may account for her development of MRONJ. This case indicates that although tooth extractions may increase the risk of MRONJ onset, careful tooth extractions will minimize the incidence of post-extraction MRONJ.
The one patient with post-extraction MRONJ was part of the group of 179 patients who underwent tooth extractions without discontinuing BP therapy, as well as a subgroup of 122 patients (89 of whom did not discontinue BP medication before tooth extraction) who received BP therapy for more than 3 years. Enforcing BP drug holidays for all patients before tooth extractions should be carefully considered.
It has been reported that BPs may been retained in the bone due to their extended half-life. Therefore, the discontinuation of BP therapy for several months (a drug holiday) will have little effect on the BPs already incorporated into the bone in cases of tooth extraction procedures16. A previous study recommended that necessary tooth extractions should be completed before starting BP therapy and that tooth extraction procedures during BP therapy should be avoided17. However, excessive delays in extracting an inflamed tooth may increase the risk of MRONJ, so tooth extractions cannot be completely avoided.
Since no previous study has assessed the incidence of MRONJ following the long-term discontinuation of BP medication prior to extraction procedures, the literature lacks data on extraction socket evaluations to which the results of the present study can be compared. However, a prior report found no evidence of the effect of a short-term oral-BP drug holiday before tooth extraction on reducing the risk of developing MRONJ after tooth extraction and recommended a minimally traumatic extraction technique to lessen the risk of postoperative MRONJ12.
Since our study included a limited number of patients (n=465), additional studies that include more patients from more institutions should be performed to validate our findings concerning the effects of long-term BP discontinuation (>3 months) on the various types of BP therapy according to medication type and period of use. The mean age of the BPC group was significantly higher than the BPDC group. This means that the compared study group was not homogeneous. The current study is a retrospective study which has incomplete medical records for BP therapy. Therefore, a prospective study with clear BP therapy medical records will be helpful for defining the BP drug holiday for dental procedures including tooth extractions.
This study is valuable for the evaluation of the extraction area. Among the patients who were excluded from this study, one patient was diagnosed with MRONJ at the time of tooth extraction. Despite not being diagnosed with MRONJ before the extraction, this patient exhibited a necrotic alveolar bone lesion in the extraction socket at the time of extraction.(Fig. 1) Histopathological results indicated that the lesion was necrotic alveolar bone, suggesting that the patient had already developed MRONJ prior to the tooth extraction procedure.
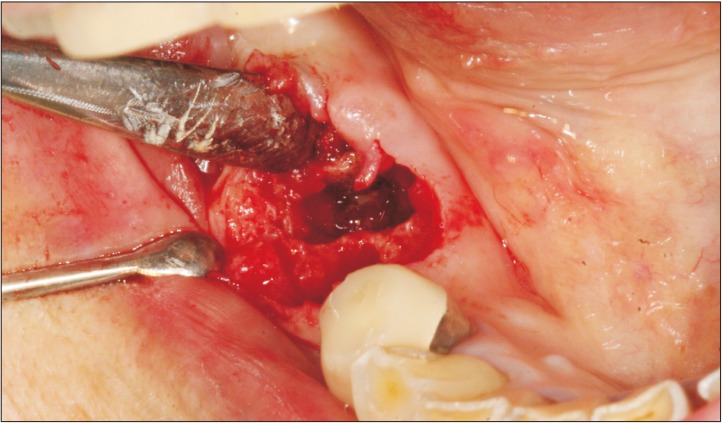
However, we confused the staging of this case. No clinical evidence, including radiographic support, for necrotic bone was found before the tooth extraction. During the extraction procedure, the necrotic bone of the tooth extraction socket was exposed, and the bony exposure did not last longer than 8 weeks9. Therefore, this case may not have been MRONJ. If it was, it would be difficult to determine the stage of the condition. As a result, we suggest a new category of MRONJ with a definition encompassing bony necrosis found in the extraction socket.
A lack of thorough evaluation of the socket at the time of extraction may lead to a misdiagnosis. This may result in false-positive cases of post-extraction MRONJ for cases in which MRONJ had already occurred at the planned extraction area before tooth extraction. Patients diagnosed with post-extraction MRONJ do not always receive a clear preoperative diagnostic evaluation at the time of extraction. Therefore, previous studies suggesting that tooth extraction procedures induce a high rate of post-extraction MRONJ should be assessed carefully to ensure that pre-extraction evaluations of the patients were adequately performed.
Furthermore, it should be reconsidered whether tooth extraction procedures constitute a major risk factor in the development of MRONJ. Future studies with a thorough assessment of whether MRONJ already presents at the planned tooth extraction site are warranted. Understanding the indications of tooth extraction before procedures are performed is essential. Not only should the possible onset of MRONJ before the extraction procedure be considered carefully, but surgeons must also be prepared to treat the possible onset of MRONJ during the extraction procedure because of the possibility of pre-existing MRONJ in the extraction socket area.
Clinicians should consider the following contents for tooth extractions associated with BP therapy. Preventive dental treatment should be conducted to preclude the need for invasive dental treatment and BP therapy6. The incidence of MRONJ after tooth extraction is relatively low among patients exposed to oral BPs1011, and a short-term drug holiday may not effectively decrease the incidence of MRONJ after tooth extraction1213. In addition, excessive delays in extracting an inflamed tooth may increase the risk of MRONJ, so tooth extractions cannot be completely avoided. The treatment of pre-existing MRONJ in the extraction socket area must be always prepared for tooth extraction-associated BP therapy. Finally, in the tooth extractions associated with BP, a risk evaluation is essential, a proposed algorithm is helpful, and informed consent is necessary18.
Go to :
V. Conclusion
The findings of the present study suggest that the accurate diagnosis of MRONJ at the time of extraction is crucial, and that an additional category of MRONJ that encompasses cases of bony necrosis found in the extraction socket during tooth extraction procedures is needed. Our study further indicates that the routine discontinuation of BP medication several months prior to the extraction procedure should be considered carefully.
Lastly, it is difficult to confirm that tooth extractions in patients treated with BP medications for extended periods of time increases their risk of MRONJ. Despite the limitations of our study, we conclude that discontinuing BP medication regimens before tooth extraction is not recommended to reduce the risk of post-extraction MRONJ.
Go to :
 XML Download
XML Download