

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Local anesthesia is commonly used in dental clinics for pain control. For instance, the inferior alveolar nerve block is a useful method to anesthetize the posterior mandibular area.
Needle breakage is a rare complication of inferior alveolar nerve block anesthesia [1]. Its prevalence has decreased with better materials and practitioner training [12].
We report the case a broken needle in the pterygomandibular space, and discuss preventive measures regarding this complication.
CASE REPORT
A 68-year-old woman with a past medical history of hypertension and arrhythmia (on medications) was referred by her dentist to the Department of Oral and Maxillofacial Surgery at Seoul National University Dental Hospital. She was scheduled to undergo implant installation surgery on the left mandibular posterior area in the clinic; however, a needle broke during inferior alveolar nerve block anesthesia. Therefore, she was referred to the hospital for its removal.
The patient was told to stop taking aspirin two weeks prior to her scheduled implant surgery.
A 30-gauge needle was used to anesthetize the left inferior alveolar block. However, the needle was broken in the process. The fragment disappeared into the tissues and the dental clinician was unable to retrieve it. Therefore, the patient was referred to the Department of Oral and Maxillofacial surgery at the university dental hospital. Surgeons failed to remove the needle under general anesthesia using CT (computed tomography) images (Fig. 1A). Next, the patient was referred to our department.
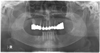
Upon her arrival to our department, the patient was having difficulty opening her mouth because of pain and her previous surgery. Radiographs including a panoramic view (Fig. 1B), a posterior-anterior skull (Fig. 1C) and lateral skull view (Fig. 1D) confirmed that the fractured needle was in the left pterygomandibular space. The panoramic view revealed that the needle was on the posterior border of mandibular ramus. Based on these data, it was decided that surgical exploration under general anesthesia was the most appropriate next step to retrieve the needle.
The patient underwent general anesthesia via nasotracheal intubation. The patient was prepped and draped. In order to gain access, an existing suture was cut and a vertical incision was made along the existing incision from the first surgery. Blunt dissection was used medially along the ramus to expose the pterygomandibular space. A malleable retractor was used to protect the lingual and inferior alveolar nerves. Further exploration of the pterygomandibular space was performed using a microscope. The tip of the needle fragment was identified under the microscope. The broken needle was removed using a hemostat forcep (Fig. 2). This fragment was approximately 20 mm long and bent. No vital structures were injured in the process. The incision was closed using 3-0 and 4-0 Monocryl®. Total intraoperative time was about 2 hours. Postoperative radiographs confirmed that the broken needle had been completely removed (Fig. 3).
The patient recovered well postoperatively, without any pain or numbness. She was still interested in undergoing implant installation surgery. Therefore, she successfully underwent implant installation surgery on the left posterior mandibular area, and was discharged the next day.
DISCUSSION
Although it is possible for a needle to break in the maxillary area, it most often occurs during mandibular inferior alveolar nerve block anesthesia in the pterygomandibular space [23456]. The pterygomandibular space involves several masticatory muscles and the inferior alveolar nerve, which is targeted for inferior alveolar nerve block anesthesia [78]. It is very important to understand the anatomy of this space, not only for successful local anesthesia, but also for troubleshooting complications such as a broken needle.
Radiographic images are important in the localization of a broken needle. In this case, the patient was referred to our hospital several days after the needle was broken. Therefore, 3D CT images had already been taken. Nevertheless, we confirmed the change of location using additional radiographs including the standard panorama, lateral cephalogram, and skull PA images. Finally, the fragment was successfully retrieved under microscope guidance.
Needle breakage is a rare complications of local anesthesia [8]. However when it happens, like in this case, it is not always easily remedied. The retrieval process in this case required a lot of time and money. Therefore, it is important to perform local anesthesia as carefully as possible to avoid such a complication.
As previously mentioned, needles rarely break during local anesthesia because they are disposable and made with high quality material [1910]. In most cases, a needle breaks at the connecting part between the metal and plastic [9]. Therefore, breakage may be a result of poor construction, rather than of material.
Most cases of breakage have occurred with 30-guage short needles [9]. Compared to that of the 27-guage needle, 30-guage needles are less effective for pain relief during needle penetration [9]. Therefore, there are no benefits to using a 30-guage needle, especially for inferior alveolar nerve block anesthesia.
In conclusion, in order to prevent needle breakage during inferior alveolar nerve block, a 27-guage long needle should be used. In addition, it is important to avoid inserting the hub of the needle into the soft tissue.


 XML Download
XML Download