

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
One of the most common complications after bilateral sagittal split ramus osteotomy (BSSRO) is neurosensory impairment of the inferior alveolar nerve (IAN) following injury to the nerve bundle during surgery. Such injuries may occur due to the variable anatomy of the inferior alveolar canal and buccolingual and its vertical orientation123. This is an important concern in mandibular osteotomy, since patients may experience variable degrees of neurosensory dysfunction for long periods of time; in some cases, dysfunction is permanent1. The incidence of IAN dysfunction is reported to range between 13%–100% immediately after surgery to 0%–85% after one year4. Surgeons aim to decrease the incidence of IAN dysfunction by improving surgical techniques and performing preoperative imaging such as panoramic views to avoid nerve bundling. However, if they fail, injury to the nerve can lead to complications such as drooling, lip biting, and thermal injury as well as patient dissatisfaction3567.
Therefore, preoperative radiographic examinations are of significant clinical value8. Although panoramic and lateral cephalography is the main method used, it is limited by inconsistencies in magnification of different parts of the image and its inability to exhibit all three-dimensions891011. On the other hand, cone-beam computed tomography (CBCT) can illustrate buccolingual depth without distortion and seems excellent for localizing the inferior alveolar canal (IAC) and adjacent structures810121314. Therefore, accurately determining the position of the IAN canal within the mandible with CBCT before surgery may reduce IAN dysfunction after BSSRO. Despite its clinical relevance, the impact of CBCT combined with routine imaging compared to routine imaging alone on post-surgical sensory disturbances has been examined in only one preliminary study2. Therefore, the purpose of this study was to evaluate the effects of preoperative imaging of the IAN canal using CBCT with routine imaging versus routine imaging alone (panoramic and lateral cephalography) on sensory disturbances perceived during the first year after surgery. The null hypotheses were that there would be no differences between groups, between sexes, between left and right sides, over time, or across ages.
Go to : 
II. Materials and Methods
This parallel randomized clinical trial comprised 43 patients (30 females and 13 males) with skeletal class III deformity needing mandibular setback surgery with or without simultaneous maxillary surgery who were treated at Buali Hospital in Tehran, Iran during 2014 to 2016. We included patients who were candidates for BSSRO due to mandibular setback less than 7 mm and excluded patients who had jaw asymmetry, pathologic conditions of the IAN, previous surgery in that region, any neurosensory dysfunction of the IAN, required genioplasty, and had medical conditions with associated neuropathy before surgery. We also excluded patients who were randomly assigned to the CBCT group but who did not consent to undergo CBCT imaging, although they received routine treatment. The protocol ethics were approved by the Islamic Azad University's Board of Ethics and Research according to the Helsinki declaration (No. 08-21-214), and informed consent was obtained from each patient. The trial was reviewed by and approved/registered at an international institute before beginning the study (RCT code: IRCT2014052217798N1).
1. Randomization
The patients were randomized sequentially to either the control or experimental group based on order of treatment at the clinic (the first patient being randomly assigned to the experimental group). Patients with odd and even numbers were assigned to the experimental and control groups, respectively. Since the order of patients was random and not previously known, this systematic sampling was considered random. The surgeon and patients were not blinded to grouping, but the operator who collected the information was blinded. However, the study is not considered a blind study.
2. Intervention
Plain radiographs, including panoramic radiographs and lateral cephalographs, were performed for all patients in both groups. In the experimental group, we performed CBCT (Newtom VG-Quantitative Radiology, Verona, Italy) from both sides of the ramus and mandibular body through the region of the second molar with 2 mm interval cuts. The distance between the mandibular foramen and sigmoid notch was measured. The distance between the cortical border of the IAN canal and the lateral cortex of the mandible, the thickness of the lateral cortex of the mandible, and the distance between the canal and inferior border of the mandible in the region of the second molar were measured and documented on the CBCT. The regions of the canal near the cortex were documented to avoid nerve bundle injury in these regions.(Fig. 1)
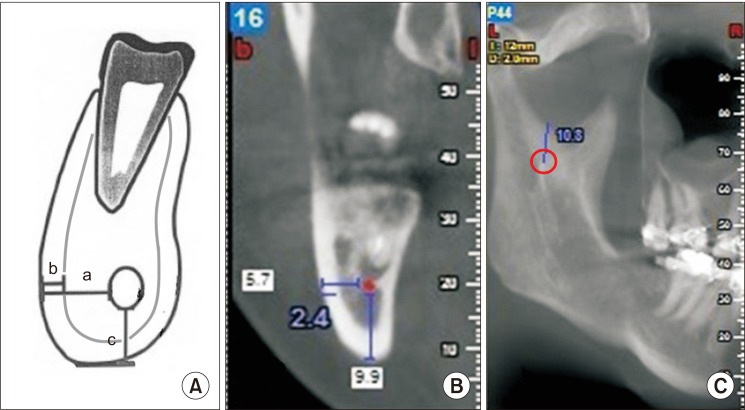 | Fig. 1A. Schematic view of the mandibular body. a: distance between inferior alveolar nerve (IAN) canal and buccal cortex of the mandible, b: thickness of the buccal cortex, c: distance between IAN canal in inferior border. B. Measurements of cone-beam computed tomography. C. Distance between the mandibular foramen (at the center of the red circle) and sigmoid notch. The mandibular foramen was located on images as the starting point of the mandibular canal.
|
3. Surgical procedure
All surgeries were performed by one right-handed, experienced surgeon. The surgical method applied for all patients was BSSRO with the Obwegeser–Dal Pont technique and Hunsuck modification15. After incision and during dissection of the medial side of the ramus, attention was paid to the site of the mandibular foramen. After identification of the sigmoid notch, the site of horizontal osteotomy of the medial was determined half-way between the sigmoid notch and mandibular foramen. The medial soft tissues were retracted, and the osteotomy was performed with a Lindemann bur. Vertical osteotomy of the buccal cortex was performed in the region of the second molar to the medullary bone, and crestal osteotomy of the anterior border of the ramus was completed to connect the lingual and buccal osteotomies. Bone splitting was achieved with a chisel in close contact to the inner side of the buccal cortex as it advanced forward. Splitting of cortices was accompanied by searching for and preserving the neurovascular bundle. After splitting, any irregularity in the interior surface of the two proximal and distal segments was removed by a round bur. After mobilization, the distal segment was repositioned in occlusion, and a maxillomandibular fixation wire was placed. The proximal segment was repositioned to correct the relationship with the glenoid fossa; in 62 hemimandibles, rigid fixation was achieved with two bicortical screws while paying attention to protect the neuromuscular bundle from injury during screw placement. In 18 hemimandibles, this procedure was performed using one screw. In two hemimandibles, there was no fixation; in two others, three screws were installed, and plates were used for fixation in two others. Dexamethasone 8 mg was injected in all patients before surgery and every 8 hours after surgery for two days, with the dose tapered to 4 mg every 12 hours on the third day after surgery and discontinued the day after that.
When the surgeon predicted IAN damage based on CBCT, the following precautions were taken during surgery. The patient was notified that the risk of IAN damage is high, and that there might be neurosensory disturbances after the surgery. In some cases, it was necessary to change the location of the vertical cut. In areas where the nerve was very close to the lateral cortex, fine osteotomes and splitting methods were used to bypass the danger zone. The exact top-bottom location of the nerve at the lateral side of the mandibular trunk was determined, and in cases of proximity to the lateral cortex, the depth of bone removal was reduced.
4. Neurosensory evaluation
Neurosensory functional evaluation of IAN was determined subjectively using a 5-point Likert scale questionnaire following Westermark et al.16. The patients were asked to rate the numbness of the right and left sides of the lip and chin areas. On this scale, scores of 1 to 5 were indicative of complete numbness, almost near numbness, some sensation, almost near normal sensation, and normal sensation, respectively. This questionnaire was administered preoperatively and 7 days, 1 month, 3 months, 6 months, and 12 months post-surgery. All preoperative sensory measurements indicated health in all patients (i.e., all scores were 5).
5. Statistical analysis
The sample size was pre-determined based on a 6-month pilot study of 10 patients. We determined that 40×2 patients were necessary to obtain a test power greater than 80%. The pilot sample was not included in the study.
Descriptive statistics and 95% confidence interval were calculated for all measurements. The extents of mandibular setback were compared between the two groups using an independent-samples t-test. Groups were compared in terms of sex and age using Fisher's exact test and independent-samples t-test, respectively. The Spearman correlation coefficient was used to evaluate correlations between neurosensory scores on left and right sides and between neurosensory scores and extent of mandibular setback. Independent-samples t-tests were used to compare neurosensory function of control and cohort groups for each of the 5 time points. A paired t-test was used to compare the neurosensory function of left versus right sides at each time point.
The whole dataset was analyzed once using a mixed-effects linear model, discarding the effect of time. Then, the data were divided into two datasets pertaining to the left and right sides, and each side was analyzed separately using repeated-measures ANCOVA while accounting for the effect of time but discarding the right/left sides.
A mixed-effects linear model was used to assess the effects of jaw side (left or right), the intervention, displacement extent, and patient age on overall neurosensory function. In each of the left or right subgroups, repeated-measures ANCOVA was used to analyze the effects of time, setback extent, and radiography method (control/experimental) as the intervention on neurosensory function. We conducted analyses using IBM SPSS Statistics (ver. 23; IBM, Armonk, NY, USA). The level of significance was set at 0.05 for all tests, except the two t-tests used for comparisons of neurosensory scores between groups and sides at each time point. For these tests, significant was adjusted to 0.01 using the Bonferroni method.
Go to :
III. Results
This study was composed of 43 patients (86 sides) who were randomized into an experimental group of 21 patients (42 sides) (14 females and 7 males, with a mean and standard deviation age of 26.1±4.5 years) and a control group of 22 patients (44 sides) (16 females and 6 males, with a mean age of 25.4±2.7 years; range, 18-33 years). Mean mandibular setback extent was 4.00±1.45 mm and 4.59±0.91 mm (range, 1–7 mm) in the experimental and control groups, respectively. There was no significant difference between groups according to sex (Fisher exact test, P=0.747), age (unpaired t-test, P=0.492), or amount of movement (unpaired t-test, P=0.115). No adverse effects were identified.
There were significant differences between the control and experimental neurosensory scores measured 1 month and 6 months after surgery.(Table 1) There were significant differences between the right and left sides during the first, fourth, and last intervals.(Table 2)
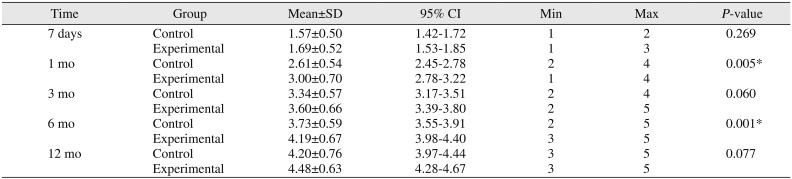
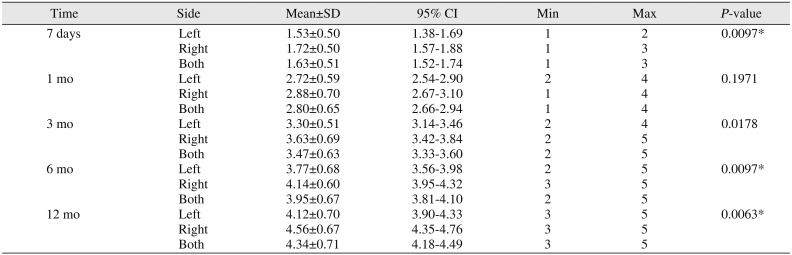
Table 1
Descriptive statistics for control and treatment groups and the results of the independent-samples t-test (α=0.01)
![]()
Table 2
Descriptive statistics for left and right sides and the results of the paired t-test (α=0.01)
![]()
Except during the first interval (7 days after surgery, Spearman rho=0.635, P<0.001), there were no significant correlations between neurosensory functions perceived by patients on their left and right sides at the second (rho=0.200, P=0.199), third (rho=−0.058, P=0.710), fourth (rho=0.039, P=0.805), or fifth (rho=−0.129, P=0.409) follow-up visit. The extent of displacement was not associated significantly with sensory function rate on left or right side for any of the five intervals (all rho values ranged between −0.221 and 0.179, all P-values >0.250).
The mixed-effects model (n=86) indicated significant effects for jaw side (P=0.003) and CBCT intervention (P=0.002; Fig. 2) but not age (P=0.617) or displacement extent (P=0.122).
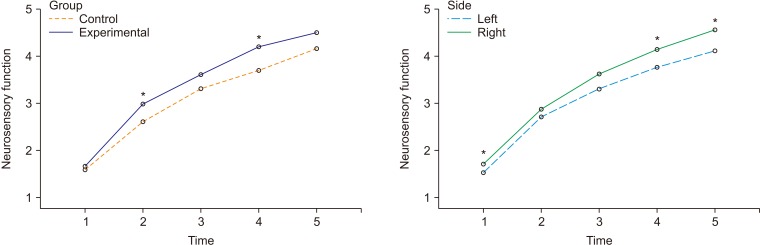 | Fig. 2Marginal means of neurosensory function in the control/experimental groups (left panel) and jaw sides (right panel), estimated at an age of 25.7 years and at a displacement extent of 4.3 mm. The time points 1 to 5 indicate 7 days, 1 month, 3 months, 6 months, and 12 months after surgery, respectively. Significant comparisons (*P<0.01) between control versus experimental groups (left panel) and between left versus right sides (right panel).
|
On the left side (n=43), repeated-measures ANOVA detected significant effects for time (P=0.001) and CBCT intervention (P=0.005). On the right side (n=43), a significant effect was observed for time (P<0.001), while the effect of the intervention was marginally significant (P=0.066). The effect of mandibular displacement was not significant on either side (both P-values >0.280).
Go to :
IV. Discussion
We found that performing BSSRO surgery while taking advantage of CBCT information can aid clinicians seeking to reduce neurosensory deficits more rapidly. Only one previous preliminary study by Aizenbud et al.2 had compared CBCT and routine imaging versus routine imaging alone before BSSRO surgery. In that study, there was a significant difference between two groups in terms of neurosensory function during the first postoperative year, and they observed positive effects of CBCT imaging on postoperative neurosensory function2. However, they did not detect differences between sides2. CBCT allowed the surgeon in the present study to observe data that are not available with panoramic imaging alone, such as the distance of the mandibular foramen from the sigmoid notch on the medial side of the ramus, which allowed for better preservation of the nerve bundle. We also increased the number of patients in our sample for better statistical analysis.
Our findings can be discussed considering more general research. Yamamoto et al.17 evaluated neurosensory disturbances after BSSRO in patients who had undergone preoperative transaxial CT scans of the IAN canal before surgery and evaluated postoperative neurosensory function with two-point discrimination, light touch discrimination, and a thermocryesthesiometer during the first year after surgery. They concluded that neurosensory dysfunction occurred for all cases in which the mandibular canal was in contact with the lateral cortical plate of the mandible, and that a marrow space 0.8 mm or less between the mandibular canal and external cortical bone was more likely to associate with neurosensory disturbance. Two of the most common causes of injury to the IAN during BSSRO are the variable anatomy of the canal and the relationship of the IAN to the external cortex of the mandible1819. Injury to the nerve bundle most commonly occurs during vertical buccal osteotomy, splitting of segments, screw placement or compression by rigid fixation or during dissection, and osteotomy of the medial side of the ramus572021. The IAN canal has a S-shaped course in the ramus and mandibular body. From its entrance to the mandibular foramen, it is close to the lingual cortex; in the region of the third molar, it is most lateral and closest to the buccal cortex; and in the first molar region, it approaches the lingual cortex and finally exits the mental foramen near the premolar region222324. In our study, we obtained CBCT data in the experimental group that allowed us to determine the exact anatomic position of the nerve bundle and secure it from injury during medial dissection, osteotomy, vertical buccal osteotomy, and splitting of segments. This allowed clinicians to minimize neurosensory dysfunction after BSSRO. The reason neurosensory function on the right side improved more rapidly than that on the left side might be due to better access by the surgeon to the right side, resulting in better handling of the tissues and less traction-induced damage. The only other study that has made this comparison found no significant differences between sides2, possibly due to small sample size or greater caution exercised during surgery. Future studies are needed for further evaluation of the effect of side, since it might differ from case to case depending on the dominant hand of the surgeon or other operational habits.
Neurosensory disturbances could be attributed to age4. In this study, we did not observe a link between age and neurosensory dysfunction despite a wide range of ages among our subjects (and age range might matter1), but this may reflect the relative youth of our patients rather than an actual lack of association. We did not find the extent of mandibular displacement to be associated with neurosensory deficits, which might be attributed to the low variations in displacement.
This study was limited by some factors. We did not use objective methods of neurosensory evaluation such as blink reflex, electroneurography, or other neurophysiological techniques in our analysis. It remains unclear whether objective or subjective evaluations are superior. A systematic review showed that the incidence of nerve dysfunction is higher after subjective evaluations than objective ones. After one year of evaluation, objective methods determined an incidence of neurosensory dysfunction of 12.8%, while subjective methods yielded an incidence of 18.4%25. Other studies also showed that subjective evaluations of neurosensory dysfunction were associated with greater frequency of detection of sensory impairment than objective methods52627. One study found that the results of subjective evaluations of neurosensory function were comparable to the results of two-point discrimination28. The most important evaluation factor is patient satisfaction, and good results of aesthetic surgery may be negatively affected by a neurosensory dysfunction. Therefore, we applied subjective evaluations of neurosensory function in the present study. Injury to the IAN can be avoided by applying surgical techniques such as intraoral vertical ramus osteotomy, which yields an incidence of neurosensory dysfunction that is lower than that of BSSRO but has limitations in cases of mandibular deficiencies that require advancement and does not allow rigid fixation that requires a period of maxillomandibular fixation262930. The use of the Lindemann bur might be traumatic, especially when the site of surgery is very close to the nerve31. However, this was a routine protocol and is also a limitation of many other high- and (especially) low-speed rotating instruments. Moreover, since the protocol was standardized for both groups, it could not affect study outcomes. Finally, the method of randomization used in this study was nonstandard, and we did not use more popular methods such as a random number table.
Go to :
V. Conclusion
In this study, we found that CBCT imaging can allow a surgeon to perform more conservative procedures and therefore indirectly contributes to acceleration of improvement in neurosensory functions over a 1-year period after treatment. We also found that neurosensory disturbances following BSSRO were ameliorated faster on the right side, perhaps due to surgical convenience when operating on that side.
Go to :
 XML Download
XML Download