

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Metabolic syndrome (MetS), also known as syndrome X or insulin resistance, is a growing health problem, with increasing prevalence in Asian countries and in the U.S.1 MetS is a multiple risk factor for type 2 diabetes, atherosclerotic cardiovascular disease, and non-alcoholic fatty liver disease.2 The causes of MetS are excessive energy intake, physical inactivity, sedentary lifestyle, excessive alcohol use, aging, disrupted sleep, mood disorder, psychotropic medication use, and genetics.345678 The World Health Organization Expert Consultation reported that MetS is a pre-morbid condition, rather than a clinical diagnosis, as well as an educational concept involving a complex multifactorial health problem.9
Lifestyle modifications, such as an energy-restricted diet and physical activity, are strategies to prevent the development of MetS.10 Several randomized controlled trials have shown that regular physical activity effectively prevents type 2 diabetes, while increasing the total physical activity volume decreases the development of MetS.11 An analysis of the dose-response association between physical activity and incident hypertension in cohort studies showed that every 10 metabolic equivalent of task (MET) h/wk increase in leisure time physical activity (LTPA) reduced the risk of hypertension, a component of MetS, by 6%.12
The 2018 Physical Activity Guidelines for Americans distributed by the U.S. federal government recommend 150–300 minutes of moderate-intensity or 75–150 minutes of vigorous-intensity activity a week to achieve substantial health benefits.13 Researchers reported that, compared to individuals not performing LTPA, those performing three to five times the minimum MET h/wk of physical activity recommended by the Physical Activity Guidelines for Americans demonstrated a 39% lower mortality risk.14 For Koreans, the prevalence of MetS has shown an increasing tendency among men 19–49 years since 2007 and nearly 40% women aged over 60 years have MetS.15 To prevent cardiovascular events, type 2 diabetes mellitus, chronic kidney disease, cancer, and even all-cause mortality associated with MetS, an appropriate physical activity recommendation must be established for Koreans.1617 However, few observational and prospective studies examining the association between physical activity and the incidence of MetS for Koreans have been published.
Thus, the goal of this study was to investigate the association between LTPA levels and the incidence of MetS over 10 years of follow-up in Korean adults. We also evaluated the LTPA levels that might be recommendable to efficiently reduce the risk of MetS.
MATERIALS AND METHODS
Study population and design
We analyzed data from the Ansung-Ansan cohort within the Korean Genome Epidemiology Study (KoGES; 4851-302). The Ansung-Ansan cohort is a population-based prospective study that consists of people aged 40–69 years residing in a rural and urban community. This project was initiated in 2001 by the Korea Centers for Disease Control to investigate the risk factors of various chronic disorders. Ansung-Ansan cohort participants were first recruited from 2001 to 2002 and comprised 10030 people aged 40–69 years with the same ethnic background. Every 2 years, the participants were re-examined; by the sixth follow-up (2013–2014), 5906 people participated. Among them, we excluded 1650 subjects who had more than three components of MetS and further excluded 346 subjects for whom data on MetS components were missing. After these exclusions, 3910 subjects were enrolled in the analysis (Fig. 1). At each examination, all participants provided informed consent.
This study protocol was approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR317305) and the Ethics Committee of the Korean Center for Disease Control (KoGES; 4851-302).
Data collection
A comprehensive health examination and health-related interview were completed by all participants. The health examination included the collection of biological specimens and anthropometric indices for assessment. The health-related interview was performed using a questionnaire covering family disease history, medication use, and lifestyle characteristics, such as alcohol use and smoking status. All tests and interviews were conducted by health professionals who followed a standardized protocol using required instruments to collect the data. Detailed information about the data collection procedure is available in a previous report.18
Definition of MetS
This study defined MetS in accordance with the worldwide consensus criteria of MetS issued by the International Diabetes Federation, American Heart Association, National Heart, Lung, and Blood Institute, International Atherosclerosis Society, World Heart Federation, and International Association for the Study of Obesity modified National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III).3 MetS was defined as the presence of three or more of the following components: 1) abdominal obesity, defined as a waist circumference ≥90 cm for males or ≥85 cm for females (following Korean specific cut-offs for abdominal obesity defined by the Korean Society of Obesity)19; 2) high blood pressure, defined as a systolic blood pressure ≥130 mm Hg and a diastolic blood pressure ≥85 mm Hg or treatment with antihypertensive agents; 3) hypertriglyceridemia, defined as a serum triglyceride concentration ≥150 mg/dL or specific treatment for this lipid abnormality; 4) low high-density lipoprotein (HDL) cholesterol level, defined as a serum HDL cholesterol concentration <40 mg/dL for males or <50 mg/dL for females, or specific treatment for this lipid abnormality; 5) high fasting glucose level, defined as a fasting serum glucose level ≥100 mg/dL or current use of antidiabetic medication.
LTPA assessment
LTPA was assessed using a questionnaire to quantify activities in the leisure time domain. All participants were asked the types, duration, and frequency of LTPA performed. LTPA levels were determined by calculating MET-h/wk as the time spent exercising/week and assigning a weight based on exercise intensity.2021 The MET is an objective rate measure of the amount of physical activity performed, and the intensities of physical activities were standardized according to the Compendium of Physical Activities.21
LTPA volume (MET h/wk) was calculated by multiplying the median or midpoint of duration and frequency of the performed LTPA by the reported intensity of that LTPA category by its assigned MET value. One MET is defined as 1 kcal/kg/h and is considered the resting metabolic rate during quiet sitting (1 MET=3.5 mL/kg/min of oxygen consumption).20 LTPA volume (MET h/wk) was calculated in this study as follows:
There were nine types of LTPAs in the Ansung-Ansan cohort at baseline: aerobics, jogging, swimming, tennis, golf, bowling, fitness club exercise, walk, and climbing.
Statistical analysis
To analyze the relationship between LTPA levels and MetS, we counted the numbers and percentiles of demographic characteristics for the participants at the first examination for comparison between the normal and MetS groups during the follow-up period. The chi-square test was performed to estimate differences between two groups according to covariates and to calculate p values. Mean values of each LTPA volume type between two groups were compared using Student's t-test. The chi-square test, as a non-parametric statistic, was used for categorical variables, while Student's t-test, as a parametric statistic, was used for normally distributed variables.
Furthermore, we performed multivariate-adjusted logistic regression analysis to generate relative risks (RRs) and 95% confidential intervals (CIs) for LTPA levels and MetS incidence. We categorized LTPA volume into five categories for MET-h/wk (0, 0.1 to <7.5, 7.5 to <15.0, 15.0 to <22.5, 22.5 to <40.0, and ≥40.0). These five categories were established to reflect multiple levels of the minimum recommendation of Physical Activity Guidelines for American and ranged from one to two times the recommended minimum (7.5 to <15.0 MET-h/wk) to up to five or more times the recommended levels (≥40.0 MET-h/wk).22 The first model was a crude model in which the RR of MetS incidence associated with higher LTPA levels versus the lowest LTPA level (i.e., physically inactive during leisure time at 0 MET-h/wk). Final models were adjusted for sex, age, educational level, income level, marital status, smoking status, alcohol use, and body mass index.
RESULTS
Among the 3910 participants included in this study analysis, MetS developed in 1023 (26.2%) during the 10-year follow-up period. The mean follow-up period was 11.8 years. Table 1 shows the baseline characteristics of the participants according to MetS incidence. Participants with MetS were older, less educated, had less income, were smokers, and had a higher body mass index. These differences between groups were greater among females than males (Table 1). We also compared LTPA participation and quantities according to MetS incidence (Table 2). For this comparison analysis, we excluded participants reporting no LTPA in the assessment of total LTPA MET-h/wk. Of the 2887 participants in the normal group, 139 (4.8%) and 52 (1.8%) participants reported swimming and golf as LTPAs, compared to the MetS incidence group [n=29 (2.8%) and n=10 (1.0%), respectively]. Regarding the performed LTPA quantities, the normal group performed more LTPA in aerobics, swimming, golf, and climbing than those in the MetS incidence group (mean METs were 22.0, 27.9, 25.4, and 25.3 MET-h/wk among the normal group and 18.8, 26.0, 17.3, and 23.2 MET-h/wk among the MetS incidence group, respectively). When assessing total LTPA participation and performed LTPA quantities between the two groups among females, the normal group was more likely to participate in LTPA, while the total average quantity of LTPA was larger in the MetS group than normal group among males (Table 2).
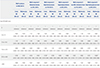
Table 3 shows the results of multivariate logistic regression analysis assessing the association between changes in LTPA levels and the incidence of MetS after the adjustment for related covariates. High blood pressure was most common in this study, and the presence of a high fasting glucose level was the least common MetS risk factor [n=1770 (45.3%) and n=919 (23.5%), respectively]. As the category of total volume of LTPA levels increased, there was trend of a decreased likelihood of developing MetS. Although this was not significant, we observed a 13.4% lower risk of MetS in those performing LTPA at two to three times the recommended minimum (15.0 to <22.5 MET-h/wk: RR, 0.87; 95% CI, 0.60–1.24), and this association grew stronger at three to five times the minimum (22.5 to <40.0 MET-h/wk: RR, 0.77; 95% CI, 0.57–1.03). The multivariate adjusted analysis also showed this trend, although this relationship was also insignificant (15.0 to <22.5 MET-h/wk: RR, 0.96; 95% CI, 0.65–1.40; and 22.5 to <40.0 MET-h/wk: RR, 0.78; 95% CI, 0.57–1.06, respectively). In analyses of LTPA and MetS incidence, we found an inverse trend among participants performing five or more times the recommended minimum (≥40.0 MET-h/wk), compared with lower levels of total LTPA (crude RR, 0.89; 95% CI, 0.65–1.21; adjusted RR, 0.93; 95% CI, 0.67–1.29). In stratified analyses of MetS risk factors, a positive association was found at one to two times the recommended minimum or higher levels. In univariate logistic regression analysis, associations for three to five times (22.5 to <40.0 MET-h/wk) and for more than five times (≥40.0 MET-h/wk) the recommended minimum with the presence of high blood pressure were significant. However, only more than five times (≥40.0 MET-h/wk) the minimum was significant after adjustment for related covariates (≥40.0 MET-h/wk: RR, 0.74; 95% CI, 0.55–1.00). We also found that participants performing three to five times (22.5 to <40.0 MET-h/wk) the minimum had a 31% lower risk of having a high fasting glucose after adjustment (adjusted RR, 0.69; 95% CI, 0.50–0.95).
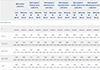
Tables 4 and 5 show the RRs of MetS incidence by sex stratification. Compared with no baseline LTPA, more than two times the recommended minimum might be associated with lower risk of MetS and MetS components. This association was stronger in females than males. We observed a 34.5% lower risk of MetS significantly among participants performing three to five times (22.5 to <40.0 MET-h/wk) the minimum in females (crude RR, 0.66; 95% CI, 0.43–0.99). Abdominal obesity (crude RR, 0.65; 95% CI, 0.44–0.96) and high blood pressure (crude RR, 0.53; 95% CI, 0.36–0.79), which are MetS components, also had significant association with LTPA of more than 5 times the minimum (≥40.0 MET-h/wk). Regarding high fasting glucose level, the significant association was remained after adjustment for LTPA of three to five times (22.5 to <40.0 MET-h/wk) the minimum (crude RR, 0.57; 95% CI, 0.34–0.95; adjusted RR, 0.50; 95% CI, 0.29–0.89).
DISCUSSION
In the present study, we assessed the relationship between total LTPA levels and the incidence of MetS in Korean adults among the Ansung-Ansan cohort community-based prospective study. Our main finding was that the relative risk of MetS decreased as total LTPA levels increased, although the difference was not statistically significant. The 3 to 5 times level (22.5 to <40.0 MET-h/wk), the recommended minimum of 7.5 metabolic-equivalent hours per week, reduced the risk of MetS by 21.9%. Furthermore, participants who performed more than three times the minimum recommended activity had a significantly lower risk of high blood pressure, an abnormal MetS component. We also found that more than three times the recommendation of LTPA could reduce MetS risk significantly in women, as well as the risk of abdominal obesity, high blood pressure, and high fasting glucose level. In terms of LTPA volume, performing three times the recommended minimum was associated with a lower risk of MetS incidence and abnormal MetS components for Korean adults.
As the Western lifestyle spreads worldwide, the prevalence of the MetS is increasing.1 The consumption of high-calorie, low-fiber fast food and decreases in physical activity due to increased transportation and sedentary lifestyle result in MetS.25 Approximately 20–25% of the worldwide adult population carry MetS risk factors.26 In the U.S., 29.2% of adults had MetS according to the National Health and Nutrition Examination Survey 1999–2006, and an increase in MetS prevalence was expected.27 For Korea, the prevalence of MetS in 2013–2015 was 20.3% and remained stable since 2007 on the Korea National Health and Nutrition Examination Surveys.15 The results of this prospective study reported a 26.2% MetS incidence. These findings demonstrate that the increasing MetS trend has been maintained and remains a serious public health concern. Moreover, preventive strategies to manage MetS risk factors are needed.
Performing physical activity regularly is associated with a reduced risk of mortality and influences life length.2829 A preceding study, which divided the total weekly minutes of moderate or vigorous physical activity into three categories (0, <150, and ≥150 min/wk), reported an almost two times higher risk of MetS occurrence than in those who performed more than 150 min/wk of physical activity.30 Another prior cross-sectional study found that the frequency of MetS was lower among those who reported performing moderate or vigorous physical activity.31 A meta-analysis of prospective cohort studies revealed that a high LTPA level was associated with a significantly decreased risk of MetS.32 We observed consistent findings to those of other studies, although the association between total LTPA level and MetS incidence in our study was not statistically significant.
In a previous study that investigated the association between physical activity and MetS components, physical activity was a protective factor for low levels of HDL cholesterol in regard to MetS.33 Another previous study stated that higher mean volume of physical activity exhibited inverse associations with all components of MetS, decreasing the presence of abdominal obesity, hypertriglyceridemia, a high fasting glucose level, and a low HDL cholesterol level.34 Although some differences were found, our results are in line with those of a previous study suggesting beneficial effects of increasing physical activity on health. In perspectives of abdominal obesity and high blood pressure, the total volume of LTPA in the normal weight group was more than that of abdominal obesity and high blood pressure groups. This finding indicated that performing LTPA might be effective to manage abdominal circumference and blood pressure.
The strength of our study is that it reports results based on a large community-based sample of Koreans and uses long-term (10 years) follow-up data. Many studies have examined associations between physical activity and MetS incidence, although most had a cross-sectional design that could not obtain stronger conclusions of the observed associations on causality.303335363738 Our findings suggest that complying with the 2018 Physical Activity Guidelines for Americans (150–300 minutes of moderate-intensity or 75–150 minutes of vigorous-intensity activity a week) decreases the presence of some MetS components and that performing more than two or three times the minimum recommended activity is essential to maximizing health benefits.
There are some limitations to our study. First, the lack of an association between physical activity and MetS incidence was attributed to the lack of physical activity assessment in household and occupational activities. Therefore, future studies are needed to collect information about everyday physical activities (household, occupational, and lifestyle) to determine the optimal dose of physical activity (intensity, duration, and frequency) for reducing the risk of MetS. However, general household or occupational activities consisting of nondynamic movements do not increase the cardiovascular burden and are insufficient to induce beneficial metabolic or cardiorespiratory effects.39 Additionally, the lack of a significant difference has been attributed to participants who aged more than 60 years and only 30% of them performed LTPA. As a result of this, there was not significant difference in total amount of LTPA between the normal and MetS groups, and multivariate logistic model had limits to clarify association. Second, the mechanisms by which LTPA may reduce the development of MetS are unclear. We collected nine types of LTPAs and assessed the mean volume performed of each. Although we compared the total LTPA volume by type, we found no notable differences except for the effect of swimming on high blood pressure. Third, self-reported questionnaire of physical activity could be considered a potential limitation and possible bias. We had a limitation in the use of standardized intensities because the questionnaire did not cover a detailed description of LTPA. We just used typical standardized MET intensity. For this reason, there could be differences in MET assessment about each of the participants' practical LTPA because of variances in the physical activities performed. Assessing physical activity using wearable devices may be used to measure energy expenditure in the future. Fourth, we used only baseline data for physical activity assessment. Study participants may have changed their LTPA during the follow-up term. The Ansung-Ansan cohort was limited to LTPA measurement at baseline, therefore, we could not analyze LTPA changes with follow up. Fifth, MetS is caused by various factors; therefore, just performing physical activity would not prevent it efficiently. High-carbohydrate diets and food patterns might be associated with MetS.40 Thus, dietary management should remain a focus in MetS intervention.
Our study demonstrated that increasing LTPA was associated with a lower risk of MetS and its components in a 10-year follow-up cohort study of Koreans. The total volume of LTPA impacted the risk of MetS. We suggest that performing more than two times the recommended minimum activity will prevent MetS and aid in health management. Individuals should be encouraged to participate in high LTPA regularly to lower their risk of developing MetS. Further investigations are needed to establish whether overall physical activity, including household, occupational, and other lifestyle activities, can contribute to the prevention of MetS.




 XML Download
XML Download