

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anaplastic lymphoma kinase (ALK) is a membrane-associated receptor tyrosine kinase that belongs to insulin receptor superfamily.1 ALK rearrangement is oncogenic, activating cellular signaling pathways by dimerization via the specific structures of fusion partners.2 Genetic alteration in ALK has been identified in various tumors. Recently, the World Health Organization designated ALK rearrangement-associated renal cell carcinoma (ALK-RCC) as a new/emerging renal tumor entity.3 Identifying ALK-RCC is important because ALK inhibitors have been shown to be effective in treating this tumor. Notwithstanding, ALK-RCC is rare, and few studies have described its clinicopathological features.4567 To date, 28 cases of ALK-RCC have been reported, and six partner genes have been confirmed.3891011 Here, we present a case of RCC with TPM3-ALK fusion and review its clinicopathological characteristics.
CASE REPORT
A 14-year-old male individual presented with gross hematuria. Abdominal computed tomography revealed a 5.3×4.5-cm, well-demarcated, solid cystic mass at the upper pole of the left kidney (Fig. 1A). There was no further history, and laboratory tests were unremarkable. Hemoglobin electrophoresis showed normal RBCs. The patient underwent left radical nephrectomy, revealing stage III (pT1bN1) disease. The postoperative course was uneventful, and he was discharged without any complications. There was no further treatment after the operation, and no recurrence was observed during the 4-month follow-up period.
Pathological and molecular findings
Grossly, the mass involved the renal medulla and cortex (Fig. 1B). Microscopically, the tumor showed diffuse growth, focal tubulocystic changes, and multifocal inflammatory cell infiltration, similar to renal medullary carcinoma (RMC) (Fig. 2A and B). The infiltrated inflammatory cells were mainly lymphocytes. The tumor cells were dis-cohesive and epithelioid with abundant eosinophilic cytoplasm and cytoplasmic vacuoles. Although most nuclei were round-to-oval, some nuclei were multinucleated and pleomorphic (ISUP grade 4). Mitosis was observed in two to three cells per 10 high-powered fields (Ki-67 index, 10%). Abundant background mucin and intracytoplasmic mucin were frequently seen. Coagulative necrosis was also found. The tumor cells showed diffuse positivity for pan-cytokeratin in immunohistochemistry, and INI1 expression was preserved. In addition, the tumor was positive for PAX8, CD10, and vimentin. Immunoreactivity for TFE3, but without genuine TFE3 rearrangement, was observed. We performed targeted next-generation sequencing. Library preparation was performed using the Oncomine Comprehensive Assay v3 (Thermo Fisher Scientific, Waltham, MA, USA), and the products were sequenced on the Ion S5 System (Thermo Fisher Scientific). Sequencing data analysis was performed using Ion Reporter 5.4. Next-generation sequencing identified a TPM3-ALK fusion gene between exon 7 of TPM3 and exon 20 of ALK. The tumor showed membranous and cytoplasmic ALK expression (anti-ALK antibody, D5F3, Ventana, Tucson, AZ, USA) in tumor cells (Fig. 2C).
This study adhered to the guidelines established by the Declaration of Helsinki and was approved by the Institutional Review Board of Chungbuk National University Hospital (Cheongju, Korea, IRB No: 2019-09-018). Informed consent was obtained from the patient's parents.
DISCUSSION
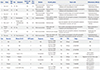
The recognition of ALK alterations in neoplasms is important, because of the potential benefit of ALK inhibitors. However, screening for ALK rearrangement in RCC is not routinely performed in view of cost-effectiveness.12 Previous studies have reported that this tumor is found in <1% of RCCs and in 3.8% of pediatric and young adults with RCC.513 Attempts have been made to establish the characteristics of this tumor; however, its rarity and the variety of histologic features depending on fusion partners make it difficult. Various partner genes (VCL, TPM3, EML4, HOOK1, STRN, and RAD51AP2) have been reported, along with various clinicopathological findings. Of these genes, VCL-ALK RCC was described in children with the sickle-cell trait. TPM3 has been primarily reported as a partner in ALK-RCC. The coiled-coil structure of TMP3 induces dimerization of the fusion protein and promotes ALK activation. Including the present case, eight cases of TPM3-ALK RCC have been reported. We investigated the clinicopathological characteristics of this subtype (Table 1). TPM3-ALK RCCs have been detected in five teenagers and three young-to-middle aged adults. Men and women have been affected equally, although the number of patients is too small to seek any meaning. Symptoms of the disease resulted from mass effects and hemorrhage in two patients. No patients had the sickle-cell trait. All tumors were well-circumscribed and measured 3.1 cm to 7.0 cm (mean, 5.0 cm). Histologically, all cases demonstrated solid growth patterns, and the majority of cases (75%, 6/8) had tubular architectures. The tumor cells had polygonal and pleomorphic cells with abundant eosinophilic cytoplasm and cytoplasmic vacuoles. Some cases (62.5%, 5/8) showed intracytoplasmic mucin, reminiscent of ALK-positive lung cancer. The nuclei presented with high ISUP grade (3 or 4). Intratumoral inflammatory infiltrates, coagulative necrosis, and high proliferative activity were also noticed in most cases. These pathological features were similar to RMC; however, all cases expressed INI-1 and had no clinical findings of RMC. The pathological diagnosis was made in three cases as unclassified RCC. All TPM3-ALK RCCs had exons 20 through 29 of ALK, in which the entire tyrosine kinase domain was included. Two fusion points within the TPM3 gene have been identified (exon 7 and exon 8), and all had a coiled-coil structure for dimerization of the fusion protein. This tumor showed typical ALK expression and TFE3 immuno-positivity in all cases, not related to TFE3 rearrangement. The expression of TFE3 in TPM3-ALK RCC remains unknown. The majority of patients were stage pT1, and half had lymph node metastasis (pN1) at diagnosis. An in vitro study showed that TPM3-ALK fusion conferred higher metastatic capacity than other fusion proteins.14 Although the majority of patients lived uneventfully, a young woman experienced relapse at 1 year after surgery. She was treated with an ALK inhibitor, showing good outcomes.11 Considering lymph node metastasis at diagnosis in half of the cases, increased metastatic potential in in vitro study, and the aggressive clinical behavior in other tumors with TPM3-ALK fusion, TPM3-ALK RCC may be aggressive.15 However, clinical data are insufficient to predict a prognosis.
The present case and literature review suggest that TPM3-ALK RCC may be associated with distinct clinicopathological features. Tests for the detection of ALK translocation are far from routinely performed in all cases. If the morphological features mentioned above are present and TFE3 expression is found in adolescent and young patients, molecular tests for ALK translocation should be performed. This awareness is crucially important, because ALK rearrangement confers sensitivity to ALK inhibitors.


 XML Download
XML Download