

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Osteogenesis imperfecta (OI), also known as brittle bone disease, is a heterogeneous group of connective tissue diseases that is predominantly characterized by bone fragility and skeletal deformity1. Most cases of OI are associated with autosomal dominant mutations in the two type I collagen genes (COL1A1 on chromosome 17 and COL1A2 on chromosome 7)234. Collagen is the most abundant protein in the body and comprises the connective tissue in cartilage, bone, and blood vessels. In addition, there are 19 types of collagen, and type I collagen, the most common, provides mechanical strength5.
OI has a birth prevalence of approximately 1:20,000. However, a significant number of patients are undiagnosed, possibly due to lack of awareness, absence of severe symptoms, or other reasons.
Sillence et al.1 classified OI based on clinical presentation and pattern of inheritance into types I to IV, and the classification system is the most widely used.(Table 1) Patients with the typically-milder type I (mild) and IV (mild-to-moderate) present with bone fragility and, at times, dentinogenesis imperfecta and some hearing loss. In type I, the sclera is usually blue and/or stature is normal, but in type IV, the sclera is normal while stature is variably short. Types II (lethal, perinatal type) and III (progressively deforming type) are more severe and often associated with extreme bone fragility. Perinatal death with under-mineralized skull and micromelic bone is frequent in type II, whereas in type III, patients have moderate deformity of the limbs at birth and, oftentimes, very short stature and dentinogenesis imperfecta1.
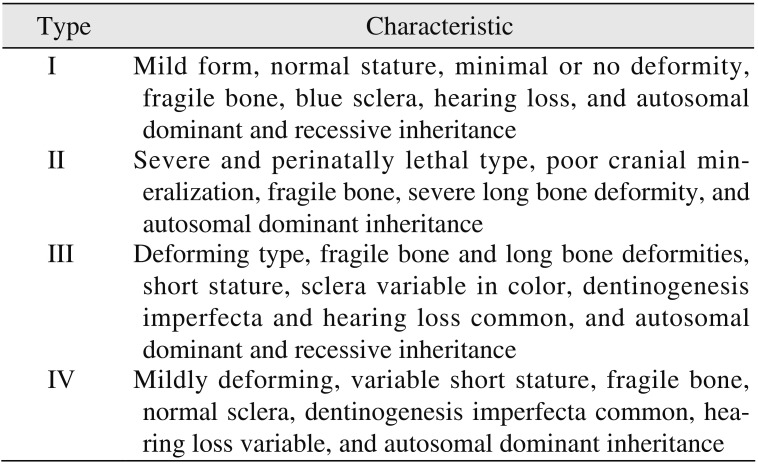
Table 1
Sillence's classification of osteogenesis imperfecta
![]()
Like other organs containing type I collagen, the cranial bones are also affected by OI. Many studies have reported that the intermaxillary relationship in patients with OI has a Class III tendency with a posterior open bite and an anterior posterior crossbite678910. An abnormal jaw relationship was especially found in patients with types III and IV OI. On the other hand, some studies have reported that patients with type I OI do not show a severe abnormality of the intermaxillary relationship, although the size of the facial bones is smaller than normal linear measurements10.
Few cases of orthognathic surgery in patients with OI have been reported, but most describe successful operations5111213. In this report, we present two patients (siblings) with type I OI. During the course of treatment for the younger sister, the disease was not recognized until abnormal extensive ecchymosis occurred in the early postoperative period. Because we detected OI during the first operation for the younger sister, we were able to carefully prepare for the older sibling's operation.
Go to : 
II. Cases Report
1. Case 1
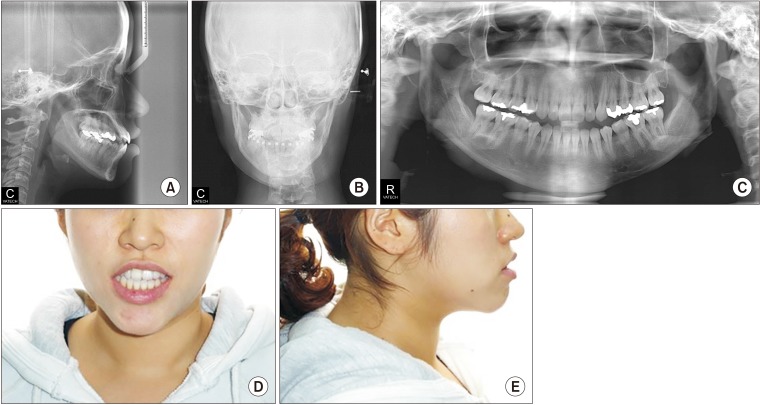
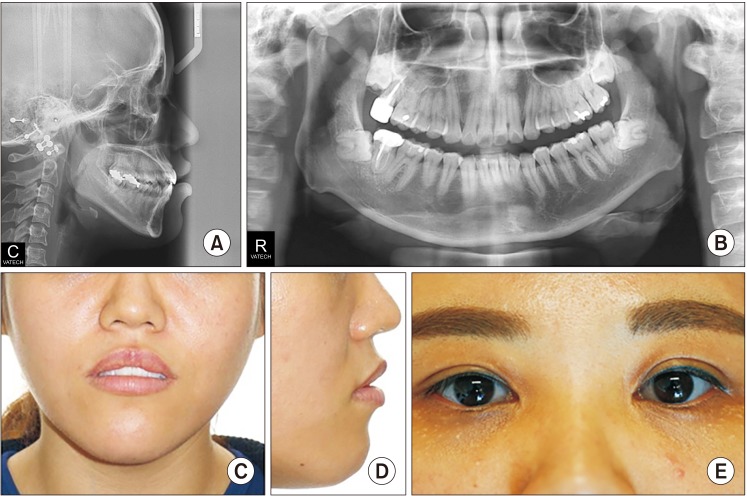
A 31-year-old female patient was referred by her orthodontist to Asan Medical Center in Seoul, Korea for treatment of facial asymmetry and prognathism. The patient had never been diagnosed with a medical problem and had no previous history of fracture. Clinical examination revealed that the patient was slightly short in height (153.4 cm) and moderately overweight (62.4 kg, body mass index [BMI] 26.52 kg/m2). Examination of her facial features revealed a long lower face with vertical maxillary excess and mandibular asymmetry with occlusal canting of the maxilla. In addition, she had upper lip protrusion and lip incompetence.(Fig. 1, 2) The intraoral findings included Class III malocclusion with an open bite. She had normal tooth structure and received proper dental care. Therefore, her periodontal health and oral hygiene were good.

After the initial interview, the patient was referred to an orthodontist for leveling and alignment of the teeth, and treatment continued for approximately one year. After the presurgical orthodontic treatment, a clinical evaluation was repeated, and cephalometric radiographs and face bow recordings were obtained for final surgical planning 4 weeks prior to the surgery.
In addition, a work-up for general anesthesia and surgery was performed, and the preoperative hematologic examination, electrocardiogram and chest radiograph were unremarkable.
The surgery included bimaxillary procedures. Le Fort I osteotomy with midline correction, canting correction, posterior impaction, and setback movement of the maxilla were performed via rigid skeletal fixation. Bilateral sagittal split ramus osteotomies were performed with a setback movement via the hybrid fixation technique (with one miniplate and one additional bicortical screw). On the left side, a greenstick fracture occurred in the proximal segment. However, we could appropriately position the proximal and distal segments as planned, and so two additional bicortical screws were used to fix the fractured proximal segment. Two closed suction drains were inserted into the mandibular surgical site. The operation was completed without major bleeding, and the estimated blood loss during the surgery was 200 mL.
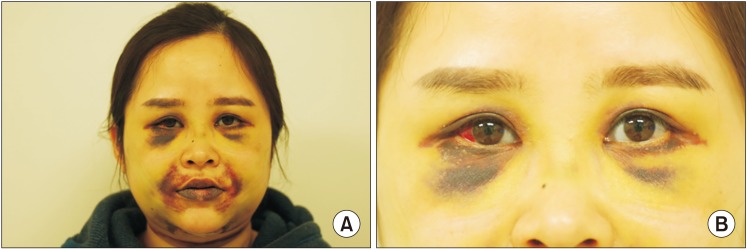
Abnormal edema and ecchymosis were observed from the second postoperative day.(Fig. 3) At first, an improperly functioning closed suction drain was suspected, but the ecchymosis and edema appeared to be bilateral, decreasing the likelihood of drain malfunction. On the second postoperative day, drain removal and maxilla-mandibular fixation (MMF) with elastic ring were routinely performed. Normally, an orthognathic surgical patient is hospitalized for 2 nights and 3 days after surgery, but in this case, the discharge was delayed due to the appearance of abnormal ecchymosis and edema. On the fifth postoperative day, nasal bleeding and transient blood pressure lowering were noted, but the problems resolved after nasal packing and administration of intravenous fluids. At 6 days postoperatively, the patient was stable, and she was discharged from the hospital.
MMF was routinely stopped 2 weeks after surgery, and training elastics were applied. No other complications were observed. However, the ecchymosis persisted for 6 weeks, and although it dissipated slowly and spontaneously, no specific treatment was needed for its resolution. The follow-up examination at postoperative 3 months showed uneventful healing.
During the search for the cause of unexpected postoperative bleeding, she recounted multiple fractures of the lower limbs during childhood, and blue sclera was noticed. Furthermore, her familial history included multiple bone fractures in her mother, grandmother, and cousin. Therefore, OI type I was suspected, and it was inferred that the patient's complications were ultimately caused by bleeding due to vessel fragility from OI.
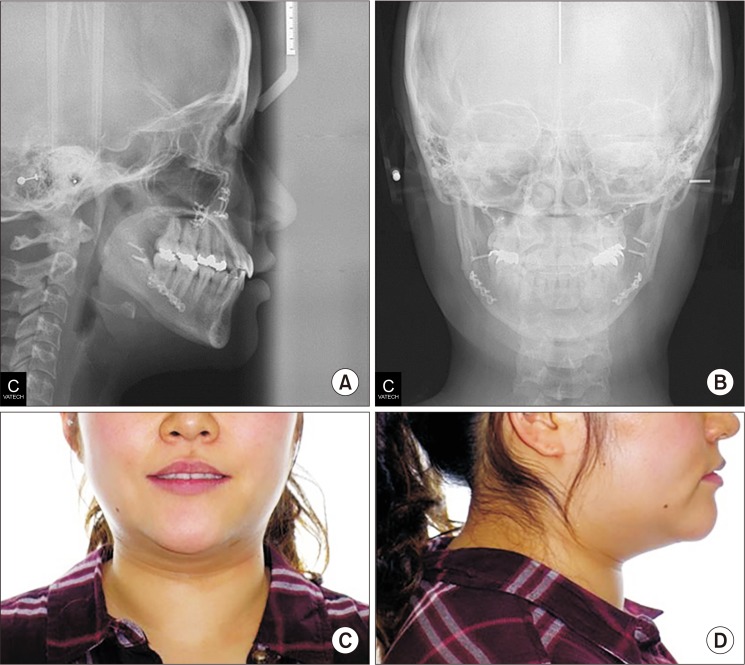
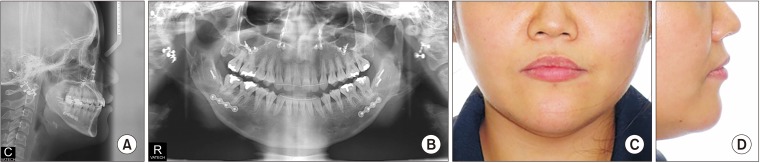
The postsurgical orthodontic treatment began one month after surgery. The molar and canine relation became Class I, and the open bite was greatly improved. After approximately eight months, debonding was done. The long lower face with vertical maxillary excess and mandibular asymmetry with occlusal canting of the maxilla were greatly improved. The upper lip protrusion and lip incompetence were also improved.(Fig. 4, 5)

2. Case 2
A 33-year-old female patient was referred by her orthodontist to Asan Medical Center in Seoul, Korea for the treatment of facial asymmetry and chin protrusion. She was the older sister of the patient from Case 1, and she appeared similar to her younger sister.
The patient also had never been previously diagnosed with a medical problem, but she did have a history of surgery for a left leg bone fracture in her teenage years. The general examination revealed that the patient was slightly short in height (155.0 cm) and slightly overweight (52.8 kg, BMI 21.98 kg/m2), similar to her younger sister.
As for her facial features, the patient had a facial appearance similar to her sister's, and she had the following similar problems. She had a long lower face with vertical maxillary excess and mandibular asymmetry with occlusal canting and yawing of the maxilla. Upper lip protrusion and chin protrusion were also apparent.(Fig. 6, 7) Intraoral findings included Class III malocclusion with a shallow overbite. Likewise, she had normal teeth structure, and she also had good periodontal health and oral hygiene due to proper dental care.

She was referred to the same orthodontist as her sister for one year of orthodontic treatment before surgery. After the presurgical orthodontic treatment, the clinical evaluation was repeated, and cephalometric radiographs and face bow recordings were obtained for final surgical planning 4 weeks prior to the surgery.
In addition, a work-up for general anesthesia and surgery were performed, and all results were normal. However, during the patient's surgical preparation, OI was critically considered due to her family history and her younger sister's operative complications.
The possibility of hemorrhage due to OI was explained to the patient prior to surgery. Furthermore, we noted that the operation could be stopped and changed to a two-step procedure if massive bleeding occurred during surgery.
The surgical plan was similar to that of the patient from Case 1 as the sisters had similar craniofacial relationships. The surgery included bimaxillary procedures. Le Fort I osteotomy with midline correction, canting correction, posterior impaction, and setback movement of the maxilla were performed using rigid skeletal fixation. Bilateral sagittal split ramus osteotomies were performed with a setback movement using the hybrid fixation technique (one miniplate and one additional bicortical screw). On the left side, a greenstick fracture occurred in the proximal segment, as in the younger sister's case, but we could appropriately position the proximal and distal segments as planned, and so two additional bicortical screws were used to fix the fractured proximal segment. Two closed suction drains were inserted into the mandibular surgical site. The operation was completed without major bleeding, and the blood loss during the surgery was estimated to 200 mL.
The patient's recovery process proceeded routinely, and there was no remarkable finding. Daily dressing was done, and on the second postoperative day, drain removal and MMF with elastic ring were performed. On the third postoperative day, the patient was discharged without any abnormal complications.
MMF was stopped 2 weeks after surgery, and training elastics were applied. No other complications were observed. The follow-up examination at postoperative 6 months showed uneventful healing.
The postsurgical orthodontic treatment began one month after surgery. After Class I molar, canine relationship, normal overbite and overjet were achieved, debonding was done. The patient's long lower face with vertical maxillary excess and mandibular asymmetry with occlusal canting and yawing of the maxilla were greatly improved. Upper lip protrusion and chin protrusion were also improved.(Fig. 8, 9) No specific problems during orthodontic treatment were encountered.

Go to :
III. Discussion
A significant number of patients with OI remain undiagnosed. Initially, we did not consider the existence of an underlying medical problem in the present cases. However, after orthognathic surgery for the first patient (younger sister), we speculated the cause of abnormal bleeding. Thereafter, we confirmed the diagnosis of OI type I in both cases based on the typical clinical features of OI, such as multiple bone fracture history, short stature, blue sclera, the bleeding episode during the younger sister's orthognathic surgery and familial history; we did not base the diagnosis on laboratory findings.
Most orthognathic surgeries for patients with OI have reported acceptable outcomes. The risk of perioperative bleeding in patients with OI should be very carefully considered, and some authors reported patients with OI and severe bleeding during or after orthognathic surgery141516. The patient in the first case showed abnormal edema and ecchymosis after surgery, despite normal blood test results. This appears to be due to vessel fragility in patients with OI and has been reported previously17. A Rosén et al.5 reported that orthognathic surgery in patients with OI had been considered as a two-step procedure in cases of severe bleeding. In our cases, this method was considered for the second patient after the unfavorable recovery of the first patient. Fortunately, there was no abnormal bleeding in the second case, and bimaxillary surgery was executed as initially planned.
Several authors reported poor bone quality in patients with OI512. Moreover, Tashima et al.12 reported that he changed his plan and would only perform mandibular orthognathic surgery in cases that need bimaxillary orthognathic surgery, and he suggested prolonged intermaxillary fixation to facilitate bone union due to poor bone quality in a patient with OI. In our cases, the patients' bone quality was somewhat poor, but fortunately, internal fixation was possible. Many authors reported normal bone healing patterns after orthognathic surgery in patients with OI, and similarly, normal recovery patterns were observed in our cases.
Many cases of successful orthodontic treatment have been reported in patients with OI, some of whom additionally had dentinogenesis imperfecta5111218. As with bone healing and remodeling after orthognathic surgery, the process following orthodontic treatment was considered successful. One consideration, however, is that some patients with OI may have been using bisphosphonates to reduce fractures1920. Therefore, if patients with OI require tooth extraction for orthodontic treatment and orthognathic surgery, clinicians should consider medication-related osteonecrosis of the jaw (MRONJ) and investigate the history of bisphosphonate drug treatment.
In conclusion, for patients with OI, an abnormal healing process may occur after surgery due to vessel fragility. Furthermore, other various abnormal complications may occur. Therefore, cases involving patients with OI should be carefully evaluated in many respects prior to the actual surgery.
Go to :
 XML Download
XML Download