

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Musculoskeletal disorders affect morbidity, mortality, and health-related quality of life (HRQOL). Therefore, prevention and treatment of musculoskeletal disorders in older populations is a priority of all interventions.12
Appropriate evaluation of HRQOL must be prioritized. There are many methods for evaluating HRQOL, although an optimal method has not been established.345 Among the proposed methods, the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) is a self-reported disease-specific instrument for assessing pain, stiffness, and function in patients with lower extremity osteoarthritis (OA).6 Use of a short, modified form of the WOMAC questionnaire has been found to improve patient compliance and response rate.789
Although many studies have investigated whether musculoskeletal disease affects disability, few have examined how recognizing musculoskeletal patient disability affects HRQOL scores. Therefore, this study sought to evaluate the validity of the WOMAC short-form (WOMAC-SF) for the assessment of musculoskeletal disorders. We administered the WOMAC questionnaire and evaluated whether the WOMAC-SF was correlated with the WHO Disability Assessment Schedule 2.0 (WHODAS 2.0) and Kaigo-Yobo questionnaires for assessing health outcomes.
MATERIALS AND METHODS
Participants
This cross-sectional study used data from the Namgaram-2 cohort, which consisted of people residing in six rural areas who were enrolled in studies on activity limitations due to work-related musculoskeletal disorders. The cohort comprised individuals aged 60 years or older who agreed to participate in the study from March 2016 to December 2018. Participants were excluded if they had cardiovascular disease, cognitive disorders, stroke, and/or malignancy.
To assess the relationship between musculoskeletal disorders and disability or frailty, we surveyed the WHODAS-12 and Kaigo-Yobo checklist starting in September 2016, additionally. All participants had to provide written informed consent. The study was approved by the Institutional Review Board of Gyeongsang National University (GIRB-A16-Y-0012).
Materials
Nurses who knew the purpose of the study and were trained in data collection procedures conducted a one-on-one survey. The questionnaire took approximately 30 min to complete. The survey included information on sociodemographic variables (age, gender, drinking, and smoking status, marital status) and nutrition status. To standardize the questionnaire, we trained investigators twice a year. Examinations were administered at one hospital to standardize the equipment used.10
In addition, sarcopenia (appendicular skeletal muscle mass, grip strength) and osteoporosis were added as correction variables that may affect the relationship between disease-specific QOL and radiology-confirmed knee osteoarthritis (RKOA).
WOMAC
The WOMAC, which is a pain index measurement for OA, is the most widely used parameter for knee joint function and also a tool for evaluating disorders related to OA of the lower extremities. The WOMAC consists of a total of 24 questions and three subscales. Among them, there are five questions related to pain, two questions related to stiffness, and 17 questions related to difficulties in performing activities of daily living in relation to physical function. The disease-specific tool is of use in clinical evaluation of changes in pain-related health status and clinical outcomes. The WOMAC is valid and reliable for defining function in lower extremity disorders.11
WOMAC short form
Bilbao, et al.12 published the WOMAC-SF, which comprises three pain- and eight function-related questions. WOMAC-SF pain was selected from a previously shortened version that included questions 1, 2, and 4 from the original form.13 WOMAC-SF function included questions 1, 2, 3, 6, 7, 8, 9, and 15 from the original form, based on previous studies and the opinions of patients and experts.14 Therefore, the WOMAC-SF that we used comprised 11 questions grouped into two dimensions: pain (3 questions) and function (8 questions). Final scores for the WOMAC and WOMAC-SF versions were standardized to a value range between 0 and 100, with 0 being the best health and 100 being the worst.
Disability by WHODAS-12
Participant disability was evaluated using the WHODAS-12. This questionnaire addresses difficulties caused by health conditions. Respondents were asked to describe any difficulties they experience in their daily lives. For each item, individuals estimated the magnitude of disability over the last 30 days using a 5-point scale (none=1, mild=2, moderate=3, severe=4, extreme=5). The total score was calculated using the SPSS syntax (available through the WHO), with higher scores representing greater disability, ranging from 0 to 100.1516
Frailty: Kaigo-Yobo checklist
Frailty was evaluated with the Kaigo-Yobo checklist. This checklist is a yes/no questionnaire covering 15 items: activities of daily living (n=1), social activities (n=5), fall-related issues (n=3), nutritional status (n=4), vision (n=1), and hospitalization (n=1). Total scores ranged from 0 to 15, with higher scores indicating greater frailty.17
Measurement of radiologic knee OA
Radiographs of bilateral knee joints were analyzed based on the Kellgren-Lawrence (K/L) classification system, and a score greater than or equal to stage 2 was defined as RKOA. Two radiologists with more than 20 years of experience in musculoskeletal interpretation interpreted the radiographs. Disagreements were resolved by consensus.
Assessment of sarcopenia
Dual energy X-ray absorptiometry (DEXA; Discovery W, Hologic, Waltham, MA, USA) was used to apply the limb skeletal muscle index (SMI), which is obtained by dividing appendicular skeletal mass (ASM) by height squared (SMI=ASM/Ht2). Muscle strength was assessed by handgrip strength. The participants held a digital hand dynamometer (Digital Grip Strength Dynamometer, T.K.K 5401, Takei Scientific Instruments Co., Ltd., Tokyo, Japan) in the standing position. Sarcopenia was defined according to the Asia Working Group for Sarcopenia criteria for low muscle mass strength (hand grip strength below 18 kg in women and below 26 kg in men) and low muscle strength (SMI below 5.4 kg/m2 in women and below 7.0 kg/m2 in men).18
Diagnosis of osteoporosis
Bone density in the lumbar area was measured using DEXA (Discovery W, Hologic). A T score of −2.5 or less was defined as osteoporosis.19
Statistical analysis
SPSS for Windows (version 23.0; IBM Corp., Armonk, NY, USA) and AMOS were used for statistical analysis. Categorical variables are presented as numbers and percentages and continuous variables as means and standard deviations. Pearson's correlation test was used to evaluate the relationship between WOMAC-SF and WOMAC. Associations between WOMAC-SF pain, function, and knee arthritis were evaluated by multiple regression analysis. In addition, confirmatory factor analysis (CFA) was performed to determine the effectiveness of WOMAC-SF as a pain and function instrument. Values of the comparative fit index (CFI) and an adjusted goodness-of-fit index (AGFI) greater than roughly 0.90 may indicate reasonably good model fit.20 Root mean square error of approximation (RMSEA) was used to measure fit. The criteria for judgment were as follows: RMSEA≤0.05, close approximate fit; RMSEA 0.05 to 0.08, reasonable error of approximation; and RMSEA≥0.10, poor fit. CFA was performed by AMOS.
The relationships among WOMAC-SF, disability, and frailty were analyzed via stepwise regression. In all analyses, p<0.05 were defined as significant.
RESULTS
General characteristics of participants
A total of 929 participants were included. The mean age was 68.56±7.40 years, 66.5% were female, and 67.9% had a spouse. Low muscle mass was seen in 22.9% of the population, and 26.5% had low grip strength. Osteoporosis was seen in 14.6% and risk of malnutrition in 15.1% (Table 1).
Concurrent and construct validity of WOMAC-SF
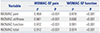
WOMAC-SF pain and function items were associated with WOMAC pain, WOMAC stiffness, WOMAC function, and WOMAC total score (Table 2). Results of CFA for the hypothesized model of two latent factors, pain and function, showed satisfactory fit indices (Table 3). RMSEA values were less than 0.08, and CFI and AGFI values all exceeded the benchmark of 0.90. All factor loadings were significant (p<0.001) (range, 0.605 to 0.917).
In an evaluation of concurrent validity, WOMAC-SF pain was associated with knee OA (b=8.400, p<0.001), as was WOMAC-SF function (b=7.528, p<0.001) (Table 4).
Associations among WOMAC-SF, disability, and frailty with WHODAS-12 and Kaigo-Yobo
Kaigo-Yobo was associated with WOMAC-SF pain (b=0.140, p=0.001) and WOMAC-SF function (b=0.042, p=0.004). WHODAS-12 was associated with WOMAC-SF pain (b=0.679, p=0.003) and WOMAC-SF function (b=0.804, p<0.001) (Table 5).
DISCUSSION
The principle findings of this study were that WOMAC-SF is correlated with the WOMAC questionnaire and that WOMAC-SF was correlated with disability and frailty from the WHODAS-12 and Kaigo-Yobo questionnaires in patients with musculoskeletal disease.
Many disease-specific HRQOLs have been developed and used. To improve their use for outpatient or epidemiological purposes, they must be short, accurate, and sensitive to the disease course. Too many items in questionnaires used for self-reporting lead to missing values, which lowers study validity. In addition, the use of several types of questionnaires in addition to a disease-specific HRQOL questionnaire can be burdensome for patients. Thus, short questionnaires can reduce patient burden and increase response rate, while still evaluating disease state. Therefore, shorter versions should further enhance applicability in epidemiologic studies and clinical practice.
The WOMAC-SF was first published by Yang, et al.,21 who found that in patients with lower extremity OA, the short-form WOMAC function scale was an effective, reliable, and responsive alternative to the original WOMAC. Bilbao, et al.12 also reported that the WOMAC-SF, with three pain items and eight function items, is a great alternative to the traditional WOMAC, with improved usability and acceptability in clinical research and orthopedic clinics. Disease-specific HRQOL tools for assessing knee arthritis, which commonly occurs in older people, typically comprise 20 or more questions.789 In our study, the WOMA-SF correlated with the WOMAC questionnaire in patients with musculoskeletal disease.
In CFA, model fit and factor loading values were appropriate.22 In particular, we saw a difference of 8.4 points in WOMAC-SF pain according to the presence or absence of radiologic knee arthritis, and a 7.5-point difference in function. This result is meaningful in light of results of a study that showed that the minimal clinically important differences for pain and function are 13.3–36.0 and 1.8–33.0, respectively, after knee replacement operation.23
The WOMAC-SF showed a relationship with the WHODAS-12 when analyzed to determine the predictive validity of WOMAC-SF. Musculoskeletal disorders are major health conditions associated with aging that affect morbidity, quality of life, and mortality, and contribute to increased societal healthcare costs.21 Silva, et al.24 analyzed the WHODAS-12 in 204 patients with musculoskeletal pain and reported high disability levels in patients with high musculoskeletal pain. Yoo, et al.3 reported that upper and lower extremity musculoskeletal HRQOL and disability are interrelated in community-dwelling populations. Based on these findings, the WOMAC-SF can also predict disability. In particular, a one-point change in a function item (range: 0–100) was related to a similar 0.8-point change in disability (range: 0–100).
Several aging-assessment tools have been published, including the Kaigo-Yobo test. Hwang, et al.25 reported that the Kaigo-Yobo test adequately assesses frailty in older people. In addition, they evaluated a significant correlation between the Kaigo-Yobo test and arthritis. In our study, WOMAC-SF correlated with the Kaigo-Yobo test. With the WOMAC-SF, pain was more sensitive to score change than function. The change in pain score was 0.140 on the Kaigo-Yobo (range: 0–15), which was similar to the Kaigo-Yobo score when converted to 100 points.
This study had several limitations. First, the study included participants who were not treated for musculoskeletal complaints. Therefore, individual characteristics, associated health conditions, and disease levels may differ from hospital-based participants. Nevertheless, the WOMAC-SF was related to musculoskeletal quality of life, and the WHODAS-12 was related to social disorders, which were interrelated. Second, only knee x-ray was used for diagnosis of lower extremity disorders. Therefore, we could not confirm disability and frailty caused by other diseases of the lower limbs or whether WOMAC-SF correctly identified disability and frailty in the presence or absence of radiologic knee OA. To overcome this problem, we reduced these limitations by further examining osteoporosis and muscle weakness.
In order to measure the HRQOL of knee arthritis in older adults, short survey items are needed to achieve higher reliability and validity. The implication of this study is that the effects of frailty and disability must be considered in the treatment of older adult patients with knee arthritis.
In conclusion, we validated the use of WOMAC-SF for the evaluation of musculoskeletal diseases in a community-based population in relation to WOMAC. Furthermore, we confirmed that WOMAC-SF scores reflected those from the WHODAS-12 and Kaigo-Yobo, which are currently used to assess health outcomes.




 XML Download
XML Download