

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cerebral palsy (CP) is the most common motor disability in children, and 0.25% of total neonates are diagnosed with CP in Korea.1 Associated reactions (ARs) and mirror movements (MMs) are common motor dysfunctions in children with CP.2 While AR and MM have been used interchangeably to describe unintended motions in the non-task hand, AR is characterized as involuntary movement in non-homologous muscles, either contralaterally or ipsilaterally,34 whereas MM comprises simultaneous involuntary movements of homologous muscles on the contralateral side of the body that accompany voluntary movement.5
Although ARs are considered to be a normal feature of motor behavior in young children due to immaturity of their central nervous system,67 they are considered to be pathological if pronounced and persistent.2 It has been suggested that white matter abnormalities in motor/premotor circuits are responsible for pathologic AR.4 In general, AR is thought to be associated with impaired upper limb function, especially in bimanual activities.5789 However, the association between AR and unimanual function in children with CP still remains inconclusive:2578910 some researchers have reported no significant relation between them,25 whereas others have demonstrated significant associations in both hands 57910 or only in the non-paretic hand.8
This study aimed to characterize unintended contralateral upper arm movement with surface electromyography (SEMG) of multiple muscles during unimanual tasks and to identify factors related with AR in children with CP.
MATERIALS AND METHODS
Participants
This prospective, cross-sectional, observational study was conducted at a university-affiliated, tertiary-care hospital. Children with CP, who were admitted to our hospital for intensive therapy between March 2017 and November 2017, were consecutively screened for inclusion and exclusion criteria. The inclusion criteria were as follows: 1) Manual Ability Classification System (MACS) I (handles objects easily and successfully) to IV (handles a limited selection of easily managed objects in adapted situations), 2) age between 4 and 18 years, and 3) child and/or primary caregiver of the child agreed to participate in this study. Exclusion criteria were 1) inability to understand and follow commands, 2) chemodenervation therapy in upper extremities within 6 months, 3) previous orthopedic surgery in the upper limb within 1 year, and 4) changes in antiepileptic drugs or in medicines for hypertonia, or in their dosages, within 6 months.
The Institutional Review Board (IRB) of Severance Hospital approved this study protocol (approval number: 4-2016-0006). Informed consent was obtained from the primary caregiver and/or the participant, according to IRB rules.
Clinical assessments
For each child, Gross Motor Function Classification System-Expanded & Revised (GMFCS-E&R) and MACS functional levels were determined according to their instruction manuals by one of the authors (Park HK) with 5 years of experience in managing children with CP. GMFCS is used to categorize gross motor function in children with CP into five different levels, with emphasis on sitting, transfers, and mobility. MACS is considered a standard classification system for manual ability in children with CP, and it classifies how children with CP use their hands to do daily activities across five different levels.11 MACS assesses the collaboration of both hands; however, it does not assess the function of each hand separately. In this study, GMFCS or MACS levels of I or II were defined as good functioning, while other levels were defined as poor functioning. The Melbourne Assessment of Unilateral Upper Limb Function (MUUL) is a reliable and valid tool for measuring upper limb function, and it has been increasingly used as an outcome measure in children with CP.1213 MUUL was revised to Melbourne Assessment 2 (MA-2) in an effort to increase uni-dimensionality of the total scale of the original version through Rasch analysis. MA-2 comprises 14 tasks and 30 movement scores grouped across four separate subscales.13 In this study, MA-2 was administered by an occupational therapist who had more than 5 years of experience in managing children with CP.
Associated reaction scoring
Each patient was comfortably seated in a chair, with both arms placed on a table. The children performed three unimanual activities: Task 1, opening and clenching the fist; Task 2, a finger opposition task; and Task 3, tapping fingers on the table surface. Each task was repeated five times for each hand, first with the less-affected hand and then with the more-affected hand. The intensity of visible ARs was assessed according to the method used in previous studies.514 The participants were videotaped (50 frames per second). The occurrence of ARs in each trial was evaluated separately for each task using a four-point scale: 0, no clear imitative movement; 1, barely discernable repetitive movements; 2, slight MM or stronger, but briefer repetitive movements; 3, strong and sustained repetitive movements; and 4, movements equal to those expected for the intended hand.15 The highest score in trials for each task was selected as the score of each task. Total possible scores ranged from 0 to 12. Videos were scored by a physiatrist (Park HK). For each task, if the score was more than 2, it is defined as AR positive in the AR subscale;14 in this study, visible AR was defined as a total score ≥4.
Surface electromyography
For SEMG recording, each patient was comfortably seated in a chair, with both arms on the table surface. While children performed three tasks with one hand, the muscle activities of the contra-lateral shoulder abductor, elbow flexor, elbow extensor, wrist flexor, and wrist extensor muscles were recorded using surface electrodes. Five consecutive trials were performed in each task. Prior to electrode attachment, the skin was rubbed with alcohol, and skin resistance was kept below 5 kΩ. Active electrodes were attached to the belly of the shoulder abductor, elbow flexor, elbow extensor, wrist flexor, and wrist extensor muscles. The reference electrode was placed at the olecranon process. A multi-channel EMG system (MA 300 DTU, Motion Lab Systems, Inc., Baton Rouge, LA, USA) was used to record and analyze EMG data. The band pass filter was set at 20 Hz to 500 Hz. EMG signals were captured at a 1000-Hz sampling frequency. EMG data were transferred to a personal computer after the end of measurement, and were further processed by Matlab software (MathWorks, Inc., Natick, MA, USA). All EMG signals of the five consecutive trials of each task were rectified and integrated. EMG signals in each task were divided into 16 time intervals, and the root mean square (RMS) values of each interval were computed using “rms” Matlab software. We set a baseline period as intervals in which the lowest RMS value appeared continuously in two or more of the 16 intervals, and an active period was set as intervals in which the values were larger than the baseline period. The mean RMS values during the active and baseline periods were assessed. Then, the ratios between active RMS and baseline RMS values were calculated.
Statistical analysis
Since the data were not normally distributed, the Mann-Whitney U-test was used to investigate differences in continuous variables between age groups and MACS groups, and the Wilcoxon rank sum test was used to compare the more- and less-affected sides. Fisher's exact test was used to compare differences in the distributions of functional levels and in the incidence of visible AR between groups due to the small expected cell sizes. Spearman correlation analysis was used to investigate correlations between clinical AR scores and other variables, such as age, MA-2, and RMS ratios of SEMG. Significant variables, except for confounding variables, entered multiple regression analysis to analyze factors associated with scores of clinical AR. Spearman's correlation ≥0.80 was defined as very strong, 0.80–0.60 as strong, 0.60–0.40 as moderate, 0.40–0.20 as weak, and 0.20 as very weak.16 All statistical analyses were conducted with SPSS version 25 for Windows (IBM Corp., Armonk, NY, USA), and p-value <0.05 was considered statistically significant.
RESULTS
Thirty-five children with spastic CP (21 unilateral CP and 14 bilateral CP; 21 boys and 14 girls) were recruited in this study. SEMG data were not available for six children due to poor cooperation throughout the procedures. The mean age of the subjects was 9.6 years (±3.7), ranging from 4 to 16 years. The children were at GMFCS level I to IV (8/13/8/6) and MACS I to IV (7/15/8/5). MA-2 scores were significantly lower in the more-affected side than in the less-affected side (p<0.001). Grouping the children into two groups of young children (age <9 years) and older children (age ≥9 years), we noted that the median age (interquartile range) of the young group was 5.8 years (2.4), whereas that of the older group was 12.4 years (2.9). There was no significant difference in demographic characteristics, including gender, GMFCS and MACS levels, and MA-2, between the young and older groups (Table 1).
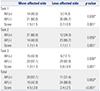
Visible AR (total AR score ≥4) in the more-affected limb was noted in 20 (57.1 %) children, whereas it was noted in 11 (31.4%) children in the less-affected limb. Positive AR (AR subscore ≥2) was significantly more common on the more-affected side than on the less-affected side during Tasks 1 and 3 (p=0.030, p=0.036, respectively). The mean total scores of AR were significantly higher in the more-affected limb than in the less-affected limb (p<0.001) (Table 2).
Visible AR in the more-affected limb was more frequently observed in the low functioning group in regards to manual ability (MACS III to IV) than in the high functioning group (p=0.002), although this difference in visible AR in the more-affected limb was not significant for differences in gross motor function (GMFCS III to IV). In the less-affected limb, there was a significant difference in frequency of visible AR in low functioning groups on both manual ability and gross motor function (p=0.007, p=0.011, respectively). Children with visible AR in the more-affected upper limb had significantly lower MA-2 scores than children without AR. However, there were no significant differences in MA-2 scores in the less-affected upper limb according to presence of visible AR, except for dexterity (Table 3).
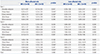
Muscle activities increased during trials of each task from baseline activity at resting status in the limb with visible AR (Fig. 1). RMS ratios were significantly higher in some muscles of the more-affected upper arm when performing tasks with the less-affected limb. For the more-affected limb, RMS ratios of the elbow flexor and extensor for Task 1 (p=0.034, p=0.004, respectively) and elbow extensor and wrist extensor for Task 3 (p=0.046, p=0.025, respectively) were significantly higher in the group with visible AR, compared to the group without visible AR. For the less-affected limb, children with visible AR had significantly larger RMS ratios in the wrist flexor during Task 1 without any significant differences during other tasks, compared to the group without visible AR (p=0.005). The average total RMS ratios of the three tasks did not show significant differences between groups with and without visible AR on either the more- or less-affected side (Table 4).
Visible AR in the more-affected limb was significantly more common in the young children group than in the older children group (p=0.002). However, the presence of visible AR in the less-affected limb was not significantly different between the young and older children groups. The total scores of AR in the more-affected limb were significantly higher in the young children group than in the older children group (p=0.003), whereas total AR scores in the less-affected limb were not significantly different. Children in the high functioning group of manual ability (MACS I–II) had significantly higher MA-2 scores and lower AR total scores in both the more-affected and less-affected limbs (Table 5).
Visible AR in the more-affected limb was noted in 17 (81 %) children with unilateral CP, whereas it was noted in only nine (42.9%) children in the less-affected limb. Visible AR was significantly more common on the more-affected side than on the less-affected side in children with unilateral CP (p=0.011). Visible AR of the more-affected upper limb was significantly more common in children with unilateral CP than in children with bilateral CP (p<0.001), although there was no significant difference in frequency of visible AR in the less-affected limb between children with unilateral and bilateral CP. The mean scores of AR were significantly higher in the more-affected limb than in the less-affected limb only in children with unilateral CP.
AR scores in the more-affected upper limb showed a strong association with MA-2 score (ρ=−0.700, p<0.001) and moderate relationships with the ratio of RMS (ρ=0.476, p=0.012) and age (ρ=−0.471, p=0.004), whereas AR scores in the less-affected limb showed only moderate association with MA-2 score (ρ=−0.414, p=0.013). Multiple regression analysis revealed that age and MA-2 were significant factors associated with AR scores in the more-affected hand (p=0.010, p=0.002, respectively), whereas no factor was associated with AR scores in the less-affected hand. Also, the standardized beta of MA-2 was larger than that of age in the more-affected side, with negative values (Table 6).
DISCUSSION
In this study, AR was assessed using a clinical tool and SEMG in multiple muscles, and we found motor overflow up to the elbow muscles of the non-task hand depending on the task and side, as well as significant factors related to the extent of AR in the more-affected side.
Previous studies have shown inconsistent results regarding the association between AR and upper extremity function.2578910 Among those studies, only Klingels, et al.8 administered MUUL for unimanual function, and found a significant association between MM and the scores of MUUL only in the paretic limb. The results of our study on the association of AR with unimanual function were consistent with those of Klingels, et al.8
ARs are present in normal children up to the age of 9 years and then systematically diminish.617181920 In the present study, visible AR was more common in younger than in older children. These findings suggest that AR reflects CNS immaturity. However, AR was more common in the more-affected limb than in the less-affected limb, and we discovered a stronger association for visible AR with upper arm function, rather than age, suggesting that both upper arm function and age are related to AR. In addition, visible AR in the less-affected limb was only related to upper arm function. These findings imply that in children with CP, upper arm function plays a more significant role in AR than CNS immaturity in young children.
To our knowledge, the present study is the first to describe muscle activity according to presence of visible AR in children with CP. The present study documented increased muscle activities in the wrist and elbow muscles in the contra-lateral upper limb depending on task and side in children with AR. Also, muscle activation patterns in the non-task limb were different from activation patterns in the task limb. When performing voluntary movements, muscle activity in the contralateral upper arm was increased in both homologous muscles and non-homologous muscles. In patients who had experienced stroke, unintended contralateral upper limb muscle activation across multiple muscles of the contra-lateral non-task upper limb during pinch grip was observed.21 In that study, the researchers demonstrated that the non-task hand did not mirror the task hand's muscle activation patterns. Since there were differences in the muscles selected for SEMG and unimanual tasks between studies, a comparison of the results of our study with those of previous studies seems to be unreasonable. However, based on those findings, the muscle activity recorded from SEMG seems to differ depending on the side (paretic/non paretic) or upper arm function, type of unimanual task, and muscles selected for recording. In consideration of these factors, further studies are needed.
In the current study, AR was more frequently observed in the more-affected limb. Chiu, et al.10 also reported that AR is more common in the more-affected limb in people with quadriplegic CP. On the other hand, some studies have reported more frequent MM in the less-affected hand in children with hemiplegic CP.578 Meanwhile, lesion timing is also considered to be a significant factor related to AR in patients with hemiplegic CP. Significantly higher muscle activity in elbow flexion in the paretic hand has been observed in children with hemiparesis in pre- and perinatal brain groups.22 In addition, MM in the paretic hand in hemiplegic CP was related to earlier brain lesions.8 Taken together, we propose that there are various factors associated with the occurrence of AR in children with CP, which seem to contribute to the inconsistent results of the studies. Therefore, further investigation of AR is needed in order to characterize AR in consideration of these factors in children with CP.
The lack of a normal control group was a major limitation of our study. In future studies, the extent of AR in children with bilateral CP should be compared with that of a normal control group. Despite these limitations, this study revealed increased muscle activity in various muscles, as well as factors associated with AR.
In conclusion, in children with visible AR, motor overflow to the elbow and wrist muscles in the non-task hand during unimanual hand tasks was observed depending on the side and task. Age and upper arm function were significant factors related to the extent of AR in the more-affected limb of children with CP.





 XML Download
XML Download