

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Esthesioneuroblastoma (olfactory neuroblastoma) is a rare sinonasal tumor originating from the olfactory neuroepithelium. Ectopic adrenocorticotropic hormone (ACTH) syndrome is defined as an abnormal elevation of plasma ACTH secreted from a source other than a pituitary or an adrenal gland.1 New technology that uses radiolabeled somatostatin analogs, such as 68Ga-DOTA-conjugated positron emission tomography (PET), is useful in detecting an unidentified ectopic ACTH-producing neuroendocrine tumor.2 Here, we report a case of esthesioneuroblastoma in which 68Ga-DOTA-conjugated PET was extremely useful.
CASE REPORT
History and examination
A 46-year-old man without significant medical history presented with hyposmia and Cushingoid feature. On laboratory test, hypokalemia (2.6 mmol/L) was identified, and serum cortisol and plasma ACTH levels were 70.1 mcg/dL and 291.4 pg/mL, respectively. A profound increase in 24-h urine cortisol (7665 mcg/day) was also confirmed. Renin and aldosterone were within the normal range and ratio, which excluded primary hyperaldosteronism. In both low-dose and high-dose dexamethasone suppression test (DMST), cortisol was not sufficiently suppressed, which is suggestive of ectopic Cushing's disease, and the result of inferior petrosal sinus sampling (IPSS) was consistent with Cushing's disease. Sellar MRI (Achieva; Philips, Best, Netherlands) showed no pituitary enlargement or tumor and, instead, revealed a bulky mass in nasal cavity (Fig. 1A and B). Due to diagnostic uncertainty on the source of ACTH secretion, we conducted nuclear imaging with a somatostatin analog tracer. The 68Gallium-DOTA-TOC PET scan showed strong uptake in the nasal cavity (Fig. 1C). Preoperative clinical characteristics are summarized in Table 1. Informed consent was obtained from the patient for this report.
Operation
Under the impression of an esthesioneuroblastoma causing ectopic Cushing's syndrome, the tumor was surgically resected. First, the intranasal portion of the tumor was removed by an endoscopic endonasal approach (Supplementary Video 1 only online). The tumor was very soft and hypervascular. We then performed transcranial tumor removal via a bifrontal craniotomy and an extradural approach. The tumor was radically removed together with surrounding dural layer and the anterior skull base. The galeal flap was harvested and used to cover the skull defect. From the nasal cavity, the skull defect was covered by a nasoseptal flap. Lumbar puncture was maintained until 13 days after surgery. After the surgery, the patient was closely monitored in the intensive care unit with regular measurement of serum ACTH, cortisol, and 24-h urinary free cortisol levels.
Histopathological findings
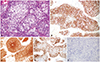
The histopathological diagnosis was that of an esthesioneuroblastoma with Hyams grade I (Fig. 2A). Immunohistochemical staining for ACTH was positive (Fig. 2B). The stains for neuron-specific enolase, synaptophysin, and chromogranin A, which are suggestive of neuroendocrine features, were positive (Fig. 2C and D). Anti T-Pit stain, a reliable corticotroph marker, was negative and disfavored an ectopic ACTH-secreting pituitary adenoma (Fig. 2E). Taken together, the histopathological findings were consistent with ACTH-secreting esthesioneuroblastoma.
Postoperative course
The serum levels of both cortisol and ACTH rapidly dropped to 7.3 mcg/dL and 26.94 pg/mL at 12 hours after surgery and to 17.9 mcg/dL and less than 0.1 pg/mL on postoperative day 3. No remnant tumor was identified in 24-h postoperative brain MRI. After 1 month, the patient underwent adjuvant radiotherapy (total 55 Gy in 25 fractions). 12-month postoperative MRIs showed no recurrence (Fig. 1D). DMST results and 24-h urine free cortisol levels were all normal at 3 months after surgery. Serum cortisol and plasma ACTH levels were 8.4 mcg/dL and 40.00 pg/mL, respectively, at 12 months after surgery. To date, the patient is uneventful.
DISCUSSION
Esthesioneuroblastoma is a rare sinonasal tumor, that can extend to the paranasal sinuses, orbital cavity, and anterior cranial fossa.3 Ectopic ACTH syndrome comprises 5–20% of Cushing's syndrome.14 Esthesioneuroblastoma as a hormone-secreting tissue was first identified in 1967 as a syndrome of inappropriate antidiuretic hormone presentation,5 and ACTH-secreting esthesioneuroblastoma was first described in 1987.6
Endocrinological workup to diagnose Cushing's disease includes low- and high-dose DMST, IPSS, and corticotropin releasing hormone stimulation test. When IPPSS is suggestive of pituitary ACTH secretion and MRI fails to localize a tumor in a sellar region, a dilemma arises as to whether to seek an explorative operation or not. In our case, 68Ga-DOTA-conjugated PET greatly helped in localizing the source of ACTH secretion in the nasal cavity and not performing unnecessary pituitary surgery. In fact, if an ectopic ACTH source is located upstream of the pituitary gland, as with, for example, an ethmoid sinus tumor, petrosal venous ACTH levels may be increased, and thus IPSS can be false positive.789
Because somatostatin receptor expression is a distinctive characteristic of neuroendocrine tumors, 18F-FDG PET or octreotide scintigraphy has been utilized in detecting esthesioneuroblastoma.10 However, 68Ga-DOTA-congugated octreotide PET scan shows greater sensitivity and specificity than conventional 18F-FDG PET or octreotide scan.1112 In our case, where the results of diagnostic tests were discordant, 68Ga-DOTA-conjugated PET clearly demonstrated that the source of ACTH secretion was not the pituitary gland, but a tumor in the nasal cavity. This is the first report to utilize 68Ga-DOTA-conjugated PET to diagnosis undetected ACTH-secreting esthesioneuroblastoma.
The endoscopic endonasal approach provides great accessibility and visibility without extensive destruction of the craniofacial vault.13 However, in this case, because the tumor had invaded multiple paranasal sinuses and the anterior skull base, as well as part of the frontal lobe (Kadish stage C), we accessed the tumor with combined endonasal and transcranial approaches. A high likelihood of local recurrence in the Kadish stage C tumor necessitated adjuvant radiotherapy after the surgery. Some have advocated the usefulness of chemotherapy, especially in the case of cervical metastasis or high histological grade (Hyams grade III or IV).14 Because the histological grade of the tumor in this case was Hyams grade I and radical tumor removal was achieved, the patient did not undergo chemotherapy.
Without question, careful surveillance is mandatory in advanced esthesioneuroblastoma. Not only regular MRI checkup, but also 68Ga-DOTA-conjugated PET is useful for surveillance.2 Furthermore, measuring serum cortisol and plasma ACTH directly provides helpful information. Kanno, et al.7 has proposed that measurement of tumor-associated hormones is important for surveillance. Despite the potential for some unforeseen difficulties, we emphasize that using 68Ga-DOTA-conjugated PET and monitoring ACTH and cortisol levels comprise a reliable and convenient way through which to check for recurrence in ectopic ACTH-secreting esthesioneuroblastoma.


 XML Download
XML Download