

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pneumonia was the fourth leading cause of mortality in South Korea in 2017, and Streptococcus pneumonia was the leading cause of bacterial pneumonia.1,2 Despite the use of antibiotics and intensive care over the past 50 years, the case fatality rate of pneumococcal bacteremia has remained at 15–20% in children and young adults, and at 30–40% in the elderly.345 Moreover, the rates of antimicrobial resistance in various pneumococci have been steadily increasing. Under these circumstances, vaccination has become the most cost-effective way to prevent pneumococcal infections.6 The two main types of pneumococcal vaccines are 23-valent pneumococcal polysaccharide vaccines (PPSVs) and pneumococcal conjugate vaccines (PCVs), in which polysaccharides are conjugated to a protein.7 The National Immunization Program (NIP) of South Korea introduced 23-valent PPSVs in 2013 for people aged 65 years and older,8 and PCVs in 2014 for children under 5 years of age.9 The expansion of NIP appears to have benefited both children and adults in recent years; in 2017, more than 2 million doses of pneumococcal vaccines have been administered to both adults and children.10
Amidst the widespread use of pneumococcal vaccines, it would be interesting to analyze the difference in adverse events (AEs) between the two types of vaccines. While the most common adverse reactions after receiving PPSVs were local reactions, such as injection-site pain (soreness, tenderness) (60%), local swelling or induration (20.3%), headache (17.6%), local erythema (16.4%), asthenia and fatigue (13.2%), and myalgia (6.1%), less than 1% of the recipients developed fever or more severe local reactions.11 In comparison, injection-site reactions (erythema) occurred in approximately 10% of PCV recipients, and there may have been an increase in milder injection-site reactions with subsequent doses in older age groups (12–15 months of age).12 Overall, there was no difference between PCVs and PPSVs in terms of the incidence of serious adverse events (SAEs) reported within 1 month of an initial study dose. While these aforementioned studies evaluated the immunogenicity and safety of PPSVs and PCVs in adults who were older than 65 years, these studies were limited in that they were randomized clinical trials involving only 1000 older patients.1314 Therefore, the objective of this study is to analyze AEs after vaccination with different types of pneumococcal vaccines (PPSVs and PCVs) using a spontaneous AE reporting system, and to determine the signals of pneumococcal vaccines by comparing the identified signals with data on vaccine labels in South Korea.
MATERIALS AND METHODS
Data sources
The spontaneous AE reporting system was first introduced in South Korea in 1988 when the Ministry of Food and Drug Safety started collecting spontaneous AE reports. In 2012, the Korea Institute of Drug Safety and Risk Management (KIDS) developed the Korea Adverse Event Reporting System (KAERS) to facilitate computerized reporting and management of AE reports.
Data on the AEs of pneumococcal vaccines were taken from KAERS. The KAERS database contained a total of 39933 reports on AEs after vaccination with pneumococcal vaccines from January 2005 to December 2016. We classified all reported AEs into two subgroups: AEs after receiving PPSVs and those after receiving PCV. We then calculated the percentage of AEs according to vaccine type by dividing the number of AEs after receiving each vaccine type (i.e., PPSV and PCV) by the number of AEs after receiving all vaccines, and analyzed the temporal trends of AEs according to the year from 2005 and 2016. We excluded cases without basic patient data, such as age.
Definition of covariates
When comparing the AEs between PPSVs and PCVs, we included a number of covariates such as age, sex, type of reporter, SAE, and degree of causality. Age was divided into following groups: children aged 0 to 18 years and adults aged ≥19 years for PPSVs, and only children aged 0 to 18 years for PCVs. This was because there was only a single case of AE after receiving PCVs in an adult aged over 18 years in our data. As a result, we could not compare AEs in adults between PPSVs and PCVs. Reporters of AEs were categorized into four groups: physician, pharmacist, nurse, and consumer. SAEs were classified into death and non-fatal categories. The degree of causality was classified into seven terms: certain, probable, possible, unlikely, unclassified, unassessable, and not applicable. This categorization was based on the “World Health Organization-Uppsala Monitoring Centre System for standardized case causality assessment.”15
Coding of AEs
All drug names in the database were coded using the Anatomical Therapeutic Chemical classification system, and AEs were coded using the World Health Organization Adverse Reaction Terminology (WHO-ART, ver. 092). The WHO-ART, developed to serve as a terminology for coding adverse reaction terms, covers most medical terms needed in AE reporting. Following a hierarchical structure, WHO-ART uses system-organ classes and preferred terms as the main and sub-categories, respectively. Symptoms that matched the same preferred terms were treated as the same event. Two or more preferred terms reported for one patient were counted as different vaccine AEs. According to the WHO criteria, SAEs were defined as one of three cases: fatal, causing hospitalization or persistent disability, and life-threatening.
Signal detection and validation
In pharmacovigilance analyses, data mining is a process of detecting signals to find statistical associations and patterns between drugs and AEs in a large database. Three indicators are used to detect signals from spontaneously reported data: proportional reporting ratio (PRR), reporting odds ratio (ROR), and information component (IC). PRR is the proportion of specific AEs for a particular vaccine divided by the proportion of specific AEs for other vaccines. ROR is calculated by dividing the odds of target AEs for patient exposure to a specific vaccine by those for exposure to other vaccines. For PRR and ROR, a signal is detected if PRR and ROR values are 2 or higher, χ2 (chisquared) values are 4 or higher, and the number of occurrences is 3 or greater. IC is a logarithmic metric of the value calculated by dividing the probability of target AEs associated with a target vaccine with the probability of all AEs associated with all vaccines in the database.16 It is given by a Bayesian confidence propagation neural network. The IC criterion was set at the lower limit of 95% confidence interval greater than 0. A signal was defined as the AE that met all three indices of PRR, ROR, and IC.
The detected signals for each vaccine were compared with the information on vaccine labels in South Korea to determine whether the signal was listed on the vaccine label. Assuming the AE listed on the vaccine label is a true value, we examined how accurately the signal detected by data mining discriminated the known AE on the label. The detected signals were validated by calculating four indicators: sensitivity, specificity, positive predictive value, and negative predictive value.
Statistical analysis
We calculated the frequency and percentage (%) of all categorical variables. The Cochran-Mantel-Haenszel chi-squared test was used to compare the demographic characteristics. For testing the difference in proportions, we conducted the exact two-sided chi-squared test based on the test score.17 All variables were considered statistically significant if the p-value was lower than 0.05. SAS (Windows version 9.30, SAS Institute Inc., Cary, NC, USA) and Excel 2013 (Microsoft Corp., Redmond, WA, USA) were used to create a dataset and perform all statistical procedures.
RESULTS
Among the patients vaccinated with PPSVs, females accounted for 62.3% (n=820) of the adult population and 44.9% (n=801) of the children population (Table 1). An equal number of male and female children was vaccinated with PCVs. Physicians reported 47.9% and 80.9% of AEs in adults and children vaccinated with PPSVs, respectively. Moreover, 0.5% (n=6) of adults and 0.9% of children (n=16) died after receiving PPSVs. Among the patients vaccinated with PPSVs, 2.9% and 16.2% of AEs were unlikely to be caused in adults and children, respectively; the causality of another 2.7% and 12.0% of AEs, respectively, was not assessable. Among the children vaccinated with PCVs, 2.4% of AEs were assessed to be possible to have been caused by the vaccines, and the causality of another 0.4% and 0.0% of AEs was assessed as probable and certain, respectively. Most (89.2%) of the adults who were vaccinated with PPSVs received only one pneumococcal vaccine, whereas 56.7% and 47.8% of the children who were vaccinated with PPSV and PCV, respectively, received another vaccine. The median interval between vaccination date and onset date of AEs was 7, 320, and 532.5 days for adults and children receiving PPSVs and children receiving PCV, respectively.
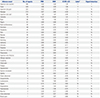
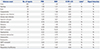
Of all the 39933 AE reports after pneumococcal vaccination, 5718 (14.3%) AEs were pneumococcal vaccine-related (Fig. 1). Injection-site reaction was the most common AE in adults vaccinated with PPSVs, accounting for 25.0% of all AEs. Respiratory system disorders, as a category, were the most frequent AEs in children vaccinated with PPSVs or PCVs (Table 2). Fever occurred frequently in both children and adults vaccinated with PPSVs, accounting for 23.9% and 18.4% of AEs, respectively. The most frequent AE occurring in children after receiving PCVs was pharyngitis (26.2%), followed by rhinitis (23.2%).
We summarized the AEs to compare the signals obtained through this study and labels in Tables 3, 4, and 5. In this study, signals were considered meaningful when all three criteria were significant. These signals were detected only in patients vaccinated with PPSVs. In the case of adults vaccinated with PPSVs, the most frequently reported AEs, such as injection-site reaction and fever, were labeled and represented as signals (Table 3). However, in the case of children vaccinated with PPSVs, the frequently reported respiratory system disorders, such as pharyngitis and rhinitis, were not mentioned on the labels and not detected as signals (Table 4).
A total of 13 AEs after pneumococcal vaccination met the criteria of three data mining indices for signal detection. Twelve AEs reported for adults vaccinated with PPSVs satisfied all three indices for signal detection; three AEs (hypotension, sepsis, and apathy) were not listed on the vaccine label (Table 3). In the case of children vaccinated with PPSVs, only one AE [increased serum glutamic oxaloacetic transaminase (SGOT) level] satisfied all three indices, and it was not listed on the vaccine label (Table 4). No AE satisfied the criteria for signal detection in children vaccinated with PCVs (Table 5).
The results of validation analysis show that PRR and ROR had a sensitivity ranging from 0% to 40% and a specificity from 66.7% to 100% (Table 6). IC had a sensitivity ranging from 0% to 36% and a specificity from 0% to 100%. For adults vaccinated with PPSVs, PRR and ROR indices performed better than IC, albeit slightly. However, in comparing the signals for children, the results were not significant as there were cases of these indices having a value of 0.
DISCUSSION
This study represents a post-marketing safety review of pneumococcal vaccines based on AE reports in KAERS database between 2005 and 2016. The most common AE was pharyngitis in children vaccinated with PCVs and injection-site reaction in adults vaccinated with PPSVs. These results were consistent with the data on labels of PPSVs and PCVs.18192021 Respiratory disorders, such as pharyngitis and rhinitis, in children receiving PCVs were mentioned on the vaccine labels in South Korea based on reassessment results. The result that injection-site reaction was the most frequent AE in adults after receiving PPSVs was consistent with the findings of previous studies.222324
A controlled clinical trial involving adults reported that the degree of injection-site pain was higher for 23-valent PPSVs than for 13-valent PCVs, but there was no difference in the percentage of systemic AEs.14 However, a safety profile comparison would yield different results according to research conditions and target patients. Our comparison of AE reports showed that the proportion of SAEs reported among children was similar for both PPSVs and PCVs. However, cases of death were only reported for PPSVs. In PPSV group, SAEs were reported for a greater proportion of adults than that of children (18.1% and 7.6%, respectively). Most adults (89.2%) received only one vaccine whereas 56.7% and 47.8% of the children vaccinated with PPSVs and PCVs, respectively, received other vaccines. Nonetheless, the percentage of AEs, for which the degree of causality was assessed to be more than possible, was higher for adults than for children. Our findings suggest that SAEs after pneumococcal vaccination are more frequent and probably more causal in adults than in children.
We identified 13 new signals for which all three of the data mining methods used (PRR, ROR, and IC) indicated significant results. Among these, four AEs (hypotension, apathy, sepsis, and increased SGOT level) after PPSV administration were not listed in the approved label. Hypotension and apathy after receiving PPSV have not been reported in South Korea or elsewhere, suggesting the need for further studies. Several cases of sepsis were reported after pneumococcal vaccination; however, they were presumed to have been caused not by the vaccination itself, but by the weakened immunity of the patients.25 Our finding of increased SGOT level was consistent with the finding of a previous study, which showed that elevated C-reactive protein level after vaccination may cause an increase in the serum level of hepatic enzymes.26 According to the results of our validation analysis, PRR and ROR were slightly better than IC for adults vaccinated with PPSVs. The same results could not be obtained for children due to the existence of 0 values for these indices in some cases. A future study with more cases is needed to determine which indicator is appropriate for signal detection in children.
In our data, pneumonia was reported in both adults and children who were vaccinated with pneumococcal vaccines. Although the labels of pneumococcal vaccines list pneumonia as one of the AEs, they only refer to pneumonia caused by serotypes that are not included in the vaccine. The actual case of compensation for the occurrence of pneumonia was rejected since the vaccine did not cause systemic infections.27 Therefore, in order to establish the causality between pneumococcal vaccination and pneumonia, recipients experiencing pneumonia after vaccination should be followed up for serological studies.
To date, there has been no epidemiological study on AEs due to pneumococcal vaccinations in South Korea. To the best of our knowledge, this study is the first to detect signals of AEs after pneumococcal vaccinations by mining KAERS data. The KAERS database contains AE data and reassessment results collected from 27 local monitoring centers in South Korea. In order to increase the rigor of the current study, we used three different data mining methods to detect and validate signals after pneumococcal vaccinations. Due to these strengths, the findings of this study may be useful for analyzing post-marketing AEs of pneumococcal vaccines.
However, this study had a few limitations. The limitations with spontaneous reporting data used in this study include underreporting, inconsistent quality of reports (for example, reports may lack details and important information or contain errors), and the lack of non-vaccinated control groups.28 Furthermore, the data we used did not provide information about other underlying diseases affecting patients or their recovery from SAEs. Therefore, additional studies, including literature reviews, randomized clinical trials, and cohort studies, are required to assess the causality. Moreover, KAERS data did not provide the specific brand names of the vaccines. As a result, AE data were analyzed based on vaccine type (PPSVs and PCVs) only. Finally, although PCVs are currently used for both adults and children, we could not compare the safety profiles of PCVs between adults and children, since only a single case of AE in an adult after receiving PCV was reported in 2016. Further research based on recent data is required to compare the AEs between children and adults after receiving PCVs. Even for children who received PCVs, no significant difference was observed between signal information obtained from our data and the approved label. Addressing the deficiencies highlighted in this study could lead to better management of AE cases in the future.
In conclusion, we identified 13 new signals of PPSVs for which all three data mining methods of PRR, ROR, and IC indicated significant results. Among these, four signals (i.e., hypotension, apathy, sepsis, and increased SGOT level) were not listed in the approved vaccine label. The results of our validation analysis showed that PRR and ROR were slightly better than IC for adults vaccinated with PPSVs, although the same results could not be obtained in children. A future study based on a larger number of AE reports is needed to confirm the validity of the detected signals for children receiving pneumococcal vaccination.





 XML Download
XML Download