

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The concept of “trimodal distribution of trauma deaths” suggested by Trunkey1 in 1983 has been widely accepted in traumatology. However, many criticize that this concept does not represent the general trauma death distribution around the world in current times, since the study included many penetrating injuries in urban areas in the 1970s.2345 For example, a different pattern of trauma deaths is expected in Korea, which reports over 90% blunt injuries. Nevertheless, few studies have been conducted on this issue, and as a result, the trauma system is still not in tandem with the Korean situation, despite its highly preventable trauma death rate.678910
Gyeonggi Province is one of the representative administrative regions with the highest population density in Korea. Unsurprisingly, the largest number of trauma deaths occurred in the region. This study was designed to provide a basis for building a master plan for the national trauma system by analyzing the data distribution of trauma deaths extracted from the emergency medical system database in Gyeonggi Province. In particular, we analyzed the distribution pattern based on mechanism of injury, time to death, and cause of death.
MATERIALS AND METHODS
This is a secondary data analysis study based on the “Project for the Establishment of a Regional Trauma System,” which was performed by a collaboration between Ajou University Hospital and the local government of the Gyeonggi Province. The original target population of our study included all trauma patients who visited the 66 emergency medical institutions located in Gyeonggi Province from January 1, 2017 to December 31, 2017. We extracted the data on injured patients (n=548158) from the National Emergency Department Information System (NEDIS) database. The study was approved by the Institutional Review Board of Ajou University Hospital with a waiver for informed consent (IRB no. AJIRB-MED-EXP-18-157).
We included the cases with one or more of the injury codes of the Korean Standard Classification of Diseases (KCD). Patients with KCD codes for frostbite, intoxication, drowning, burn, and unspecified injury or complication were excluded. Five hundred cases were sampled using the stratified two-stage cluster sampling method. The number of deaths, level of hospital, and decision to transfer (yes or no) were used as the first stratification variables for sampling. Moreover, the sites where deaths occurred (deaths on arrival, at the emergency room, after hospitalization, and after transfer to other hospital) and the patient's age were used as the second stratification variables for sampling. Additionally, cases with missing information were excluded from further analysis through the panel review of medical records (Fig. 1).
Basic demographics of the study population, time to death, cause of death, and mechanism of injury were collected from death certificates, first aid activity records, hospital medical records, and radiologic imaging findings records. The time from trauma to death was divided into four periods: within a day, over a day within a week, over a week within a month, and over a month. Additionally, the distribution of deaths within 24 hours was further analyzed.
The duration of posttraumatic deaths was divided into five intervals (within 4 hours, over 4 hours within a day, over a day within a week, over a week within a month, and over a month) to investigate the distribution of trauma deaths according to the time from injury to death by cause of death and mechanism of injury. The mechanisms of injury were classified into six categories: traffic-related accident, fall from height, fall from standing (ground fall), struck by, cut/pierce, and not further specified or unknown. Cause of death was classified as bleeding, central nervous system (CNS) injury, multiple organ dysfunction syndrome (MODS)/sepsis, respiratory arrest, cardiac arrest, and not further specified or unknown, according to the World Health Organization trauma quality improvement program guidelines.11 Final decision on the cause of death was made by multi-panel reviews (three teams consisting of five trauma care experts each). The rule of decision was to choose one cause that contributed the most to death; however, when deciding on only one cause was difficult even after discussion with multi-panels, the cause was designated as “multiple.”
Data were analyzed using SPSS version 25 (IBM Corp., Armonk, NY, USA) and presented as median and IQR for continuous variables or percentages for categorical variables. The difference in time distribution among the time from injury to death groups, according to the mechanism of injury and cause of death, was verified using the chi-square test. p values were considered significant when they were less than 0.05.
RESULTS
Of the 1546 trauma deaths reported in Gyeonggi Province, 328 cases were included in the final study population, after excluding the cases with missing or inappropriate information for review (Fig. 1). The number of males (220, 67.1%) was twice that of females. The mean age was 61.8±23.3 years, and two-thirds of the study population were over the age of 60 years. Blunt mechanism of injury had a significantly higher incidence (98.5%) than penetrating trauma. Patients who died within a day after injury were the most prevalent (40.9%). Mortality rates for the second day after the accident to the first week, between the second week and the first month, and after a month were 27.4, 21.6, and 10.1%, respectively. Of the 134 trauma patients who died within 24 hours, 91.8% died within 12 hours. The cases within 1 hour accounted for 40.3% (54/134) of the highest proportion (Table 1, Fig. 2).
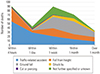
Traffic-related accident (38.1%) was the most common mechanism of injury, followed by falls from height and ground. Majority of trauma deaths within 4 hours were caused by traffic-related accidents (55, 60.4%) and falls from height (30, 33.0%). The number of deaths due to falls from the ground increased rapidly as time went by, and peaked during the period between “over a week” and “within a month.” Statistically significant differences existed in the time distributions from injury to death according to mechanism of injury (p<0.001) (Table 2, Fig. 3).
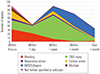
The most common cause of death in trauma patients was CNS injury (42.4%), followed by MODS/sepsis and bleeding. The deaths caused by bleeding and CNS injury accounted for most early trauma deaths within a day (70.1%). Over one day and within a week, CNS injury was an unrivaled cause of trauma death. Conversely, MODS/sepsis had the highest ratio (23, 69.7%) of late death after a month. A statistically significant difference existed in the time distribution from injury to death according to cause of death (p<0.001) (Table 2, Fig. 4).
DISCUSSION
Since the concept of trimodal distribution was first introduced, studies on trauma death distribution have been conducted outside of Korea.12345 Although several investigations on preventable trauma deaths have been conducted since the 1990s, few studies have been conducted on the timing of deaths in Korea.678910 This could be due to the lower rate of autopsies conducted in the country.12 However, the main reason was that no basis has been established for in-depth analysis and investigation on trauma deaths due to the lack of a trauma system.1314 Moreover, previous studies on preventable trauma deaths in Korea tended to focus on determining the preventability of death and calculating mortality rates.678910 These studies did not investigate in detail the timing of death, mechanism of injury, and cause of death. As a result, the trauma system in Korea has not yet reached a level that is high enough to draw corrective action plans or injury prevention programs. Although this study did not include all of the data on trauma deaths in the country, we extracted data on nearly half of them for a year in the most populous province in Korea. It is significant that the pattern of trauma deaths be understood according to the mechanism of injury and cause of death through professional reviews by a multi-panel of experts.
In our study, the pattern of trauma deaths in our province was close to a bimodal distribution, which was different from the traditional trimodal model. This indicated that the traditional concept of trimodal distribution may no longer be accurate for the recent trauma situation in Korea. Our findings were consistent with those of previous studies conducted in other developed countries.2345 As suggested in these studies, bimodal distribution was observed since the boundary between immediate and early deaths became obscure, due to the development of active injury prevention programs and pre-hospital transfer system as well as the implementation of well-organized comprehensive trauma systems. Conversely, the late deaths caused by underlying diseases or MODS/sepsis became more frequent than early deaths, due to the trauma itself. However, we should consider the possibility that these results reflected the domestic situation where few gunshot injuries and fewer penetrating traumas were recorded compared to the USA. Even though a similar study was conducted in 2001, the results could not be compared with this study as it was not population-based and focused on patients who visited only one hospital.15 To understand the current situation and establish a trauma system in Korea, a nationwide population-based epidemiological study on trauma deaths should be conducted in the near future.
According to the mechanism of injury, early deaths mostly included traffic-related accidents and falls from height, which are usually considered to be the two most common mechanisms of injury in Korea. Late deaths, usually referred to ground falls, occur mostly in older individuals. These findings were similar to those of other studies, which revealed that traffic-related accidents and falls were the main causes of early deaths from blunt trauma.4516 However, we should consider that the two studies conducted in the USA reported that 24% to 48% of the cases were penetrating injuries, whereas the other study performed in New Zealand included other mechanisms of injuries, such as hanging and burning. Nevertheless, based on these results, we can derive that a focus should be placed on injury prevention through the establishment of safety devices or guidelines to prevent early deaths in cases of traffic-related accidents.
In this study, we distinguished ground falls, which usually occur in elderly patients, from falls from heights, such as buildings and construction fields. As a result, we were able to confirm that deaths from ground falls account for a high percentage of trauma deaths in Korea, as revealed by a similar study.5 The percentage may have been over-estimated due to the longer length of hospital stay in Korea than that in the USA. The treatment outcomes in the USA are difficult to understand, as fewer data are available on follow-up after discharge at the first hospital, which is due to the quick discharge or transfer to other facilities immediately after performing initial trauma care.17 However, our results indicated that many geriatric trauma patients died from ground falls, especially in the late period. Considering that geriatric ground falls are usually not severe enough to cause death in early stages, this result suggests that a specialized team or treatment strategy, which can be offered thorough intensive care for them over all periods, are needed to prevent deaths.
When it comes to cause of death, CNS injury was the most common, followed by MODS/sepsis and bleeding. This result was consistent with those of other research that were conducted in the USA during the 1970s to 1990s.1819202122 Few studies have been conducted on the causes of trauma deaths due in part to the difficulties of follow-up, as Sobrino and Shafi23 pointed out in his review article. Other researchers have insisted that late deaths after about 30 days of being discharged from a hospital should be considered as non-traumatic deaths, and this controversy also makes detailed classification for cause of trauma death more complicated.242526 In this study, we determined the cause of death by consensus based on multi-panel review, in case opinions within the panel were different from one another. Nonetheless, we cannot deny that some cases were classified as multiple, not-further specified, or unknown cause of deaths, since no consensus was reached in certain cases.
The distribution of causes and timing of trauma deaths indicated that deaths from bleeding were the main cause of early deaths, whereas CNS injury peaked within a week after the accident. We confirmed that the cause of early trauma death was mainly bleeding and CNS injury in Korea, as previous studies mentioned.182122 However, existing studies have shown that deaths from bleeding or CNS injury were usually reported within 2 days,1921 whereas this study revealed that CNS injury is the most common death within a week. We need to recognize that CNS injury may progress irreversibly to death within a week, unless appropriate treatment is given early, although it may not be as urgent as bleeding.
Death from MODS/sepsis peaked within a month after injury, as previous studies indicated.1192122 Sudden respiratory arrest was one of the leading causes of death, which can occur at any time within a month after injury. Cardiac arrest was observed in both early deaths, which mainly resulted from a direct impact on the heart or great vessels, and late deaths, which were caused by myocardial infarction or arrhythmia during the later period. This suggests that intensive surveillance and care for complications that may occur at any point during the treatment process should be accompanied with appropriate early care for injury until the final stage of recovery in order to prevent death.
This study had some limitations. First, since it was a retrospective study using medical records, data accuracy could not be ensured. Second, the sample size was small, and many cases were excluded during the multidisciplinary panel review process owing to insufficient information for a complete review. However, statistical experts determined the sampling method and size to be sufficient for estimating differences and representing the population. Third, it was difficult to classify cause of death exactly, since no autopsy data were available. We tried to minimize the effect of this limitation by reviewing and discussing cases among three different team panels consisting of five trauma care experts each. Lastly, even though the target region had the highest population density, it may not be representative of the entire Korean population.
In conclusion, we confirmed the distribution of trauma deaths in a province of Korea. The mechanism of injury in Korea was different compared to other studies that were conducted in the USA, which had high rates of penetrating injuries such as gunshots. However, the distribution of overall timing of death was found to follow a bimodal pattern rather than a trimodal distribution. In cases of death by bleeding, the importance of the golden hour was proven in our study, as it still showed high death rates within 1 hour after injury. However, it should also be noted that more blunt trauma deaths, which can take at least 2 to 4 hours for resuscitation, and less penetrating injuries, which can cause death within a shorter amount of time—even in a few minutes, are usually recorded in Korea than in the USA or other western countries. Moreover, considering that most cases of CNS injury could live long enough to be hospitalized for more than a week, it is important to remember that there could be many patients who may have the chance to undergo better management somewhat earlier. It is also necessary to take measures to prevent injuries and provide critical care for patients who may die from ground falls, which showed a particularly high distribution in the late stage. Based on our findings, a suitable and modified trauma system should be developed in Korea, and further studies on the nationwide distribution of trauma deaths should be conducted in the near future.




 XML Download
XML Download